IJCRR - 7(2), January, 2015
Pages: 66-68
Print Article
Download XML Download PDF
BILATERAL OCCURENCE OF THIRD HEAD OF BICEPS BRACHII ASSOCIATED WITH UNILATERAL VARIATION IN THE COURSE OF MUSCULOCUTANEOUS NERVE - A CASE REPORT
Author: Shastrakar Rupali Sureshrao, Sawant V. G.
Category: Healthcare
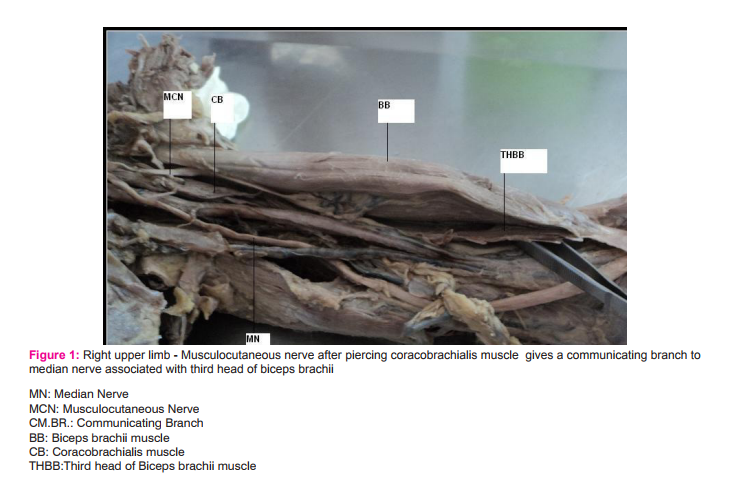
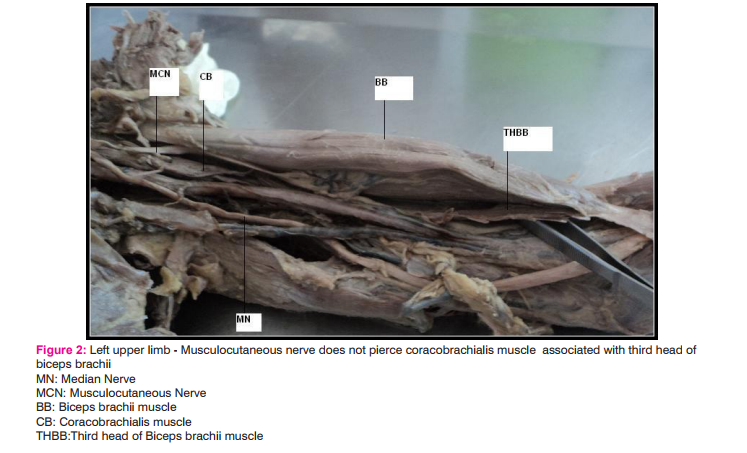
Abstract:It is very common to see variations in the course of nerves and muscles of the arm. We observed one bilateral concurrent variation in the course of musculocutaneous nerve and origin of biceps brachii muscle. Musculocutaneous nerve, after piercing the coracobrachialis muscle gives one communicating branch to the median nerve and then supply the third head of biceps brachii and brachialis muscle in the right upper limb. After that it continues as the lateral cutaneous nerve of forearm.In the left upper limb musculocutaneous nerve is not piercing the coracobrachialis muscle but otherwise following the normal course.
Keywords: Nerve, Musculocutaneous, Median, Biceps brachii, Third head of biceps brachii
Full Text:
INTRODUCTION
Brachial plexus is formed by the anterior primary rami of spinal nerves C5, C6, C7, C8 and T1. The plexus is said to be prefixed when the branches of fourth cervical fibers join the plexus and postfixed when joined by branches from second thoracic nerves. C5 and C6 roots join to form upper trunk. C7 root forms the middle trunk. C8 and T1 roots join to form lower trunk. Each trunk divides into ventral and dorsal divisions. Ventral division of the lower trunk forms medial cord. Dorsal divisions of all the three trunks join to forms posterior cord. Ventral divisions of upper and middle trunk joint to forms lateral cord. Musculocutaneous nerve (MCN) is the branch from the lateral cord of the brachial plexus. The nerve initially accompanies the axillary artery, pierces the coracobrachialis muscle, and then passes downwards between the biceps brachii and brachialis. It supplies coracobrachialis, biceps brachii and medial part of brachialis muscles. Below the elbow joint the nerve is continuous as the lateral cutaneous nerve of the forearm. It should be noted that the brachial plexus is the most variable part of the peripheral nervous system [1]. The prevalence of variations ranges from 12.8 up to 53% [1, 2].Variations of the musculocutaneous nerve may occur in 6.25% of cases [3]
CASE REPORT
During routine dissection for medical undergraduates ,in a middle aged Indian cadaver we observed a variation in the course of musculocutaneous nerve associated with third head of biceps brachii muscle . In the right upper limb , musculocutaneous nerve after piercing the coracobrachialis muscle gives one communicating branch to the median nerve to supply the third head of biceps brachii and brachialis muscle . In the left upper limb ,third head of biceps brachii associated with normal course of musculocutaneous nerve except that it is not piercing the corachobrachialis . After that it continues as lateral cutaneous nerve of forearm in the right and the left upper limb.
DISCUSSION
Variations in the course and termination of musculocutaneous nerve are common . As reported by Venieratos D. and Anagnostopoulou S. [4],there are three types of communications between musculocutaneous and median nerve with reference to coracobrachialis muscle. In one type ,communication was proximal to entry of musculocutaneous nerve into coracobrachialis. In second type communication was distal to entry of musculocutaneous nerve into coracobrachialis. In third type nerve and communicating branch did not pierce the coracobrachialis muscle. According to Loukas M. and Aqueelah H. four different patterns of communication exist between musculocutaneous and median nerve.Type I (54 communications , 45%).The communications were proximal to the point of entry of musculocutaneous nerve into coracobrachialis. Type II (42, communications, 35%) the communications were distal to the point of entry of the MCN into the coracobrachialis; type III (11 communications, 9%): the MCN did not pierce the coracobrachialis; and Type IV (9 communications, 8%) : the communications were proximal to the point of entry of the MCN into the coracobrachialis and additional communication took place distally. [5] In this case report the findings coinside with second type of communication mentioned by Venieratos D. and Anagnostopoulou S. and Type II by Loukas M .and Aqueelah H., in the right upper limb. The lateral root of the MN carries fibres that may pass through the MCN, and a communicating branch from the later usually joins the MN in the lower third of arm[13].In the left upper limb it coinside with Type III by Loukas M .and Aqueelah H. A supernumerary head of biceps brachii is the most frequently occurring muscular variation in the upper limb, prevalence is upto 22.9%.[6] Variations include bifurcate origin of long head[7], occurrence of third head [8-9] and occurrence of four heads[10-11].Greig, Anson and Budinger found one or more accessory heads of biceps brachii in 28 (21.5 %) of 130 muscle studied. In most of them extra head was arising from middle third of humerus. In another two it arose from intertubercular groove and in other five from the pectoralis major. In this case the third head is arising from the middle of the shaft of humerus. The clinical relevance of such variations might also be correlated to entrapment syndromes. Entrapment of MCN is rare and has its origin either in physical activity according to Falsenthal et al., 1984[14] or in violent passive movements of arm and forearm according to Kim and Goodrich, 1984[15 ]. This knowledge may prove useful for clinicians in order to avoid an unnecessary Carpal tunnel release [4]. Knowledge of these variations is important in traumatology and in plastic and reconstructive surgeries.
References:
1. Johnson E, Vekris M, Demesticha T, Soucacos P (2010) Neuroanatomy of the brachial plexus: normal and variant anatomy of its formation. Surg Radiol Anat 32:291–29
2. Pandey SK, Shukla VK (2007) Anatomical variations of the cords of brachial plexus and the median nerve. Clin Anat 20(2):150–156
3. Bhattarai C, Poudel PP (2009) Unusual variation in musculocutaneous nerves. Kathmandu Univ Med J 7:408–410
4. Venieratos D, Anagnostopoulou S. Classification of communications between the musculocutaneous and median nerves. Clin Anat 1998; 11: 327–331.
5. Loukas M, Aqueelah H. Musculocutaneous and median nerve connections within, proximal and distal to the coracobrachialis muscle. Folia Morphol (Warsz). 2005; 64: 101–108.
6. Vijayabhaskar P, Baral P, Vaishya R, Shrestha RN (2008) Supernumerary head of biceps brachii: a rare occurrence in the Nepalese population. Kathmandu Univ Med J 6:225– 227.
7. Enad JG. Bifurcate origin of the long head of the biceps tendon. Arthroscopy. 2004; 20: 1081–1083. 8. Abu-Hijleh MF. Three-headed biceps brachii muscle associated with duplicated musculocutaneous nerve. Clin. Anat. 2005; 18: 376–379.
9. G. Sreedevi, S.S. Sarada Devi, K. Krupadanam, K. Anasuya. Bilateral occurrence of additional heads of biceps brachii-A case report. Int J Res Dev Health.Nov 2013;Vol1(4):195-9.
10. Vazquez T, Rodriguez-Niedenfuhr M, Parkin I, Sanudo JR. A rare case of a four-headed biceps brachii muscle with a double piercing by the musculocutaneous nerve. Surg. Radiol. Anat. 2003; 25: 462–464.
11. Poudel PP, Bhattaraj C. Study of the supernumerary heads of biceps brachii muscle in Nepalese. Nepal Med Coll J. 2009 Jun; 11 (2):96-8.
12. Greig HW, Anson BJ ,Budinger JM:Quart Bull Northwestern Univ M. School , 26:241,1952 (Quoted by ,W.Henry Hollinshead,’The Back And Limbs ‘, Third edition , Vol 3:354, 1982).
13. Bergmann RA, ThomsonSA and Saadeh F.A Compendium of human anatomic variation urban &schwarzebergMunich.1988; 139-143.
14. Falsenthal, G., Mondell, DL., Reischer, MA., Mack, RH. Forearm pain secondary to compression syndrome of the lateral cutaneous nerve of the forearm. Archaeological Physical Medical Rehabilitation, 1984, vol. 65, p. 139-141. PMid:6608339.
15. Kim, SM., Goodrich, JA. Isolated proximal musculocutaneous nerve palsy: Case report. Archaeological Physical Medical Rehabilitation, 1984, vol. 65, p. 735-736.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





