IJCRR - 6(24), December, 2014
Pages: 48-53
Date of Publication: 20-Dec-2014
Print Article
Download XML Download PDF
PREVALENCE OF METALLO BETA LACTAMASE PRODUCING PSEUDOMONAS AERUGINOSA IN HOSPITALIZED PATIENTS
Author: Vineeta Mittal, Fareya Haider
Category: Healthcare
Abstract:Aims: Study the prevalence of multidrug resistant Ps. aeruginosa in hospitalized patients by antibiotic sensitivity test and detection of MBL producing Ps. aeruginosa by two phenotypic methods.
Methods: Total numbers of 83 samples were taken from patients admitted in wards of different departments. Specimens were inoculated on Mac Conkey agar and sheep blood agar. Identification of isolates was done by colony characteristics and biochemical reactions. These isolates were then subjected to susceptibility testing against various antibiotics by Kirby-Bauer disc diffusion test as per CLSI guidelines. Imipenem resistant isolates were selected for the detection of metallo-beta-lactamases production by two phenotypic methods ie Modified Hodge Test and Imipenem-EDTA combined disc test and confirmed by E test
Results: In this study eleven imipenem resistant isolates were found. Out of which six were found positive for MBL by modified Hodge test, Disc synergy test and MBL E test .These MBL positive isolates were mostly from urine samples.
Conclusion: Clinical microbiology laboratories should use proper phenotypic screening methods in all imipenem resistant isolates. In patients admitted in hospital, there should be careful and conservative use of Carbapenems. Most of MBL producing Ps.aeruginosa were isolated from urine specimen coming from surgery wards, so strict vigilance of catheterized operated patients is needed..
Keywords: Carbapenem resistance, Metallo-beta-lactamase, Pseudomonas aeruginosa
Full Text:
INTRODUCTION
Carbapenems are used as last choice for treating serious infections caused by multidrug resistant organisms especially Pseudomonas aeruginosa (Ps.aeruginosa) and Acinetobacter spp . But later on there has been a substantial rise in the reporting of carbapenemase, most notably Metallo β-Lactamases1 . Metallo β lactamase (MBL) belongs to Ambler class B of β-lactamase which requires divalent cations of zinc as cofactors for enzyme activity. They can hydrolyse a wide variety of β-lactams, including penicillins, cephalosporins and carbapenemes.2 MBL-producing Ps.aeruginosa isolates have been reported to be important causes of nosocomial infections across the world. These constitute 20-42 per cent of all nosocomial isolates.3. We undertook this study to determine prevalence of MBL producing Ps. aeruginosa in patients admitted to tertiary care centre over a period of one year.
MATERIAL AND METHOD
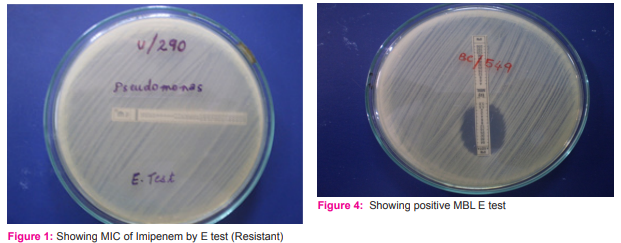
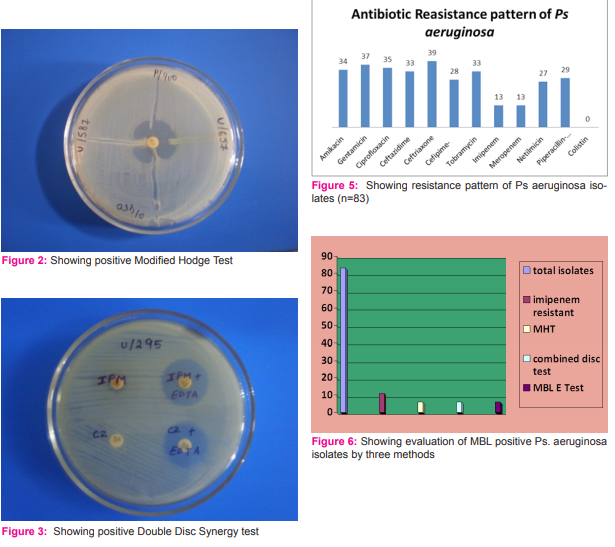
Setting: The study was carried out in the department of microbiology of a tertiary care centre of Lucknow, India. Clinical samples were taken from patients admitted in wards of different departments of a tertiary care centre. Duration of study: One year, from February 2011 to March 2012 Study design: Epidemiological Study Sample size: Total 83 isolates of Ps.aeruginosa were enrolled in one year in this study Selection of subjects: Clinical details were collected from all patients whose culture was positive for Ps.aeruginosa. We included patients who were admitted in the medical and surgical wards and ICU. Information regarding patient’s age, sex, and etiology of disease was noted. Clinical details and history of antibiotic intake at the time of admission were taken. Informed written consent was taken from each patient. Specimen collection: Specimens were processed according to site of lesion e.g. respiratory secretions, swabs pus/ wound, urine, blood culture or CSF. With Universal safety precautions, samples were collected from hospitalized patients, transported and processed in the laboratory without delay. Specimen processing Isolation: Specimens were inoculated on MacConkey agar and sheep blood agar. Plates were seen for growth after 48 hrs of aerobic incubation at 37o C. Blood culture bottle was incubated at 37ºC for 24 hr then subculture on Mac conkey agar and sheep blood agar media on next day and after 7 days. Isolate was gram stained. Identification: Identification of Ps.aeruginosa, was done by biochemical tests as Catalase, Oxidase, Indole, Methyl red, NO3 reduction, Lactose and Maltose. Antibiotic sensitivity test: Antibiotic sensitivity test was done by disk diffusion methods on Mueller- Hinton - agar (Hi-Media, Mumbai) recommended by CLSI incorporating standard stains of P. aeruginosa (ATCC 27853) with the following antibiotics discs amikacin (30 µg), gentamicin (10 µg), netilmicin (30 µg), tobramicin (10 µg)],cephalosporin’s [cefepime (30 µg), ceftazidime (30 µg), ceftriaxone (30 µg)], floroquinolones [ciprofloxacin (5 µg),],carbapenems [imipenem (10 µg), meropenem (10 µg)], and piperacillin/tazobactum (100 µg /10 µg) and colistin (10 µg ). The zone of inhibition was determined after incubation of 24 hours at 37°C. 2. MIC: MICs of Imipenem was determined by E Test (BioMeriux). [Figure 1] Result was recorded after incubation for 18 hrs at 37o C. Eleven Imipenem resistant isolates showed MIC > 4 µg/ml which is resistant according to CLSI guidelines 2012. 4 3. MBL identification: All Imipenem resistant isolates were screened for carbapenemase by modified Hodge test and for MBL production by double disc synergy test. MBL production was confirmed by E test. A. Modified Hodge test5 Modified Hodge test was carried out on Mueller -Hinton agar. The plate was inoculated using a cotton swab dipped in an overnight culture suspension of E.coli ATCC25922. (Opacity of the tube was adjusted by comparing with a 1:10 dilution of 0.5 McFarland opacity standards). After brief drying, 10 µg imipenem disc was placed at the center of the plate and test strain was streaked from the edge of the disc to the periphery of the plate in four different directions. After overnight incubation the plates was observed for the presence of a clover leaf of shape zone of inhibition. The plates with such zones were interpreted as Modified Hodge test positive. [Figure 2] B. Zone enhancement with EDTA (Double Disc Synergy test)5 Impregnated imipenem and Ceftazidime Discs: Ps.aeruginosa was inoculated on to plates with Muller-Hinton agar as recommended by CLSI. A 0.5 m EDTA.2H2 O mix in 1000 ml of distilled water and adjust it to pH 8.0 by using NaOH. The mixture was sterilized by autoclaving. Two 10 µg imipenem discs and two-30µg ceftazidime disc was placed on the surface of an agar plate and EDTA solution was added to one of them to obtain a desired concentration of 750µg. The inhibition zone of imipenem, ceftazidime, and imipenem EDTA and ceftazidime EDTA disks were compared after 16-18 hrs of incubation at 35 º C.[Figure 3] C. MBL E test (HiMedia) E-test metallo-beta-lactamase strips (Hi Media) consist of a double sided seven dilution range of imipenem IP (4 -256 µg/ml) and IP (1 - 64 µg/ml) overlaid with a constant gradient of EDTA. Individual colonies were picked from overnight agar plates and suspended in 0.85% saline to a turbidity of 0.5% McFarland’s standards. A sterile cotton swab was dipped into the inoculum suspension. The excess moisture was allowed to be absorbed for about 15 min before the MBL E-test strip was applied. Plates were incubated for 16 to 18 hrs at 37°C. The MIC end points were read where the inhibition ellipses intersected the strip. When the ratio of the value obtained for Imipenem (IPM): the value of IPM + EDTA is more than 8 or zone was observed on the side coated with IPM+EDTA and no zone was observed on the opposite side created with IPM, the culture was interpreted as MBL positive. [Figure 4] Ethics: The study was carried out after approval with institutional review board and taking informed consent. Statistical analysis: Statistical analysis was done by Gaussian test of proportion and Fisher’s exact test.
RESULTS
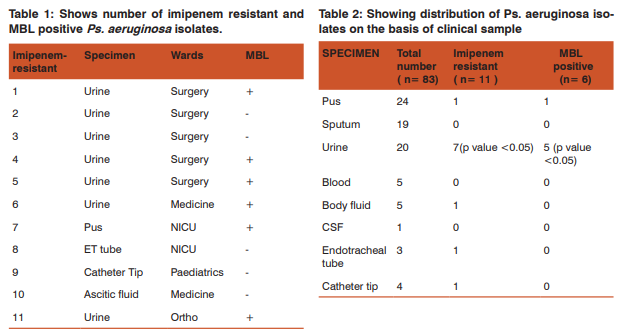
In our study 83 Ps. aeruginosa strains were isolated from various clinical specimens which were identified by biochemical methods. These Ps. aeruginosa isolates showed resistance to even the most recent antibiotics like third generation cephalosporins, antipseudomonal penicillins, aminoglycosides and flouroquinolones. In this study, around 22 isolates (26.5%) were MDR ie. resistant to all antibiotics. Colistin was most effective antibiotic recording 0% resistance. Ceftazidine, antipseudomonal reserve drug was found 33% resistant in this study. Another drug is piperacillintazobactum .We observed 29% resistant against this drug. Among aminoglycosides Netilmycin showed least resistance (27%) as compared to tobramycin (33%), amikacin (34%) and Gentamycin (37%). Quinolone, particularly ciprofloxacin was sensitive in 65% of Ps. aeruginosa. [Figure 5] In this study carbapenem resistance was found in eleven (13%) isolates. All the eleven imipenem resistant isolates were resistant to most of the antimicrobials tested including Amikacin, Gentamicin, Ciprofloxacin, Ceftriaxone, Ceftazidime, Cefipime, Tobramycin, Netilmycin and Pipercillin- tazobactum. MIC of Imipenem by E test was done. Complete correlation with dilution and diffusion method was found. In these eleven imipenem resistant isolates, six were positive for MBL by Modified Hodge test, and Imipenem -EDTA disc synergy tests, Ceftazidime EDTA disc synergy tests and five negative by all tests. These six isolates were found positive by MBL E test (Hi Media) for MBL production. DISCUSSION Ps. aeruginosa is a pathogen associated with numerous nosocomial infections in immuno compromised patients. Ps. aeruginosa strains are intrinsically resistant to various antimicrobial agents. Nowdays, Ps. aeruginosa isolates are resistance to the most recent antibiotics also. . In this study, 22 out of 83 isolates were resistant to all antibiotics except colistin which is major concern emerging from our study. Carbapenems are the drugs of choice for multidrug resistant Ps. aeruginosa and ESBL producing organisms. However, resistance to carbapenems due to reduced uptake of drug leads to imipenem/meropenem resistant isolates.6 In this study carbapenem resistance was found in 13% isolates and all the 11 imipenem resistant isolates were MDR. In this study most of the carbapenem resistance isolates were from surgery wards followed by NICU, medicine ward. [Table1] Ps. aeruginosa producing MBL was first reported from Japan in 1991.7 Navneeth et al 8 reported MBL production in Ps. aeruginosa first time from India in 2002. They reported 12% prevalence of MBL producing Ps. aeruginosa. In other studies of India prevalence ranging from 8 to 14% has been reported.9-11. In this study the overall prevalence of MBL positives Ps. aeruginosa was 7.23%. There are various methods by which MBL production can be identified. In which PCR is most sensitive and accurate method but PCR can identify specific type of MBL only and PCR could not be done in all laboratories due to its cost effectiveness. So different phenotypic methods are useful for MBL detection like modified Hodge test, imipenem-EDTA combined disk test, double-disk synergy test using imipenem or ceftazidime and EDTA and E-test.5, 12-13, In this study we used three different methods for detection of MBL producing Ps. aeruginosa; Modified Hodge test, Double disk synergy test by Imipenem and Ceftazidime with EDTA and MBL- E-test.[Figure 6] A total of 83 strains were isolated in this study over a period of one year. Eleven (13.25%) were resistant to Imipenem and six (7.23%) were found to be MBL producers by Double disk synergy test. In this study all the six isolates gave MBL positive results by both ImipenemEDTA disc synergy test and Ceftazidime EDTA disc synergy test. Bashir etal 14 showed different results by both methods in their study. This study is more or less similar to study conducted by Behera200812 who reported 14.47% imipenem resistances and 10.52% MBL production in Ps. aeruginosa. All the six isolates on which MBL-E-test was performed were MBL positive. Thus 100% positive results were obtained in this study which is comparable to various studies. In other studies, E test had a sensitivity of 92% 15 and 96% 16 in detecting MBL. Behra etal found 100% positivity by E test.12 In this study we screened carbapenem resistant isolates only which might have accounted for very high sensitivity of the test. Double disk synergy test and E-test were found to be equally sensitive in detecting MBL positive isolates. E-test is a simple screening test and can be performed along with routine susceptibility testing. The maximum number of MBL positive isolates were obtained from urine (85%) followed by pus swab (15%). Hirakata et al. (1998)11 reported in their study that the predominant source of isolation for MBL positive Ps. aeruginosa was urinary tract (40.0%) followed by respiratory tract (18.8%) and abscesses, pus and wounds (15%) .In the present study 6.02% MBL positive isolates were recovered from urine (85% of total MBL positive isolates) and the association was statistically significant. [Table 2] Most of these patients were having indwelling urinary catheter. This finding is consistent with another study reported by Hirakata et al. (2003). 16 MBL producing isolates are associated with a higher morbidity and mortality. Moreover given the fact that MBLs will hydrolyze all classes of ß-lactams and that were several years away from the development of a safe therapeutic antibiotic; their continued spread would be a clinical disaster.13 The occurrence of an MBL positive isolate poses not only a therapeutic problem but is also a serious concern for infection control management. As a result of being difficult to detect, such organisms pose significant risks particularly due to their role in unnoticed spread within institutions and their ability to participate in horizontal MBL gene transfer, with other pathogens in the hospital.17 In this study also, all the patients having MBL positive Ps. aeruginosa showed severe morbidity and did not recover well and were shifted to higher tertiary centre.
CONCLUSION
Clinical microbiology laboratories should use proper phenotypic screening methods in all imipenem resistant isolates. In patients admitted in hospital, there should be careful and conservative use of Carbapenems. Most of MBL producing Ps.aeruginosa were isolated from urine specimen coming from surgery wards, so strict vigilance of catheterized operated patients is needed.
References:
1. Gladstone P, Rajendran P, Brahmadathan KN. Incidence of carbapenem resistant nonfermenting Gram negative bacilli from patients with respiratory infections in the intensive care unit. Indian J Med Microbiol2005; 23: 189-91.
2. Bush K, Jacoby GA, Medeiros A. A functional classification scheme for beta lactamase and its correlation with molecular structure. Antimicrob Agents Chemother1995; 39: 1211-33.
3. Walsh TR, Toleman MA, Poirel L, Nordmann P. Metallob-lactamase: the Quiet before the Storm? ClinMicrobiol Rev2005; 18: 306-25.
4. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing; Twenty second informational supplement. CLSI document2012; M100-S22, 32(3).
5. Lee K, Lim YS, Yong D, Yum JH, Chong Y. Evaluation of Hodge test and the imipenem-EDTA double-disk synergy test for differentiating metallo-ß-lactamase producing isolates of Pseudomonas spp. and Acinetobacter spp. J ClinMicrobiol2003; 41: 4623-4629.
6. Bonfiglio G, Laksai Y, Franchino L, Amicosante G, Nicoletti G. Mechanisms of b-lactam resistance amongst Pseudomonasaeruginosaisolated in an Italian survey. J AntimicrobChemother1998; 42: 697-702.
7. Shashikala, Kanungo R, Srinivasan S, Devi S. Emerging resistance to carbapenem in hospital acquired Pseudomonas infection: A cause of concern. Indian J Pharmacol2006; 38: 287-8.
8. Navaneeth BV, Sridaran D, Sahay D, Belwadi MR. A preliminary study on metallo beta-lactamase producing Pseudomonas aeruginosa in hospitalized patients. Indian J Med. Res2002; 116: 264-267
9. Zavascki AP, Barth AL, Gaspareto PB, Goncalvez AL, Moro AL, Fernandes JF, Goldani LZ. Risk factors for nosocomial infections due to Pseudomonas aeruginosaproducing metallo-betalactamase in two tertiary care teaching hospitals. J AntimicrobChemother2006; 58: 882-885.
10. Varaiya A, Kulkarni N, Kulkarni M, Bhalekar P, Dogra J. Incidence of metallo-beta-lactamase producing Pseudomonasaeruginosain ICU. Indian J Med Res2008; 127: 398-402.
11. Hirakata Y, Izumikawa K, Yamaguchi T, Takemura H, Tanaka H, Yoshida R. Rapid detection and evaluation of clinical characteristics of emerging multi-drug resistant gramnegative rods carrying metallo-ß-lactamase gene blaIMP. Antimicrob Agents Chemother1998; 42: 2006-2011.
12. Behera B, Mathur P, Das A, Kapil A, Sharma V. An evaluation of four different phenotypic techniques for detection of metallo-betalactamase producing Pseudomonas aeruginosa. Indian J MedMicrobiol 2008; 26: 233-237.
13. Yong D, Lee K, Yum JH, Shin HB, Rossolini GM, Chong Y. Imipenem-EDTA disk method for differentiation of metallo-ßlactamase producing clinical isolates of Pseudomonas spp. AndAcinetobacter spp. J ClinMicrobiol2002; 40: 3798- 3801
14. Bashir D, Thokar MA, Fomda BA, Bashir G, Zahoor D, Ahmad S and Toboli AS. Detection of metallo-beta-lactamase (MBL) producing Pseudomonas aeruginosaat a tertiary care hospital in Kashmir. African Journal of Microbiology Research 2011;5(2):164-172
15. Pitout J, Gregson DB, Poirel L, McClure JA, Le P, Church DL. Detection of Pseudomonas aeruginosaproducing metalloßlactamases in a large centralized laboratory. J ClinMicrobiol2005; 43: 3129-3135.
16. Hirakata Y, Yamaguchi T, Nakano M, Izumikawa K, Mine M, Aoki S. Clinical and bacteriological characteristics of IMP-type metallo-beta-lactamase producing Pseudomonas aeruginosa. Clin Infect Dis2003; 37: 26-32.
17. Agarwal VA, Dongre SA, Powar RM. Antimicrobial resistance profile of Pseudomonas aeruginosaproducing metallo-betalactamase. Indian J Med Res2006; 124: 588-590.,
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





