IJCRR - 6(24), December, 2014
Pages: 19-23
Date of Publication: 20-Dec-2014
Print Article
Download XML Download PDF
ELECTIVE SURGICAL CASE CANCELLATION - AN AUDIT
Author: Nikhil Nanjappa B. A., Kirti Katherine Kabeer, S. Robinson Smile
Category: Healthcare
Abstract:Background: Elective surgical case cancellation refers to any surgical case that is booked into the operation theatre list on the day prior to surgery, but is not operated upon as scheduled [1]. The reasons for cancellation of elective surgical cases are many; they are as unique as they are similar. Aims and Objectives: The study aims to assess the magnitude of elective case cancellation at our hospital. This study tries to delineate the reasons for elective case cancellations across all surgical departments. The study aims to suggest necessary steps to alleviate the problem. Methodology: This is a prospective observational hospital based audit done between 23rd February 2012 and 5th May 2012. Observations and Results: The total number of elective cases booked into the operative list during the study period was 725, of which 197 (27.2%) was cancelled on the day of surgery. General surgery had the highest percentage share of total cancellations at 54.8%, followed by obstetrics gynecology (16.2%), orthopedics (13.1%), ENT (9.1%), urology (3.5%), pediatric surgery (2%), CTVS and neurosurgery (0.5% each). There were 9 cases that were cancelled more than once. They commonest reason for case cancellation was list over run (73%), followed by lack of patient fitness (14%). Discussion: Case cancellations on the day of surgery lead to underuse of OT's, increases waiting period for the patients, frustration and mental stress to the patients and their families, and increases cost and wastage of hospital consumables [1-6]. Cancellation of booked elective surgeries is a common problem across all hospitals in our country and around the world. The incidence of cancellation of elective surgical operations has been reported in literature to range from 20% to 40% [3, 5, 7-10]. Improving the scheduling and admission procedure is of paramount for better use of hospital resources [16].
Keywords: Surgical case, CTVS, Neurosurgery
Full Text:
INTRODUCTION
The operation theatre, among the surgical staff is regarded as the heart and soul of the hospital. Most hospital administrators agree that a considerable allocation of resources is made for the proper functioning of the operating room (OR). Also, it is the operation theatre that generates a substantial part of the hospital revenue. Elective surgical case cancellation refers to any surgical case that is booked into the operation theatre list on the day prior to surgery, but is not operated upon as scheduled [1]. The reasons for cancellation of elective surgical cases are many; they are as unique as they are similar. Unexpected OR cancellations are usually divided into avoidable cancellations (e.g., scheduling errors, equipment shortages, list overrun, and cancellation due to inadequate preoperative evaluation) and unavoidable cancellations (e.g., emergency case superseding the elective schedule, unexpected changes in the patient’s medical status, or patient nonappearance)[1]. The most common factor that leads to cancellation is lack of OR time [1]. The cancellation of patients from elective theatre operating lists considerably increases cost, duplicates workload, decreases efficiency and wastes operating room time [2, 3]. The major brunt of case cancellation is borne by the patients and their families. It causes significant emotional trauma to the patients as well as their families [4]. Elective surgery cancellations will directly and indirectly increase the patients’ treatment expenses due to longer hospital stay and in many cases, repetitions of pre-operative preparations and management [5, 6]. Repeat cancellations result in poor patient satisfaction, staff morale, hospitalpatient relationship and training [3, 5, 6]. The incidence of cancellation of elective surgical operations has been reported in literature to range from 20% to 40% [3, 5, 7-10]. With the end objective to reduce the number of case cancellations in our hospital, the first step would be to assess the magnitude of the problem.
AIMS AND OBJECTIVES
1. To assess the magnitude of elective case cancellation at our hospital.
2. To study and evaluate reasons for elective case cancellations across all surgical departments.
3. To suggest necessary steps to alleviate the problem.
METHODOLOGY
This was a prospective observational hospital based audit done between 23rd February 2012 and 5th May 2012. All elective cases cancelled on the day of surgery from the departments of General Surgery, Orthopedics, Obstetrics and Gynecology, ENT, Pediatric Surgery, Cardiovascular and Thoracic Surgery (CTVS), Urology and Neurosurgery during the study period were included. At Mahatma Gandhi Medical College and Research Institute, we have 10 elective theatres that function six days of the week (Monday-Saturday) from 8:30 AM to 2 PM, and one Emergency theatre common to all departments that functions 24hours a day, 7 days of the week. Of the 10 elective theatres, two are allotted to General Surgery, two to Orthopedics, one that is shared between Urology and Pediatrics, one between OMFS and ENT, one between CTVS and Neurosurgery and three for Obstetrics and Gynecology. The anesthetist in the pre-anesthetic check-up room assesses all elective cases on the previous day. Cases that are provisionally cleared for surgery will then be entered in the OT booking list. A copy of this list will be sent to the Anesthetic department and to the respective ward. The concerned anesthetist in charge of a particular OT for the next day, follow up these cases in the ward, the evening prior to the surgery. A list of all cancelled cases on the day of surgery were studied and analyzed by a surgical resident. Case cancellation of individual departments were taken into account and each case was allotted into one of the 13 causes for case cancellations which are patient unfit, operation not necessary, list over run, patient unwilling, attender not available, patient not fasted, procedure done in ward, staff not available, equipment/consumable problem, patient not affordable, blood not available, list interrupted by emergency and strikes caused by the hospital staff for various reasons.
OBSERVATIONS AND RESULTS
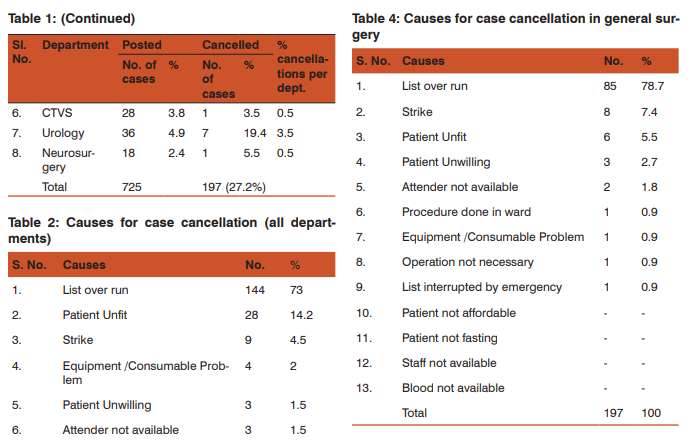
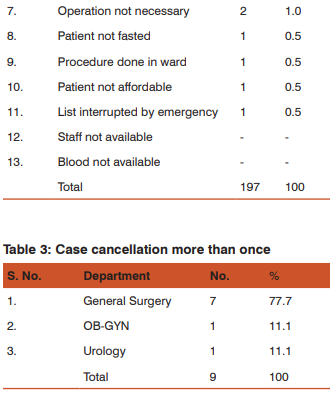
Total number of elective surgical cases posted for surgery during the study period was 725 in 61 working days. The mean was 11.9 elective cases per working day across all surgical departments. General surgery had maximum cases during the study period, accounting for 40.9%, followed by Obstetrics and Gynecology 19.8%, Orthopedics 15.1%, ENT 8.9%, Urology 4.9%, CTVS 3.8%, pediatric surgery 3.7% and neurosurgery 2.4%. [Table 1] The total number of cases cancelled was 197 (27.2%). The number of cases cancelled by individual departments is summarized in this section. Department of general surgery had the highest rate of cancellations, i.e. 36.3% of their 297 elective cases posted during the study period, followed by ENT (27.6%), orthopedics (23.6%), obstetrics and gynecology (22.2%), urology (19.4%), pediatric surgery (14.8%), neurosurgery (5.5%) and CTVS (3.5%). [Table 1] General surgery also had the highest percentage share of total cancellations at 54.8%, followed by obstetrics gynecology (16.2%), orthopedics (13.1%), ENT (9.1%), urology (3.5%), pediatric surgery (2%), CTVS and neurosurgery (0.5% each). [Table 1] The most common reason stated for case cancellation was list over run (73%), followed by patient being unfit for surgery (14.2%), strikes (4.5%). The other reasons contributed to a very small share and are listed on table 2. Surgeries for 9 of 197 patients were cancelled on more than one occasion. General surgery had 7 such incidents, followed by obstetrics gynecology and urology with 1 each. [Table 3] The reasons for case cancellation was studied separately for the department of general surgery, as it the highest share of cancellations. The commonest reason was list over run at 78.7%, followed by strikes (7.4%), patient unfit (5.5%), among other causes listed in table 4.

DISCUSSION
Elective surgical operations require a multidisciplinary approach between surgical team, hospital staff and hospital administration. Case cancellations on the day of surgery lead to underuse of OT’s, increases waiting period for the patients, frustration and mental stress to the patients and their families, and increases cost and wastage of hospital consumables [1-6]. Cancellation of booked elective surgeries is a common problem across all hospitals in our country and around the world. The cancellation rates vary significantly in various reports. The incidence of cancellation of elective surgical operations has been reported in literature to range from 20% to 40% [3, 5, 7-10]. In our study we had case cancellation of 27.2%. Though the number seems high, it is within range that is reported from most developing countries. Interestingly, the rates in developed countries are not significantly lower. The reasons for case cancellation are as varied as they are unique to each hospital. The reasons are usually categorized as modifiable and non-modifiable. Increased bed usage by medical specialties is one important factor [9]. Lack of theatre space and facilities have been cited as reasons by many researchers [5, 8, 14]. Cancellations of elective operations due to patient related factors accounted for 6.2% of cases. The most common reason for this was financial constraints [14]. “No show up of patients was the leading cause of cancellations in elective surgery” [1]. However, in our hospital day care surgery doesn’t contribute to significant proportion of elective cases, and patient ‘no show’ wasn’t a problem in our hospital. Other miscellaneous reasons are inadvertent discharge of the patient, non-fasting, anaphylactic shock, patient refused surgery, patients with prolonged coagulation profile [1]. In our study the single most important reason for case cancellation was ‘list over run’. It accounted for nearly three quarters of all case cancelations. Being a teaching hospital, most surgeries take longer to perform, as both surgical and anesthesiology residents are being mentored during the surgeries and this contributes to ‘list over run’. The scenario is common all teaching hospitals across the country and around the world. The most common cause for case cancellations on the day of surgery in all departments studied is due to list over run (73%), General Surgery having the most number of cancellations. Chalya et. al observed that case cancellations due to list over run were often due to surgeons underestimating the operating time required per case and also depended on the performing surgeon (less experienced surgeons/trainees) [14]. ‘List over run’, was followed by ‘patient unfit’. The reasons for this could vary from poor glycemic control, inadequately control of blood pressure, dyselectrolytemia, etc. In our study, the highest cancellation rate was in the general surgery department. 36.8% of all booked elective cases were cancelled. General surgery accounted for 54.8% of all case cancellations at our hospital during the study period. At distant second and third were departments’ of obstetrics and gynecology and orthopedics. The least number of cancellations were in departments of CTVS and neurosurgery. A study from Tanzania also found that most cancellations were in the general surgery section followed by orthopedic surgery and otorhinolaryngology, and the least cancellation was in the ophthalmology and cardiothoracic sections [14]. However, three other studies reported higher cancellation rate among the urology, orthopedics and gynecology than in general surgery [7, 15, 16]. Department of general surgery performs nearly 40% of all elective surgeries in our hospital; and also has the highest number of resident surgeons; hence the result was not very surprising. The commonest reason for case cancellation in the department was also ‘list over run’. General surgery also had the highest proportion of repeat cancellations (7/9), needless to say that repeat cancellations multiply patient anxiety, stress and financial burden. The cancellation of surgery creates untold hardship for patients who plan their working and family lives around the proposed operation date. Most are cancelled at less than 24 hours notice [13]. The cost implications to the community are immense but have not been calculated. Cancellations of elective operations due to lack of theatre space and theatre facilities can be prevented through careful planning and efficient utilization of the already limited hospital resources including the operating room, theatre facilities and valuable manpower. Improving the scheduling and admission procedure is of paramount for better use of hospital resources [16].
ACKNOWLEDGEMENTS
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Dawlatly AA, Turkistani A, Aldohayan A, Zubaidi A, Ahmed A. Reasons of Cancellation of Elective Surgery in a Teaching Hospital. Intern J Anesthesiol. 2008;15:2.
2. Zafar A, Mufti TS, Griffin S, Ahmed S, Cancelled elective general operations in Ayub Teaching hospital. J. Ayub Med Coll Abbollabad 2007; 19 (3): 64-66.
3. Robb WB, O’Sullivan MJ, Brannigan AE, Bouchier-Hayes DJ. Are elective surgical operations cancelled due to increasing medical admissions? Irish J Med Sci. 2004;173(3):129.
4. Miller GG. Waiting for an operation: parent’s perspectives. Can J Surg 2004; 47(3):167-9. and Kolawole I.K., Bolaji B.O. Reasons for cancellation of elective surgery in Ilorin. Nig .J Surg. Res 2002; 4 (1-2): 28-33.
5. Ojo E.O., Ihezue C.H. An Audit of Day Case Cancellations In A Nigerian Tertiary Hospital Based Day Case Unit East and Central African Journal of Surgery 2008; 13 (2); 150- 153.
6. Kolawole I.K., Bolaji B.O. Reasons for cancellation of elective surgery in Ilorin. Nig .J Surg. Res 2002; 4 (1-2): 28-33.
7. Lacqua MJ, Evans JT. Cancelled elective surgery: an evaluation. American Surgeon 1994;60:809-11.
8. Rai M, Pandit JJ. Day of surgery cancellation after nurse led pre-assessment in an elective surgical centre: the first 2 years. Anesthesia 2003; 58:692-9.
9. Dakum N. K., Ramyil V. M, Misauno M. A., Ojo E.O., Ogwuche E. I., Sani A. A. Reasons for cancellations of urologic day care surgery. Nigerian of Surgical Research 2006; 8 (1 – 2): 30- 33.
10. El-Bushra A.D., Mohamed I.M., Awadalla M.A., Mohamed Y.B., Salah E.M. Cancelled elective surgical operations at El Obeid Hospital, Western Sudan. Sudan Med. J. 2008; 44 (1, 2 and 3):56-61
11. Are elective surgical operations cancelled due to increasing medical admissions? Robb WB, O’Sullivan MJ, Brannigan AE, Bouchier-Hayes DJ. Ir J Med Sci. 2004 JulSep;173(3):129-32.
12. Elective surgery--cancellations, ring fencing and efficiency. Aaserud M, Trommald M, Boynton J. Tidsskr Nor Laegeforen. 2001 Sep 10;121(21):2516-9.
13. Impact of emergency admissions on elective surgical workload. Nasr A, Reichardt K, Fitzgerald K, Arumugusamy M, Keeling P, Walsh TN. Ir J Med Sci. 2004 JulSep;173(3):133-5.
14. Chalya PL, Gilyoma JM, Mabula JB, Simbila S, Ngayomela IH, Chandika AB, Mahalu W. Incidence, causes and pattern of cancellation of Elective surgical operations in a University Teaching Hospital in the Lake Zone, Tanzania. African Health Sciences Vol 11 No 3 September2011: 438-43.
15. Jonnalagadda R, Walrond ER, Marinara S, et al. Evaluation of the reasons for cancellations and delays of surgical procedures in a developing country. Int Clin Pract. 2005;59:716–720.
16. Venkartaraman S, Seriam K. Cancelled elective surgery: study in an Indian Corporate Hospital. Indian Surg. 1997;59:372–376.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





