IJCRR - 7(2), January, 2015
Pages: 41-46
Print Article
Download XML Download PDF
A RANDOMIZED OPEN LABELED COMPARATIVE CLINICAL STUDY ON THE EFFICACIES OF HIJAMATBILA SHURT AND HABBE GULE AAKH IN CERVICAL SPONDYLOSIS
Author: Mirza Ghufran Baig, Mohd Aleemuddin Quamri
Category: Healthcare
Abstract:Introduction and Objectives: Cervical Spondylosis is a degenerative disease of intervertebral discs and adjacent vertebral bodies of the cervical region with or without neurological sign. Despite the advancement in pharmacological, non pharmacological and surgical interventions, the management remains unsatisfactory due to high cost, and unusual eventualities. Unani physicians managed such joint disorders with diverse treatment modalities viz., diet, drugs, regimens such as dalk (massage) , riyazat (excercise), hijama (cupping), etc. Hence to scientifically validate the efficacies of Hijamat Bila Shurt (regimen) and Habbe Gule Aakh (a poly herbal formulation) a comparative clinical trial was conducted. Material and Methods: The study was conducted as a comparative, open labeled, randomized clinical trial on 30 patients with 15 in each group. Both groups received treatment for 21 days, Hijamat Bila Shurt group subjected once daily and Habbe Gule Aakh 2 BD orally with three follow ups (7th, 14th and 21st). The pre and post treatment effects were assessed based on subjective and objective parameters. Results and Conclusion: The subjective parameters like neck pain, tenderness, and difficulty in neck movement were reduced with high statistical significance (p< 0.001) with no significant reduction in paraesthesia in both group (p>0.05). Objective parameters Northwich Park Neck Pain Questionnaire (NPQ) revealed strong statistical significance (p< 0.001) in both groups, whilstno significant change observed neither in Spurling Test (ST) nor in Neck Distraction Test (NDT) (p>0.05). Inter group analysis reveals no statistical significance (p>0.05) difference between the groups, but Hijamat Bila Shurt is found comparatively more
effective than Habbe Gule Aakh using ANOVA and student 't' test (two tailed and independent). Moreover, both groups were found safe without any adverse effect.
Keywords: Cervical spondylosis; Hijamat Bila Shurt; Habbe Gule Aakh; Unani medicine
Full Text:
INTRODUCTION
Cervical Spondylosis (s?rv ??-k?l + (spondyl osis) the terms are derived from Latin cervic means “neck”, and spondyl, osis means “vertebra condition” which stands for the degenerative arthritis, osteoarthritis of the cervical vertebrae and related tissues. 1 it is a collective term describing degenerative changes that occur in the apophysial joints and intervertebral disc joints (cervical vertebrae), with or without neurological sign.2 The etiology was thought to be related to aging process and or mechanical over load applied to the spine.3 As age advances degeneration sets into the spine, however, there are some exceptions where spinal injuries to the disc can augment the degenerative process in the younger patient. Compression of the vascular and neural structures can leads to the manifestation of spondylosis secondarily and it is caused by a loss in the disc height and impinging osteophytes (mechanical cause) that contribute to cervical radiculopathy and later myelopathy.4 In general population the prevalence of Cervical spondylosis with incidence rate of 83 per one lakh populations and with the prevalence of 3.3 cases per one thousand people, and it occurs mostly between the 4th and 5th decades of life.3 As per the estimates over half of the adults experience some degree of neck pain every year, and 60–80% of older adults experience neck pain due to degenerative changes.5 Cervical spondylosis is a common and disabling condition and it is felt that it should be managed through multiple approaches viz., physical or non pharmacological, pharmacological, and or surgical. Surgery should be reserved for cases of myelopathy. 5,6,7,8 All these treatment modalities have a range of effects and their availability is meagre and cost over burdened, apart from this the unexpected or unusual eventualities ranges from mild to moderate and sometimes even severely observed. Unani physicians managed joint disorders with diverse treatment modalities viz., diet, drugs, and regimens. Cervical Spondylosis is described as Waja ul Unuq a type of Waja ul Mafasil, and treated as per the line of treatment of Amraze Mafasil with regimens including diet, drugs, and surgery. More specifically certain regimens like Takmeed (Fomentation), Zimad (paste), Tila (liniment), Roghaniyat (Oils), Dalk (massage), Hijamat Bila Shurt (dry cupping), Mahjima Nariya (fire cupping), Fasd (venesection) etc are advised as treatment modes for Cervical Spondylosis, besides this pharmacologically it will be treated with single and compound drugs such as Suranjaan (Colchicum luteum) , Muqil (Cammiphora mukul), Gule Aakh (Calotropis gegentia), Zanjabeel (Zingiber officinalis), Habbe Suranjaan, Habbe Gule Aakh, Roghane Baboon, Roghane Hifte Barg, Roghane Suranjaan, Roghane Chanbeli, Roghane Sosan, and Rogane Shibit, etc.9,10, It was hypothesized that a regimen Hijamat Bila Shurt (Dry Cupping) and a pharmacopoeial poly herbal formulation Habbe Gule Aakh (Drug) will be evaluated comparatively for their efficacies, and further to validate scientifically the interventions this study was conducted. The Habbe Gule Aakh a poly herbal pharmacopoeial formulation comprises of Zanjabeel (Zingiber officinalis), Gule Aakh (Calotropis gigentia), Filfil Siyah (Pepper nigrum), and Barge Bans (Bambosa aurundinacea), and it is indicated as anti inflammatory and analgesic 11,12 Hijamat Bila Shurt (Dry Cupping) in which a suction cup will be placed over the muscular surface and suctioned so as to create a negative pressure beneath the cupped area. The objective of this regimen is for Imalae mawad (diversion of vitiated matter), 13,14,150,16 Tanqiae mawad (evacuation of matter), 13 Taskeen alam (to alleviate pain)13,15 Tehleele auram (to resolve inflammation) 13 Tehleele riyah 13,14,15 and Taskheene muqam (local calorific). 13, 14, 15
MATERIAL AND METHODS
The study was conducted between March 2013 to March 2014 as an open labeled, randomized, comparative clinical trial on 30 patients after obtaining ethical clearance vides IEC No: NIUM/IEC/2011-12/003/Moal / 03 from the institutional ethical committee for biomedical research of NIUM Hospital, Bangalore. Based on the criterion of inclusion patients of both gender, between 20-60 years of age, having cervical headache with or without radicular symptoms ( paraesthesia,) Spurling Test (ST) and Neck Distraction Test (NDT) positives, and patients having other type of arthritis of neck (except osteoarthritis), trauma of neck, wry neck, Vertebro basilar insufficiency, local wound and infection over neck, cervical rib syndrome, Psycho somatic disorder, spinal cord disorders, carpal tunnel syndrome, pregnancy and lactation, all chronic diseases, patient who do not report for follow up, unwillingness or inability to comply the requirements of the protocol were excluded. A total of 170 patients were screened clinically and subjected to laboratory investigations, out of which 55 cases fulfilled the inclusion criterion, but 33 cases participated in the study by exercising the written informed consent, then they were randomly allocated into two groups by using G pad soft. Group A: Hijamat Bila Shurt (n=17) and Group B: Habbe Gule Aakh (n=16 ) were received interventions for 21 days with three follow ups on 7th, 14th and 21st day. At last 30 cases completed the study protocol (15 in each group) and they were alone taken in account for analysis; 3 cases lost to follow up (Group A; 2, Group B; 1)
Interventions:
Group A: Hijamat Bila Shurt (dry cupping) patients were subjected to the procedure, in which 4 manual suction cups were applied bilaterally over the cervical region for 20 minutes. Group B: Habbe Gule Aakh (poly herbal formulation) 125 mg (prepared at NIUM pharmacy) given two pills (250 mg) orally twice i.e., 500 mg a day with water after meal.

The study effects are observed in three different follow ups and recorded in pre approved case report form in the form of subjective parameters (Neck pain (axial / radiating/ referred), tenderness, difficulty in neck movement and paraesthesia in upper extremities) and Objective parameters (VAS, Spurling Test (ST), Neck Distraction Test (NDT) and Northwich Park Neck Pain Questionnaire (NPQ). The pre and post treatment values of subjective, objective along with Safety parameters (Haemograme, Erythrocyte Sedimentation Rate, Alanine aminotransferase, Aspartate aminotransferase, Alkaline phosphatase, Blood Urea and Serum Creatinine) were analyzed statistically to draw the inference of the study.
OBSERVATION AND RESULTS
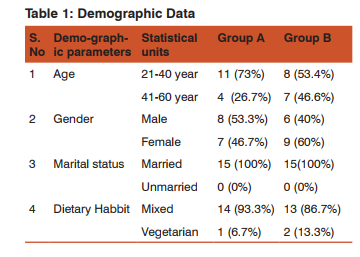
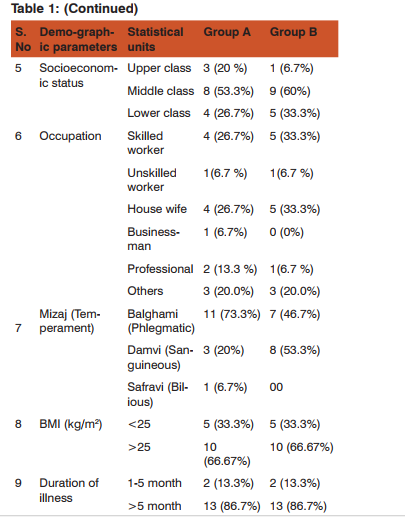
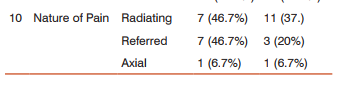
In this study 30 patients participated out of which 19 (63.2%) were found in the age group of 21- 40 and 11 (36.8 %) were between 41-60 years, 14 (46.7%) were males and 16 (53.3%) females, all were married 30 (100%), socio-economically 4 (13.3%) patients were from upper class followed by 17 (56.6%) middle and 9 (30 %) from lower class, 27 (90%) were having mixed dietary habit and 3(10%) pure vegetarian. The Mizaj (temperament) findings evidences 18 (60%) were Balghami (Phlegmatic) 11 (36.7%) Damavi (Sanguineous), and 1(3.3%) Safravi (Bilious). Occupationally 9 (30%) patients were house wives, 9(30%) skilled worker, 3(10%) professional, 2(6.7%) unskilled worker, 1(3.3%) businessmen 6(20%) others. The body mass index of 20 (66.67%) cases was found >25 and 10 (33.3%) were <25. The duration of illness (chronicity of the disease) wise was observed as 26 (86.7%) patients had more than 5 month of illness and 4 (13.3%) with 1-5 months. According to the nature of pain 18(15%) patients presented with radiating pain followed by 10(33.3%) with referred, whilst 2(6.7%) axial nature of pain (Table 1).
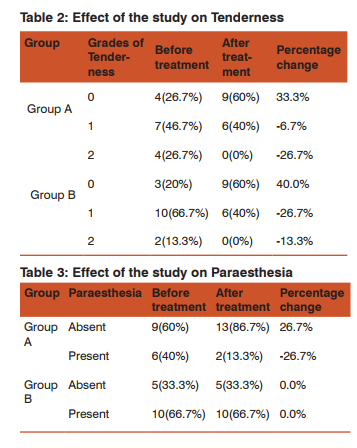
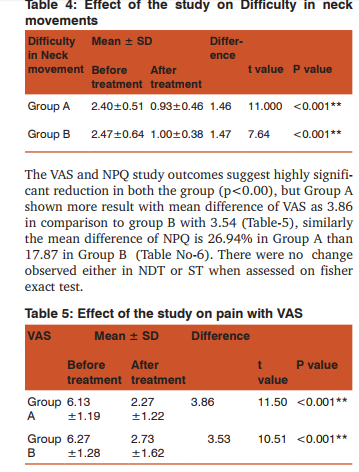
The study outcomes on subjective parameters were assessed between before treatment and after treatment by using fisher exact test, where the parameters like tenderness, paraesthesia, and difficulty in neck movement were assessed. Tenderness was improved in 33.3% in group A, and 40% in group B (Table 2). Similarly the effect on paraesthesia was observed as 26.7% in group A, no effect in group B (Table 3), but both the groups were found insignificant in terms of study response. The effect of the study on difficulty in neck movement was observed as on base line was 2.40 and after treatment it changed to 0.93 and the P value is <0.001. The mean score of difficulty in neck movements for group B was 2.47 before treatment which change to 1.00 after treatment and the p value was <0.001 (Table 4).

DISCUSSION
The data of present study revealed that disease is more prevalent in middle aged person which support the findings of Krishna Das KV17 Prasad B18 . On gender distribution it was found that the prevalence of the disease is higher in females, which correlates with the finding of Wheelees CR et al, 19 Hoy DG et al, 20 Groeneweg et al21,Cote et al,23 Graham et al6 as females have higher prevalence of degenerative changes and neck pain. In this study, the Mizaj (temperament) of subjects were reported as 18 were Balghami 11 Damavi, and only 1 was Safravi out of 30.This temperamental preponderance of Balgham in CS supports the descriptions made by the Unani physicians Zakriya Razi, Ibn Sina, Ismail Jurjani, Ibne Hubal, Akbar Arzani, and Hakim Aazm khan as Balgham is the usual cause of waja ul mafasil. 23, 24, 25,26, 27, 28 BMI findings of the study participants suggests that 20 (66.67%) cases were belongs to >25 and 10 (33.3%) were 0.05. This indicates that neither oral drug nor regimen has any significant effect on paraesthesia. The neck pain was assessed with VAS in both groups, and the intra group pre and post treatment outcomes with mean differenced are found alike 3.867 and 3.533 in Group A, and B respectively with the p value < 0.001 indicates highly significant, whereas, the inter group comparison of the effects among the two groups in terms of percentage, it was observed as 63.08 %, and 56.34% respectively, it evidences that group A is more effective in comparison to group B. The cervical spondylosis related disability was assessed with NPQ in both groups, and the intra group pre and post treatment outcomes with mean differenced are found alike 26.93 and 17.86 in Group A, and B respectively with the p value < 0.001 indicates highly significant, whereas, fisher exact test also applied for the same in order to increase reliability of come which shows 55.11% and 39.88% change in group A and B respectively. Even though, both groups shows significant improvement but more promising effect in group A. The pre and post assessments of objective parameters like Spurling Test (ST) and neck distraction test (NDT) were found insignificant in both the groups. The insignificant effects of these parameters are less considerable; because they are the signs of the disease usually may not be modified. It can be discussed that the effect of Hijamat Bila Shurt was observed from base line finding to three follow ups of 7days each. The effects of the method were observed progressive from base line to subsequent follow ups. This finding supports the observation made by Anjum et al (2005), Nayab et al (2011), Siddiqui MA et al (2011), Sheeraz et al (2013), studies on the effects of Hijamat Bila Shurt in alleviating pain, difficulty in movements and tenderness associated with various musculoskeletal condition like Knee pain , low back ache, sciatica. 30,31,32 33, 34 The effect of Habbe Gule Aakh was observed from base line finding to three follow ups of 7days each, and observed relief in symptoms progressively from base line to subsequent follow ups. This finding supports the observations of Nafees M et al (2012) as an anti-inflammatory and analgesic activity in animal module, and Usmani C (2007) clinical study with Habbe Gule Aakh in aliveating pain, difficulty in movements and tenderness associated with waja ul mafasil.5, 35, 36, hence it can be stated that the prolonged duration of treatment may more effective in term of both Hijamat Bila Shart and Habbe Gule Aakh. The study results supports the aetiopathology and principle of treatment described in Unani system of medicine. The findings also supporting that it has potential to treat the disease and may revert the pathology. This study has shown no clinically significant adverse effects, and overall compliance to the treatment of both groups was commendable because the effects on the conditions of cervical spondylosis were found ameliorated. Moreover, the results and observation evidences that the Hijamat Bila Shurt is comparatively more effective than Habbe Gule Aakh.
CONCLUSION
Due to the available resources and constrains this study was conducted with limited parameters and needed more comprehensive parameters based on long term and larger sample size for further exploration of the effects of study method adopted and also to determine their mechanism of action. It is concluded that the comparative trial revealed that both Hijamat Bila Shurt and Habbe Gule Aakh are effective and safe, and may be used for the treatment of Cervical Spondylosis.
ACKNOWLEDGEMENT
The authors are highly grateful to the Director for providing facilities and extensive co-operation throughout the study and also acknowledges to all staff of National Institute of Unani Medicine, Bangalore, India and the trial participants for their consistent support and cooperation. Authors also acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript and authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed particularly assistance rendered by staff of Central library of National Institute of Unani Medicine, Bangalore in providing the necessary classical literature.
References:
1. Venes D, editor. Taber’s Encyclopedic Medical Dictionary. 21st ed. USA, America: F.A. Davis Company Philadelphia; 2009:413,1407,2183.
2. Coblyn JS, Bermas B, Weinblatt M, Helfgott S. Brigham and Women`s Experts Approach to Rheumatology. New York: Library of Congress Cataloging in Publication Data; 2011:66-69.
3. Reddy RS, Maiya GA, Rao SK. Proprioceptive Reposition Errors in Subjects with Cervical Spondylosis. International Journal of Health Sciences & Research. 2012; 1(2): p. 65- 73.
4. Lisa AF. The Biomechanics of Cervical Spondylosis. Advances in Orthopedics. 2012:p. 1-5.
5. Marie AR. Massage Therapy for Cervical Degenerative Disc Disease:Alleviating Pain in the Neck. International Journal of Therapeutic Massage and Bodywork. 2012 September; 5(3): p. 41-46.
6. Graham N, Gross AR, Carlesso LC, Santaguida PL, MacDermid JC, Walton D, et al. An ICON Overview on Physical Modalities for Neck Pain and Associated Disorders. The Open Orthopaedics Journal. 2013; 7: p. 440-460.
7. Hirpara KM, Butler RJS, Dolan RT, O’Byrne JM, Poynton AR. Non Operative Modalities to Treat Symptomatic Cervical Spondylosis. Advances in Orthopedics. 2012; p. 1-5.
8. Rana SS. Diagnosis and Management of Cervical Spondylosis. Medscape Drug Disease and Procedures. 2013 Jun; p. 1-8.
9. Zohar AMAMI. Kitabut Taisir Fil Madawa wat Tadbir. CCRUM, New Delhi: Ministry of Health and Family Welfare,Govt of India; 1986:78-85.
10. Baig MG, Quamri MA, Ali SJ, Imtiyaz S, Sheeraz M, Ahmad Z. Concept and Management of Waja ul Mafasil (Arthritis) in Greeco Arabic Medicine- An Overview. International Journal of Current Research and Review. 6 (20):p 41-47.
11. Kabeeruddin M. Bayaze Kabeer part-2nd. Idarae Kitabus shifa. New Delhi :2010: 30, 37, 50, 57, 80,88, 89-93, 94, 176, 177, 179.
12. Anonymous. National Formulary of Unani Medicine. Part- 3rd. 1st ed. New Delhi: Govt. of India , Ministry of Health and Family Welfare; 2001:15.
13. Masihi AAFIAQ. Kitabul Umda Fil Jrahat. Vol-1st. New Delhi: CCRUM, Ministry of Health & Family welfare, Govt of India; 1986:36-38.
14. Grunner OC. The Canon of Medicine of Avicenna Incorporating a Translation of the First Book. London: Luzac & Co;1930: p.353, 508-512.
15. Sina I. Kulliyate Qanoon (Urdu translation by Mohammad Kabeeruddin). New Delhi: Ejaz publishing House; 2006:150-154,344-350.
16. Zarnigar, Arshi R. Clinical Efficacy of Al Hijama (Cupping) in Waja ul Mafasil Muzmin (Osteo arthriris). Indian Journal of Traditional Knowledge.2011; 10 (2): p 327-329.
17. Das KVK. Textbook of Medicine. 5th ed. New Delhi: Jaypee Brothers Medical Publishers (P) LTD; 2008: 1318-1319.
18. Prasad B. Principle and Practice of Medicine. 1st ed. New Delhi: Jaypee Brother Medical Publishers (P) LTD; 1997: 708.
19. Wheeless CR. Wheeless` Textbook of RheumatologyOrthopaedics References and Discussions for Physicians. [Online].;1996-2014 [cited 2014 March 25] http://www. wheelessonline. om/ortho/cervical_spondylosis.
20. Hoy DG, Parotani M, De R, Buchbindar R. The Epidemiology of Neck pain. Best Practice & Research Clinical Rheumatology. 2010; 24(6): p. 783-792.
21. Groenewes R, Kropman H, Assen LV, Mulder J, Tulder MW, Oostendrop RA. The Effectiveness and Cost-evaluation of Manual Therapy and Physical Therapy in Patients with Sub-acute and Chronic Non specific Neck pain. Rationale and Design of a Randomized Controlled Trial (RCT). BMC Musculoskeletal Disorder. 2010; 11(14): p. 1-9.
22. Cote P, Carroll L, Cassidy JD. The Epidemiology of Neck Pain: What We Have Learned from Our Population-Based Studies. Journal of Canadian Chiropractic Association. 2003; 47(4): p. 285-290.
23. Colledge NR, Walker BR, Ralston SH. Davidson’s Principles and of Practice of Medicine. 21st ed. Edinburgh: Churchill Livingstone; 2010.1221-1222.
24. Rana SS. Diagnosis and Management of Cervical Spondylosis. Medscape Drug Disease and Procedures. 2013 Jun; p. 1-8.
25. Baghdadi IH. Al-mukhtarat Fit Part-4th. New Delhi: CCRUM, Ministry of Health and Family Welfare.Govt of India; 2007:79.
26. Sina I. Al Qanoon Fit Tib. Vol 3rd (Urdu translation By GH Kantoori). New Delhi: Idarae Kitabus Shifa; YNM: 600- 601,1119-1120,1129.
27. Razi ABMBZ. Kitabul Havi. Vol-11th. New Delhi: CCRUM, Ministry of Health and Family Welfare, Govt of India; 2004: 75-76.
28. Jurjani AH. Zakheerae Khuwarzam Shahi.Vol-6th (Urdu translation by Hk Hadi Hussain). New Delhi: Idare kitabus Shifa; 2010:73-74,637-639
. 29. Ramani PS. Textbook of Cervical Spondylosis. 1st ed. Darya ganj New Delhi: Jaypee Brother Medical publisher; 2004:1,155-160.
30. Anjum N, Jamil S, Hannan A, Akhtar J, Ahmad B. Clinical Efficacy of Hijamat (Cupping) in Waja ul Mafasil Muzmin (arthritis) Indian Journal of Traditional Knowledge.2005 Oct; 4 (4). p 412-415.
31. Nayab M, Anwar M, Quamri M A, Clinical Study on Waja ul Mafasil and Evaluation of Efficacy of Hijamat Bila Shurt in the Treatment, Indian journal of Unani Medicine. 2011 Oct;10 (4):p. 697-701.
32. Nayab M, Ansari M A, Anwar M, Yaseen A, Effect of Hijamat Bila Shart in the Management of Waja uz Zohar - A Clinical Study. Hippocratic Journal of Unani Medicine, 2011Jan-Mar;6 (1): p. 79-86.
33. Siddiqui MA, Quamri MA, Singh B. Effect of Hijamat Bila Shurt in Low Back Pain- An Open Randomized Control Study. RGUHS Journal of AYUSH Science. 2011 June; 1(1): p. 39-44.
34. Sheeraz M, Quamri MA, Ahmed Z. A Comparative Clinical Study on the Effects of Mehjama Nariya (fire cupping) and Hijamat Bila Shurt (dry cupping) in Irqunnasa (sciatica). Spatula DD. 2013; 3(4): p. 161-166.
35. Usmani C. Clinical Study in The Management of Wajaul Mafasil with Unani Formulation .[dissertation].Bangalore: NIUM.RGUHS.2007:65-85.
36. Nafees M, Khan NA, Amin KMY, Ahmad G. Evaluation of Anti inflammatory activity of Habbe Gule Aakh in Albino rats. Hippocratic Journal of Unani Medicine. 2012;7(4): p.1-9.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





