IJCRR - 6(24), December, 2014
Pages: 01-06
Date of Publication: 20-Dec-2014
Print Article
Download XML Download PDF
VESICOURETERAL REFLUX - PRESENTATION AND MANAGEMENT AMONG CHILDREN AT A TERTIARY CARE HOSPITAL IN SOUTHWESTERN REGION, SAUDI ARABIA
Author: Abdullah A. Muzallef, Ali M. Alsuheel, Ayed A. Shati, Saleh M. Al-Qahtani, Zainah A. Sabr, Safa M. Al-Haider, Ahmed H. Almathami
Category: Healthcare
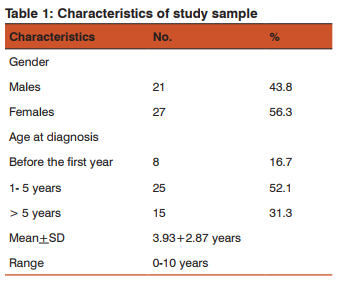
Abstract:Objective: Studying the medically and surgically outcome of Vesicoureteral reflux among pediatric patients in Aseer region. Methodology: This is a retrospective study. We reviewed and analyzed all files for VUR patients who attended the Aseer Central Hospital (ACH) during the period from January 2007 till December 2011. A total of 48 VUR patients were registered. Results: More than half of children with VUR were females (56.3%). The age of these cases ranged from one month to 10 years. Most of these cases were diagnosed at the age of 1-5 years (52.1%), with a mean +SD of 3.93+2.87 years. Conclusions: VUR affects girls more than boys in Aseer Region, starting as early as the first days of life, indicating its congenital etiology. The main presentation for these children is UTI.
Keywords: Vesicoureteral reflux, Children, Endoscopic deflux injection, Aseer, KSA
Full Text:
INTRODUCTION
The Vesicoureteral reflux (VUR) is the retrograde flow of urine from the bladder into the ureter and possibly the kidney according to the grade. Primary VUR is congenital and is not associated with any underling neuromuscular or obstructive phenomena,1 and is usually detected during radiological evaluation of children with urinary tract infection (UTI).2 While in secondary VUR the valvular mechanism is intact and healthy to start with but becomes overwhelmed by raised vesicular pressures associated with obstruction, which distorts the ureterovesical junction. The obstructions may be anatomical or functional. The cause of VUR is a developmental anomaly resulting in an inadequate length of the intravesical submucosal ureter.2 A substantial number of children also have dysfunctional voiding, which may initiate or perpetuate VUR.3 VUR is believed to be present in 1% or less of normal children. Most cases of VUR are diagnosed after occurrence of a UTI. Pediatric clinical practice guidelines recommend screening children for VUR after a UTI.4 In the first seven years, 1.7% of boys and 7.8% of girls have a UTI. Most occur in the first year with a male predominance in the first six months. In uncircumcised boys there is a 10-fold increased incidence.5 Children who have a UTI have a high incidence of VUR, which indicates that VUR predisposes patients to UTI.6 In addition, children who have a UTI and VUR are more likely to have evidence of renal involvement than children without VUR who have a UTI. The principal complications of renal scarring are chronic renal failure and hypertension.7 So, the proper management of VUR should be based on preventing these complications.4 The insult caused by VUR can either be due to the intrusion of infected urine into the renal substance, and this is the most commonly accepted danger related to VUR, or can be due to the abnormal urine pressure exerted by reflux on the papillae, or to abnormal biochemical or immunological reactions caused by the presence of bladder urine in the renal parenchyma. Not one but four factors may play a role in the pathophysiology of VUR: the virulence of bacteria and their reservoirs, incompetent vesico-ureteric junction, renal parenchyma and bladder and bowels dysfunctions.8
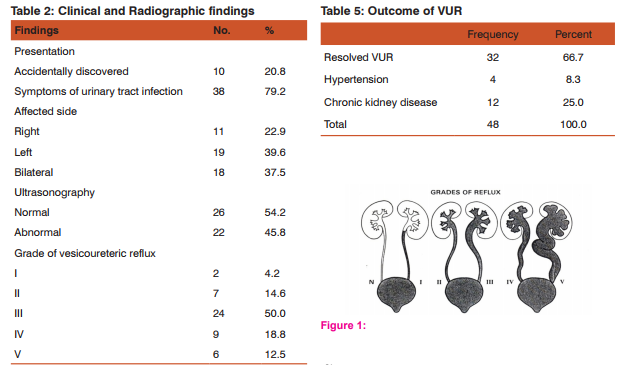
Scar formation in children with VUR after UTIs is an important cause of secondary hypertension and can cause chronic renal failure. Risk factors for renal scar formation include higher grade VUR and delay in UTI diagnosis and treatment. The use of prophylactic antibiotics to prevent UTIs also may decrease the risk of scar formation.7 This study aims to identify the pattern of VUR, outcome after deflux injection and antibiotic prophylaxis and complications of VUR among the children population of Aseer Region, Kingdom of Saudi Arabia (KSA) as single center study. MATERIAL AND METHODS This is a retrospective study. We reviewed and analyzed all files for VUR patients who attended the Aseer Central Hospital (ACH) during the period from January 2007 till December 2011. A total of 48 VUR patients were registered. Voiding cystourethrography (VCUG) was used to confirm the diagnosis of VUR. A dimercaptosuccinic acid (DMSA) renal scan is used to evaluate for any renal scar. Until the reflux resolves or the reflux is surgically treated, the patient should undergo monitoring with cystography (VCUG) every 12-24 months.9 Aseer Central Hospital (ACH) is the tertiary care hospital that serves all referred patients in Aseer Area. VUR was graded according to Dähnert as follows:10 • Grade I: Urine backs up into the ureter only, and the renal pelvis appears healthy, with sharp calyces. • Grade II: Urine backs up into the ureter, renal pelvis, and calyces. The renal pelvis appears healthy and has sharp calyces. • Grade III: Urine backs up into the ureter and collecting system. The ureter and pelvis appear mildly dilated, and the calyces are mildly blunted. • Grade IV: Urine backs up into the ureter and collecting system. The ureter and pelvis appear moderately dilated, and the calyces are moderately blunted. • Grade V: Urine backs up into the ureter and collecting system. The pelvis is severely dilated, the ureter appears tortuous, and the calyces are severely blunted, see (Figure -1).
RESULTS
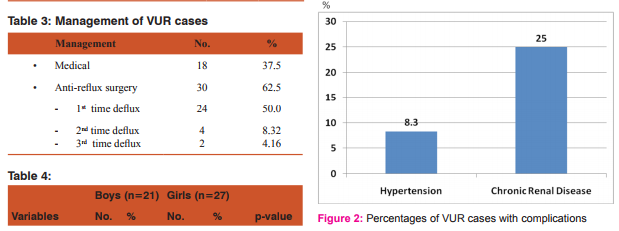
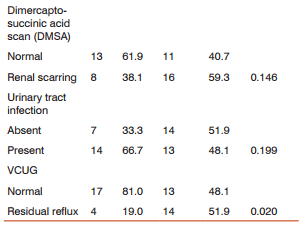
More than half of children with VUR were females (56.3%). The age of these cases ranged from one month to 10 years. Most of these cases were diagnosed at the age of 1-5 years (52.1%), with a mean +SD of 3.93+2.87 years, as shown in Table (1). Presentation was mainly symptoms of UTI (79.2%) and the rest was accidentally discovered to have VUR who were diagnosed to have hydronephrosis antenatally. The left side was more affected (39.6%) than the right side (22.9%). However, 37.5% of cases had bilateral VUR. Half of cases had grade III VUR (50%), while 18.8% had grade IV and 12.5% had grade V. Ultrasonography showed abnormal findings in 45.8% as a first tool for screening which was showing hydronephrosis. About one third of cases were managed medically (37.5%) by using antibiotics prophylaxis alone (amoxicillin was used for infant less than 6 weeks and co-trimoxazole for whom older than 6 weeks), while 62.5% were managed medically by using antibiotics prophylaxis and surgically by injecting bulking agent (deflux) underneath the intravesical portion of the ureter in a submucosal location, either once (50%) or more than once (12.5%), as shown in Table(3). Patients who required deflux injection more than once were having neurogenic bladder, three of them was due to mylomeningocele and others were idiopathic. All patients were continued on antibiotics and outpatient follow-up. VCUG and renal scan were done during follow up after 6-12 months from the procedure date. VCUG showed residual reflux in 37.5% of cases. DMSA revealed renal scarring in 50% of cases. Chronic kidney disease was present in 25% (12) in form of proteinuria and rising of urea and creatinine, and 8.3% (4) were hypertensive, as shown in figure (1). Comparing the male patients with female patients revealed a higher prevalence of renal scarring among females than males (59.3% vs. 38.1%, respectively). Incidence of recurrent UTI was higher among males (66.7%) than females (48.1%) after Deflux. Voiding cystourethrogram (VCUG) showed a significantly higher prevalence of reflux among females than males (51.9% vs. 19%, respectively, p=0.020), as shown in Table (4).
DISCUSSION
VUR is a congenital abnormality, which affects approximately 1% of infants and children. It may predispose a child with UTI to the development of pyelonephritis, which may lead to renal scarring and hypertension.11 It is the most common hereditary disorder of the genitourinary tract and some transmitted in an autosomal dominant fashion.12 This study showed an early age at diagnosis of VUR (mean age is 3.93 years) and also the more incidence among girls (56.3%) than boys (43.7%). These findings in Aseer, KSA are similar to those reported in other countries. Sharbaf et al. (2007), in Iran, reported a mean age at VUR diagnosis of 4.1 years, with a range from 54 days to 16 years and the male-to-female ratio was 0.21 (girls were 262 while boys were 57). Leroy et al. in England, studied 117 VUR children (age range, 0.0–13.9 years) of whom, 46 (39.3%) were boys and 71 (60.7%) were girls.13 Greenbaum and Mesrobian noted that girls are more commonly diagnosed with VUR because they are more likely to have a UTI.5 Wald explained the early presentation of VUR cases by its congenital nature. He added that these cases can be diagnosed in utero by ultrasonography.14 Experimental studies suggest that abnormal insertion of the ureteral bud could induce abnormal differentiation of metanephros (“renal dysplasia”).8 Smellie et al. added that VUR has a natural tendency to resolve as the intravesical part of the ureter lengthens with growth. By age 10 about 75% of VUR has resolved.15 This study showed that the main presentation for VUR cases was that of UTI (79.2%). This finding is in accordance with that reported by several authors. VUR and UTI are often associated. 16 Eighty eight percent of urine culture performed in children with VUR have sterile urine at the time of diagnosis which does not confirm that UTI causes VUR, and 60% of febrile UTI have no demonstrable VUR. Mild VUR does not increase the incidence of UTI, pyelonephritis, or renal scarring after acute pyelonephritis.17 Williams et al. stated that VUR is diagnosed in 20-30% of children with a first UTI.18 Godley noted that VUR and UTI seem to be independent pathological factors that may potentiate each other.16 The main infection pathway is the ascent from the lower to the upper urinary tract although rarely demonstrated. Other pathways have been suggested such as hematogenous or lymphatic, but none have been validated yet.8 Results of this study indicated that VUR affected the left side more than the right side, while, 37.5% of VUR cases were bilateral. This is in accordance with that reported by Jang et al., who found that 32% of VUR cases occurred on the left side, 27.9% were on the right side while 41.1% were bilaterally affected.19 This study revealed that 4.2% of VUR cases had grade I, 14.6% had grade II, 50% had grade III, while 18.8% had grade IV and 12.5% had grade V. In Korea, the series of VUR cases of Jang et al. were classified as VUR grade I in 9.2%, grade II in 36.4%, grade III in 27.7, grade IV in 16.5, and grade V in 10.1%. Differences in VUR grades among different studies may be due to variable study selection criteria and timing of cases presentation (i.e., early or late).19 It is to be noted that grades of VUR may constitute an important prognostic variable. Greenbaum and Mesrobian reported that rate of VUR resolution varies.4 Grades I and II reflux eventually cease in more than 80% of affected ureters, with a resolution rate of 10% to 25% per year. Grade III reflux resolves in more than 50% of cases, and grade IV VUR resolves in approximately 30% of cases. Grade V reflux is unlikely to resolve spontaneously. In the present study, imaging diagnostic modalities were applied. Ultrasonography showed abnormal findings in 45.8%which was done as first tool for workup of a patient with UTI . DMSA revealed renal scarring in 50% of cases. Several recent studies discussed the role and benefits of radiography in VUR. Demède and Mouriquand stated that when the renal sonography is normal, the cystography should be reserved for those cases where an abnormal DMSA scan is found or if surgery is contemplated.8 When the renal sonography is abnormal, a cystography should be performed in all infants irrespective of the findings of the DMSA scan. Leroy et al. added that renal ultrasonographic findings are believed to be good predictors of VUR. 13 Craig et al. noted that the American Academy of Pediatrics recommends ultrasonography and either voiding cystourethrography or radionuclide cystography.20 Given the good prognosis for children with VUR and the absence of good evidence for improved outcomes, the invasive, unpleasant nature of a VCUG outweighs the possible benefit of prophylactic treatment.18 Farhat et al. noted that the widespread use of routinely performing prenatal ultrasonography has led to more frequent detection of antenatal hydronephrosis. When screened, approximately 10% to 20% of these children proved to have VUR.21 Howard et al. stated that the correlation between renal scarring and VUR has been shown to vary between 23% and 75% and is higher in patients with a high grade of VUR.22 So, the high prevalence of renal scarring among VUR patients in the present study may be explained by several reasons, i.e., delayed presentation, late diagnosis and management as well as a high VUR grade among cases. Results of this study indicated that Chronic kidney disease was present in 25% (12) of VUR cases in form of proteinuria, raising of urea and creatinine, while 8.3% (4) were hypertensive as showed in figure (1) . McLaren et al. noted that VUR may result in hypertension and end-stage renal disease.23 Rodriguez et al. explained that VUR may predispose a child with a bladder infection to the development of pyelonephritis, which may lead to renal scarring and hypertension.11 Similarly, Lim emphasized that the current standards of care in the United States recommend that infants and young children with first-time UTI undergo imaging tests to evaluate for VUR.24 The severity of VUR is thought to correlate to the risk of developing permanent renal scarring that may lead to serious sequelae later in life, such as hypertension, proteinuria or end-stage renal disease. Interventions, such as follow-up imaging, antibiotic prophylaxis and surgical correction are thought to reduce the incidence of these complications. Sharbaf et al. added that complication such as hypertension and renal failure are common complication of VUR, therefore arterial blood pressure and renal function need to be continuously monitored in these patients.2 About one third of cases in the present study were managed medically, while two thirds were managed medically and surgically by anti-reflux surgery using injection of bulking agent (deflux ), either once or more than once. It was noticed that the main reason for deflux injection failure was due to neurogenic bladder. Callewaert stated that surgical treatment of VUR as well as medical treatment by prophylactic antibiotics prevent infections and renal scarring.25 Gill et al. noted that surgical techniques for VUR apply the basic principle of creating an anti-reflux mechanism by increasing the portion of the distal ureter lying in a submucosal tunnel between the detrusor muscle and the bladder mucosa.26 Sharbaf et al. added that anti-reflux surgery offers no short-term advantages other than abolishing the reflux. It also does not result in improved renal function or renal growth, and does not affect the rate of new scar formation or the incidence of hypertension.2 Comparing the male patients with female patients revealed a higher prevalence of renal scarring among girls than boys, higher incidence of recurrent UTI among boys, higher prevalence of kidney abnormalities among girls and a significantly higher prevalence of residual reflux among girls. Variable and contradicting results were reported by different authors. Sharbaf et al. stated that VUR is more common, yet less severe, in girls than boys.2 They also reported that incidence of renal scaring is significantly higher among boys than girls. Alova and Lottmann reported that renal parenchymal lesions were higher among boys than girls.27 Greenbaum and Mesrobian noted that girls with VUR are more likely to have UTI than boys,4 while Lim reported that incidence of UTI is higher among boys than girls.25 This variability in reported results may be due to differences among studies in sampling and methodology. In conclusion, VUR affects more girls than boys in Aseer Region, starting as early as the first days of life, indicating its congenital etiology. The main presentation for these children is UTI. Most cases have high grades of VUR (i.e., grades III and higher), and prevalence of renal scarring is quite high, indicating a late presentation. Imaging is important in assessment of VUR cases. Girls experience significantly higher residual reflux than boys. It is recommended to routinely screen by ultrasound all children with UTI for VUR. The awareness of general practitioners regarding VUR should be raised and they should be advised to refer immediately any child with UTI to a pediatrician. Abbreviations VUR: Vesicoureteral reflux UTI: Urinary tract infection VCUG: Voiding cystourethrography DMSA: 99 m Technetium-dimercaptosuccinic acid
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of Funding: None
Conflict of Interest: None
References:
1. Rushton HG. Vesicouretral reflux and scaring. In: Avner ED, Harman WE, Niaudet P. Pediatric Nephrology. 5th edn, Philadelphia Lippincott Williams and Wilkins, 2004; 1027- 1048.
2. Sharbaf FG, Fallahzadeh MH, Modarresi AR, Esmaeili M. Primary Vesicoureteral Reflux in Iranian Children. Indian Pediatrics 2007; 44:128-130.
3. Herndon CDA, DeCambre M, McKenna PH. Changing concepts concerning the management of vesicoureteral reflux. J Urol 2001;166:1439–43.
4. Greenbaum LA, Mesrobian HO. Vesicoureteral Reflux. Pediatr Clin N Am 53 (2006) 413– 427.
5. Chand DH, Rhoades T, Poe SA, et al. Incidence and severity of vesicoureteral reflux in children related to age, gender, race and diagnosis. J Urol 2003; 170:1548–50.
6. Cleper R, Krause I, Eisenstein B, et al. Prevalence of vesicoureteral reflux in neonatal urinary tract infection. Clin Pediatr (Phila) 2004;43(7):619– 25.
7. Ardissino G, Dacco V, Testa S, et al. Epidemiology of chronic renal failure in children: data from the ItalKid project. Pediatrics 2003;111(4 Pt 1):e382-7.
8. Demède D, Mouriquand P.Vesicoureteral Reflux: Why we Can’t Agree on its Management! An Evidence Based Approach. Arch Esp Urol, 2008; 61 (2):160-6.
9. Estrada JR CR. Vesicoureteral Reflux. http://emedicine. medscape.com/article/439403-overview. date retrieved: 13 November 2013
10. Dähnert W. Radiology Review Manual. Lippincott Williams and Wilkins, 2011. 1
1. Rodriguez E Jr, Weiss DA, Copp HL. Adherence to Antibiotic Prophylaxis in Children with Vesicoureteral Reflux. Advances in Urology 2011; vol. 2011, Article ID 134127, 6 pages, 2011.
12. Kaefer M, Curran M, Treves ST. Sibling vesicoureteral reflux in multiple gestation births. Pediatrics 2000; 105: 800- 804.
13. Leroy S, Vantalon S, Larakeb A, Ducou-Le-Pointe H, Bensman A. Vesicoureteral Refl ux in Children with Urinary Tract Infection: Comparison of Diagnostic Accuracy of Renal US Criteria. Radiology 2010; 255(3): 890-98.
14. Wald ER. Vesicoureteral Reflux: The Role of Antibiotic Prophylaxis. Pediatrics 2006;117;919-22.
15. Smellie JM, Jodal U, Lax H, Writing Committee for the International Reflux Study in Children (European Branch), et al. Outcome at 10 years of severe vesicoureteric reflux managed medically: report of the international reflux study in children. J Pediatr 2001; 139:656–63.
16. Godley ML. Vesicoureteral reflux: Pathophysiology and experimental studies. Gearhart JP, Rink RC, Mouriquand PDE, eds. Pediatric Urology, Philadelphia: W.B. Saunders Company, pág. 359-381, 2001.
17. Garin EH, Olavarria F, Nieto VG, et al. Clinical significance of primary vesicoureteral reflux and urinary antibiotic prophylaxis after acute pyelonephritis: A multicenter, randomized, controlled study. Pediatrics, 117: 626, 2006.
18. Williams G, Fletcher JT, Alexander SI, Craig JC. Vesicoureteral reflux. J Am Soc Nephrol 2008; 19 (5): 847 – 862.
19. Jang HC, Lee KH, Park JS. Primary Vesico-Ureteral Reflux: Comparison of Factors between Infants and Children. Korean J Urol 2011;52:206-209
20. Craig JC, Irwig LM, Knight JF, Roy LP: Does treatment of vesicoureteric reflux in childhood prevent end-stage renal disease attributable to reflux nephropathy? Pediatrics 105: 1236–1241, 2000
21. Farhat W, McLorie G, Geary D, et al. The natural history of neonatal vesicoureteral reflux associated with antenatal hydronephrosis. J Urol 2000;164(3 Pt 2):1057 –60.
22. Howard RG, Roebuck DJ, Yeung PA, Chan KW, Metreweli C. Vesicoureteric reflux and renal scarring in Chinese children. Br J Radiol. 2001;74:331–334.
23. McLaren CJ, Simpson ET. Vesico-ureteric reflux in the young infant with follow-up direct radionuclide cystograms: the medical and surgical outcome at 5 years old. BJU Int. 2002;90:721–724.
24. Lim R. Vesicoureteral Reflux and Urinary Tract Infection: Evolving Practices and Current Controversies in Pediatric Imaging. AJR 2009; 192:1197–1208
25 Callewaert PRH. What is new in surgical treatment of vesicoureteric reflux? Eur J Pediatr 2007; 166:763–768.
26. Gill IS, Ponsky LE, Desai M, Kay R, Ross JH (2001) Laparoscopic cross-trigonal Cohen ureteroneocystostomy: novel technique. J Urol 166(5):1811–1814.
27. Alova I, Lottmann HB. Vesico ureteral reflux and elimination disorders. Arch Esp Urol 2008; 61(2): 218-28.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





