IJCRR - 7(2), January, 2015
Pages: 17-20
Print Article
Download XML Download PDF
NORMAL FUNCTIONING MEDITATIONAL ECTOPIC THYROID - A RARE CASE REPORT
Author: Abdullateef Softah
Category: Healthcare
Abstract:We reported a 34 yrs old who had presented with a huge goiter in the neck and a separate mediastinal huge thyroid mass. He had tracoesophageal compression causing dysphagia and dysphonia. After investigations patient underwent two separate operations. One for Neck goiter and second for the mediastinal goiter. Literature is reviewed
Keywords: Thyrothymus membrane, Mediastinal thyroid tissue, Thyroid gland embryogenesis, Mediastinal tumors
Full Text:
INTRODUCTION
Thyroid is normally located on thyroid cartilage. Ectopic thyroid can be found in the area of descend of thyroglossal duct from foramen cecum and thyroid cartilage Sometimes ectopic thyroid can be found in the mediastinum which is derived from thyroid rest in the thyrothymus membrane. There may or may not be a tissue continuity between the actual thyroid and the mediastinal thyroid tissue. Any of the thyroid tissue at any location can develop into a goiter and produce pressure symptoms. We are presenting a rare case of normal functioning mediastinal ectopic thyroid goiter which presented with dysphagia.
CASE
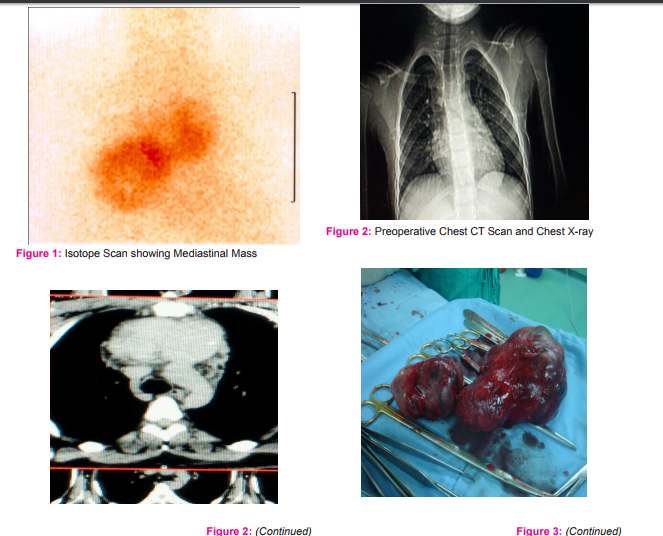
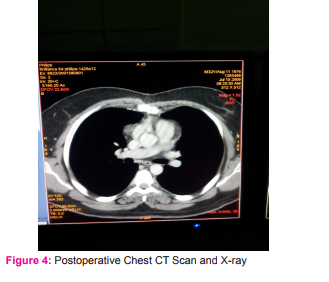
34 yrs old male presented with history of swelling in the neck progressed to big size. The swelling caused dysphagia and dysphonia. On examination the lower border was not seen not felt percussion of manubrium was dull pembuldon’d maneuver caused congestion of face Indirect laryngoscopy showed normal vocal cords movement. Investigations revealed normal T3 T4 TSH normal. Isotope Tc 99 scan showed patchy uptake (Photo 1). CT scan neck and chest revealed compression and deviation of the trachea in neck and huge anterior mediastial multinodular goiter measuring 5X 11X8 cms with dense calcification with few hypodense nodules. The mass had no connection with the proper thyroid goiter in the neck (Photo 2). FNAC report was colloid goiter. As the thyroid was huge compressing airway severely and there was a huge retrosternal mediastinal mass in chest we thought of doing this surgery in two stages. Stage one we planned to operate thro neck incision and relieve the tracheal compression. The lower poles of the goiter were delivered completely but still a separate mass could be felt in the superior mediastinum which was totally separate from the goiter. The second stage was performed after one month. Patient was operated with median sternotomy incision. Intraoperative findings revealed the mass was very vascular and big about 5cmx11cmX8cms in size (Photo 3). It was removed completely comfortably through this incision. Post operative patient had no dysphagia no injury to vital structures (Photo 4). However patient developed hypocalcaemia for which he was treated with oral calcium and vitamin D.
DISCUSSION
Ectopic thyroid tissue is a rare entity resulting from developmental defects at early stages of thyroid gland embryogenesis, during its Descent from the floor of the primitive foregut to its final pre-tracheal position. It is frequently found around the course of the thyroglossal duct. As well as in distant places such as the mediastinum and the subdiaphragmatic.
The sites of ectopic thyroid gland described are lingual, throglossal duct remnants and thyroglossal cyst. Presence of thyroid goiter in mediastinum and brancheal cyst are very rare2 Sometimes thyroid gland can be found in lateral pert of neck due to developmental anomaly. previously it was thought that papillary ca spreads to LN in lateral neck and grows in LN as a ectopic thyroid malignancy but now it has been shown that it is not the metastatic growth but it is a primary malignancy in lateral aberrant thyroid gland.3 Hence it is necessary to differentiate Ectopic thyroid tissue from papillary carcinoma. Very rarely ectopic thyroid malignancy can also be found in brancheal cyst.4 Intrathoracic or Mediastinal thyroid develops from Thyroid Rests Thyroid rests also known as thyrothymic thyroid rests are deposits of thyroid tissue arising in the thyrothymic tract below the thyroid lobes. They cause symptoms such as swallowing or breathing difficulty due to pressure on other structures .The currently accepted definition of an intrathoracic goiter is a thyroid gland with more than 50% of its mass located below the thoracic inlet.5-6 Ectopic intrathoracic thyroid is a rare presentation of thyroid disease and of all Mediastinal tumors.7 It is defined as the presence of enlarged thyroid tissue below the plane of the thoracic inlet. Utilizing the Shield’s classification of the Mediastinum.8 Wakeley and Mulvany in their 1940 seminal report divided intrathoracic thyroid into three types:
(a) “small substernal extension” of a mainly cervical thyroid goiter; (b) “partial” intrathoracic goiter, in which the major portion of the goiter is situated within the thorax; (c) “complete” intrathoracic goiter, in which all of the goiter lies within the thoracic cavity. With an overall incidence of 8.7% for substernal goiters, the incidences of the three types were 81.9%, 15.3%, and 2.7%.9 A report published from Nigeria shows that intrathoracic goiters are mostly located in the anterior and middle Mediastinum, and rarely in the posterior Mediastinal compartment.10 A report from university of Mississippi mentions that Mediastinal thyroid goiters are common on right side of chest and they commonly lie posteriorly. Most of the thyroid goiters can be tackled thro cervical incision but 5 to 10% may require additional incision. For posterior goiters it should be right ant thoracotomy and for anterior goiters it is mid sternotomy. Conversely, a “complete” or “true” intrathoracic goiter is one that is completely within the Mediastinum and separate from a coexisting cervical thyroid gland.1 Thus, the uppermost part is barely palpable in the sternal notch.5 Intrathoracic goiters tend to be attached by a thin piece of thyroid or fibrous tissue to the main body of the gland, but about 20% have no attachment at all and can migrate into the chest, presenting as an unexplained intrathoracic mass. More usually however, they are removed with rest of the thyroid at the time of a total thyroidectomy, via the standard neck incision. If completely separate, then a manubriotomy might be needed to gain access to the mass in the chest for removal.11 Although most intrathoracic goiters can be removed through a cervical incision.11,12-13 In the event that the transcervical surgical approach fails, median sternotomy may be done, particularly if thyroid cancer is suspected or the patient is experiencing acute airway compression. Generally, the decision for a more invasive procedure should be made after careful exploration of the neck and complete exposure of the thyroid.14
CONCLUSION
Although most intrathoracic goiters can be managed by removal through a cervical incision .One may not succeed in getting the thyroid out by neck incision hence preparation of median sternotomy simultaneously or in separate sitting if it is huge and vascular. Standby thoracic surgeon during surgery is essential. Conflicts of interest: None Source of Funding: None
ACKNOWLEDGEMENTS
The authors acknowledge the immense help received fro m the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.

References:
1. Noussios G, Anagnostis P, Goulis DG, Lappas D, Natsis K. Ectopic thyroid tissue: anatomical, clinical, and surgical implications of a rare entity. Eur J Endocrinol. 2011 Sep;165(3):375-82. doi: 10.1530/EJE-11-0461. Epub 2011 Jun 29.
2. Kay DJ, Meyers AD. Embryology of the Thyroid and Parathyroids. Thyroid Embryology Clinical Correlations. Emedicine. Updated: Jan 14, 2010.
3. Johnson RWP, NC. The So-called Lateral Aberrant Thyroid Br Med J. 1962 June 16; 1(5293): 1668–1669.
4. Karras S, Anagnostis P, Noussios G, Pontikides N. Thyroid papillary carcinoma arising in ectopic thyroid tissue within a branchial cleft cyst. BMJ Case Rep. 2013 Apr 22;2013. pii: bcr2013009312. doi: 10.1136/bcr-2013-009312.
5. deSouza FM, Smith PE. Retrosternal goiter. J Otolaryngol1983;12:393-6.
6. Netterville JL, Coleman SC, Smith JC, et al. Management of substernal goiter. Laryngoscope1998;108:1611-7.
7. Shields TW. The Mediastinum, Its Compartments, and the Mediastinal Lymph Nodes. Shields, TW. General Thoracic Surgery. 2005. Sixth Edition. Chapter 154, 2343-2346
8. Hedayati N, McHenry CR. The clinical presentation and operative management of nodular and diffuse substernal thyroid disease. Am Surg 2002;68:245-52.
9. Sakorafas GH, Vlachos A, Tolumis G, Kassaras GA, Anagnostopoulos GK, Gorgogiannis D. Ectopic intrathoracic thyroid: case report. Mt Sinai J Med 2004;71:131-133
10. degboye VO, Ogunseinde OA, Obajimi MO, Ladipo JK, Brimmo AI. Pattern of intrathoracic goiter in Ibadan, Nigeria. Niger Postgrad Med J 2002;9:226-232.
11. Johnston JH Jr, Twente GE. Surgical approach to intrathoracic (mediastinal) goiter. Ann Surg. 1956 May;143(5):572- 9.
12. Shaha AR, Alfonso AE, Jaffe BM. Operative treatment of substernal goiters. Head Neck1989;11:325-30.
13. Lahey FH, Swinton NW. Intra-thoracic goiter. Surg Gynecol Obstet1934;59:627-37.
14. Pace-Asciak P, Higgins K. Management of intrathoracic goiter. Can J Surg. 2008 October; 51(5): E111–E112. PMCID: PMC2556542.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





