IJCRR - 7(1), January, 2015
Pages: 24-27
Print Article
Download XML Download PDF
EFFECT OF RIGID TAPING ON PAIN AND GAIT PARAMETERS IN KNEE OSTEOARTHRITIS
Author: Anood Faqih, Ulka Gavankar, Neha Tambekar, Savita Rairikar, Ashok Shyam, Parag Sancheti
Category: Healthcare
Abstract:Background: The incidence of osteoarthritis has been seen to increase drastically over the years. The symptoms of osteoarthritis include pain, swelling, loss of function, changes in gait and an overall reduction in the quality of life. A lot of studies have been performed for the treatment of symptomatic relief of these patients including cryotherapy, kinesiotaping, therapeutic modalities. However, limited studies have been conducted on the immediate symptomatic relief with rigid taping and the effect on gait parameters. Hence, the purpose of this study is to know the effect of rigid taping on pain and gait parameters in knee osteoarthritis. Methods: 120 subjects having bilateral osteoarthritis of the knee were screened according to the inclusion and exclusion criteria and were included in the study. Pain was assessed using the Visual Analog Scale and gait parameters such as stride length, step length and cadence were assessed using the footprint method pre and post application of a rigid tape. Results: To measure the changes in pain intensity and gait parameters such as step length, stride length and cadence pre and post taping paired T test was used. The level of significance was set at p value ? 0.05. Changes in pain intensity, step length, stride length and cadence, p=0.00 which shows that there is significant change in the above characteristics after the application of a rigid tape.
Conclusion: From this study, it was hence concluded that after rigid taping there was a significant decrease in the pain intensity and the gait parameters such as step length, stride length and cadence improved in patients with knee osteoarthritis.
Keywords: Step length, Stride length, Cadence, Tape
Full Text:
INTRODUCTION
Osteoarthritis (OA) is a degenerative condition of the joint which involves mainly the articular cartilage and the subchondral bone. This is a condition in which natural cushioning between joints and cartilage wears away causing friction between articulating surfaces. This leads to pain, swelling around joint, stiffness, crepitus, abnormal gait pattern, deformities, and spur formation.[1]OA is a common condition seen after 40 years of age and is widespread in adults older than 65.[2]The incidence of osteoarthritis has been increasing drastically over the years. Knee is an important weight bearing joint in the body. Walking is the most common method of human locomotion and causes repetitive joint loading. Hence, gait is commonly affected in patients having osteoarthritis.[3] Due to pain the patient tends to walk with an antalgic gait and this inturn affects the gait parameters. The presence of pain and radiographic joint degeneration defines OA clinically.[4] OA is commonly graded on radiographs using the Kellgren and Lawrence scale[2]. Taping has been used as a part of rehabilitative and prophylactic programmes in managing musculoskeletal disorders.[5] Taping has been used as a method in physical therapy to reduce pain.[6][7][8] There are different types of taping techniques available. A rigid tape is an inelastic adhesive tape. Prior to the application of a rigid tape, a protective under wrap is commonly used.[5] Taping helps provide support to the injured soft tissues including ligaments, tendons and muscles. It helps limit unwanted joint movement. It allows optimal healing without causing unwanted stress on the tissues which are injured. It helps to support and protect the structures in a functional position during strengthening, exercise etc. Taping also enhances proprioceptive feedback from the part to which it is applied.[9] The purpose of this study was to know the effect of rigid taping on pain and gait parameters such as step length, stride length and cadence in patients having osteoarthritis of the knee.
METHODS AND METHODOLOGY
Informed consent was taken from the subjects. The study was performed on 120 subjects in outpatient physiotherapy departments. The study design was a quasi experimental type of study and the method of sampling was purposive. Inclusion Criteria was patients in the age group of 40-70 years with bilateral patello-femoral and medial compartmental osteoarthritis of the knee. Those having lateral patella tracking and grade 1-2 on Kellgren and Lawrence grading for osteoarthritis on radiographs Exclusion Criteria was patients giving a history of hypersensitive skin or any other skin conditions. Patients having sensory and motor deficits. Any fracture of the lower limb, any other inflammatory condition of other joints and any other concurrent pain.
Procedure
Study and study design were approved by the institutional review board. Patients were screened according to the inclusion criteria and were included in the study. They were evaluated using the Visual Analog Scale for pain and gait analysis was done in a 2D gait lab using the foot print method pre taping. Rigid tape was applied for the knee. An underwrap was applied before the application of the rigid tape. An underwrap is a thin polyurethane foam material used for the protection of sensitive skin. Patient was in a sitting position with knee in full extension. One anchor strap was placed over the superior pole of patella. One strip of tape was attached to the anchor on the medial side of the knee and was pulled obliquely downwards to the lateral side with the top edge of the tape passing just under the inferior pole of the patella. The same action was repeated lateral to medial to make a cross-over effect. Gait parameters such as step length, stride length and cadence were measured. Re-evaluation for pain and gait parameters was done immediately after application of rigid taping. Step length was measured as the linear distance between the two successive points of contact of opposite extremities i.e. from heel strike of one extremity to the heel strike of the opposite extremity. Stride length was measured as the linear distance from the point of one heel strike of one lower extremity to the point of the next heel strike of the same extremity. Cadence was measured by the number of steps the patient took in a duration of 10 seconds.[10]
RESULTS
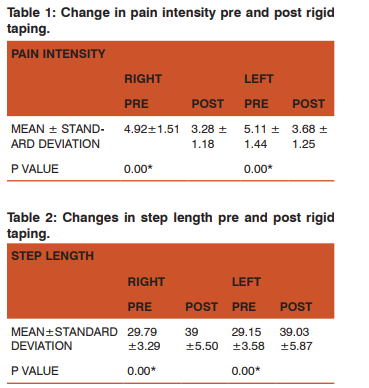
To measure the changes in pain intensity and gait parameters such as step length, stride length and cadence pre and post taping paired T test was used. The level of significance was set at p value ≤ 0.05. Changes in pain intensity, step length, stride length and cadence p=0.00 which shows that there is significant change in the above characteristics.
DISCUSSION
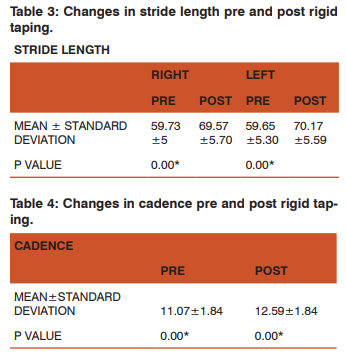
This study has shown that after the application of a rigid tape to the knee joint, there was a significant reduction in the pain intensity and gait parameters such as step length, stride length and cadence improved significantly. The taping technique used in this study, helped to unload the quadriceps tendon thereby reducing the stresses over the quadriceps tendon attachment. [11] This could explain the reduction in pain intensity of the subjects. Table 1 shows that post rigid taping there was a significant reduction in the pain intensity in both the knees. When a medially directed force is applied to the patella, it increases the patella-femoral contact, thereby, reducing stresses and improving pain. [6] Also, therapeutic taping helped improve pain and disability significantly in patients with knee osteoarthritis. [8] According to this study, there was a significant improvement in the gait parameters such as step length, stride length and cadence (Table 2, 3, 4). Patella taping helped correct the mal-alignment of the patella improving the efficiency of the quadriceps muscle which is an important muscle involved during gait. Correcting the mal-alignment of the patella and in turn the quadriceps attachment improves the biomechanical efficiency or pull of the quadriceps muscle. Also, unloading the tendon helped reduce stresses over the quadriceps attachment reducing pain. All these factors helped to improve the overall function of the quadriceps musculature. Position of the patella has a strong influence on the function of the quadriceps muscle. The patella acting like an anatomical pulley lengthens the mechanical advantage of the quadriceps by increasing the distance of the quadriceps tendon from the knee joint axis. The line of action of the quadriceps femoris is deflected away from the center of the joint by the patella which increases the angle of pull and the muscles ability to produce an extension torque. Patella-femoral joint reaction and compressive forces are high during daily activities such as walking. [12] Taping the patella to control spin, tilt, lateral glide to optimize pain is useful for efficacy and causes possible early vastus medialis obliquis (VMO) onset and improves functional capacity of the knee. [13] Taping has shown to influence the patella-femoral joint functioning. [14] A study done on the effectiveness of ankle taping on the kinematics of ankle joint during level ground walking showed that there was a significant change in step length, step duration, double stance and swing phase post ankle taping.[15] Pain limits functional activities and may lead to an overall reduction in the quality of life of the patient. Walking is an important activity of daily living which is affected in patients with osteoarthritis. Muscle pain modulates the function of the quadriceps muscle during the loading phase of walking and may lead to impaired knee joint function. [16] Hence, rigid taping is an easy, cost effective and an efficient way of treatment of pain relief. It can, therefore, be a handy tool in clinical practice for the immediate symptomatic relief of OA by reducing the pain and improving the gait parameters such as stride length, step length and cadence. Study Limitations: Effect of rigid taping could be measured on other parameters of gait.
CONCLUSION
From this study, it was concluded that rigid taping showed a significant improvement in pain of patients with osteoarthritis and hence there was improvement seen in all the gait parameters such as step length, stride length and cadence.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles were cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. We would also like to thank all our participants and for their valuable time and participation.
Financial Support: None
Conflict of Interest: None
References:
1. Maheshwari J. Essential Orthopaedics. 3rd Edition(Revised). New Delhi: Mehta Publishers; 2005.p 252-253.
2. O’Sullivan S, Schmitz Thomas. Physical Rehabilitation. 5th Edition. New Delhi: Jaypee Brothers Medical Publishers (P) Ltd; 2006, p1067.
3. Henriksen M, Graven-Nielsen T, Aaboe J, Andriacchi TP, Bliddal H. Gait changes in patients with knee osteoarthritis are replicated by experimental knee pain. Arthritis Care and Research. 2010; 62(4): 501-509.
4. Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, et al. Development of criteria for the classification and reporting of osteoarthritis: classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheumatism.1986; 29(8):1039–49.
5. Alexander CM, McMullan M, Harrison PJ. What is the effect of taping along or across a muscle on motoneurone excitability? A study using Triceps Surae. Manual Therapy. 2008; 13(1): 57-62.
6. Handbook of Non Drug Intervention (HANDI) Project Team. Taping for knee osteoarthritis. Australian Family Physician. 2013 Oct;42(10):725-6.
7. Hinman RS, Crossley KM, McConnell J, Bennell KL. Efficacy of knee tape in the management of osteoarthritis of the knee: blinded randomised controlled trial.BMJ. 2000; 327(7407):135.
8. Hinman RS, Bennell KL, Crossley KM, McConnell J. Immediate effects of adhesive tape on pain and disability in individuals with knee osteoarthritis. Rheumatology (Oxford). 2003;42(7) 865-9.
9. Macdonald R. Taping techniques- Principles and practice. 2nd Edition.Butterworth-Heinemann;2004. p3-4.
10. Levangie a, Norkin C. Joint structure and function- A comprehensive analysis. 4thEdition. New Delhi: Jaypee Brothers Medical Publishers (P) Ltd; 2006. p523.
11. Macdonald R. Taping techniques- Principles and practice. 2nd Edition.Butterworth-Heinemann; 2004. p118-119.
12. Levangie P, Norkin C. Joint structure and function- A comprehensive analysis. 4th Edition. New Delhi: Jaypee Brothers Medical Publishers (P) Ltd; 2006. p416,424.
13. Barton C, Balachandar V, Lack S, Morrissey D. Patellar taping for patella-femoral pain: a systematic review and metaanalysis to evaluate clinical outcomes and biomechanical mechanisms. British Journal of Sports Medicine. 2014; 48(6):417-24.
14. Herrington L, Malloy S, Richards J. The effect of patella taping on vastus medialis oblique and vastus laterialis EMG activity and knee kinematic variables during stair descent. Journal of Electromyography and Kinesiology. 2005; 15(6):604-7.
15. Choukou MA, Hijazi S. Effectiveness of ankle taping on ankle joint kinematics during walking on level ground. Foot & Ankle Speclist. 2013;6(5):352-5.
16. Henriksen M, Alkjaer T, Lund H, Simonsen EB, Graven-Nielsen T, Danneskiold-Samsøe B, Bliddal H. Experimental quadriceps muscle pain impairs knee joint control during walking. Journal of Applied Physiology.2007;103(1):132-139.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





