IJCRR - 9(8), April, 2017
Pages: 30-35
Date of Publication: 01-May-2017
Print Article
Download XML Download PDF
Congenital External Ear Deformity and Their Hearing Rehabilitation With Bone Anchored Hearing Aid: A Retrospective Analysis
Author: Hetal Marfatia, Ratna Priya
Category: Healthcare
Abstract:Objectives: Microtia-anotia is a spectrum of congenital anomalies of the auricle ranging from mild structural abnormalities to complete absence of the ear. Early amplification, auditory training, and speech therapy can improve speech and language development.
Materials and Methods: Case Records of 30 patients with congenital external deformity during the time period from January 2010 to June 2013 were reviewed for the grade of microtia, the degree and type of hearing loss and hearing rehabilitation.
Results: Out of 30 patients, 22 patients were given hearing rehabilitation either in the form of bone anchored hearing aid \? soft -band or Baha implant. 9 patients underwent Baha surgery. Mean post rehabilitation improvement was 23.4 dB. Closure of the air- bone gap was observed in one patient.
Conclusion: Baha is an excellent option for hearing rehabilitation in patients with congenital conductive hearing loss.
Keywords: Microtia-anotia, Baha softband, Baha surgery, Osseointegration, Rehabilitation
Full Text:
Introduction
Microtia-anotia is a spectrum of congenital anomalies of the auricle ranging from mild structural abnormalities to complete absence of the external ear (anotia). It may occur as an isolated condition, or as part of a spectrum of anomalies or a syndrome. The prime concern in the young child is the assessment and improvement of hearing. Early amplification, auditory training, and speech therapy can improve speech and language development.
Ours is a retrospective study of patients with congenital external ear deformity and their hearing rehabilitation. Medical records of 30 patients who presented during the period from January 2010 to June 2013 were evaluated.
Materials and methods
Case Records of patients with congenital external deformity who presented to the E.N.T. Department during the time period from January 2010 to June 2013 were reviewed for the grade of microtia, the degree and type of hearing loss and hearing rehabilitation. Hearing evaluation was done by behavioural audiometry and pure tone audiometry (PTA). BC BERA was done to rule out sensorineural hearing loss.
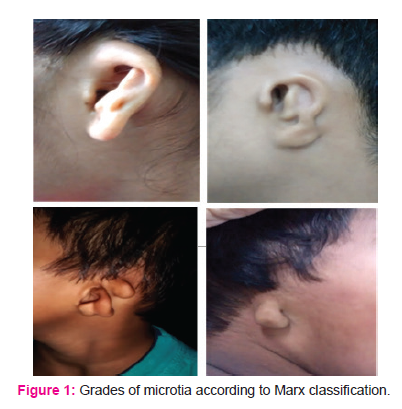
According to Marx classification, the deformity was graded.(Figure 1) All these patients underwent Baha trial with Baha Divino, BP 100 or Baha Intenso depending on the hearing loss using headband or softband. Patients with bone thickness less than 3 mm and children less than 5 years of age were given Baha soft band and others were considered for surgery.
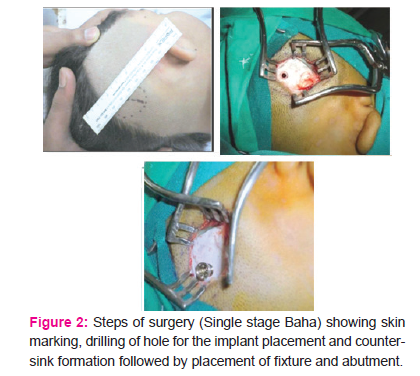
Baha surgery was done under general anaesthesia. The Linear Incision technique was used.2-6The implant site was positioned 6-6.5cm from the ear canal. A 3 cm incision was made through the periosteum at the hairline to expose the planned implant site. Approximately 1 cm of the periosteum was elevated around the site. A 3mm deep guide hole was drilled at that site (at 2000 rpm); Drill indicator was used to keep the insertion strictly 90 degree to the bone. The hole was enlarged slowly, carefully inspecting the bone. Continuous irrigation was provided to avoid thermal injury to osteoclasts. If the bone thickness was more than 3mm then spacer was removed and 4 mm drilling was done. The guide hole was used to align a countersink burr, which widened the guide hole and created a shallow countersink in the adjacent bone surface. A self tapping titanium bone screw with attached abutment (the percutaneous part to which a processor would be affixed 2 to 3 months postoperatively) was carefully picked up with an abutment inserter and then advanced to full depth at a slow revolution rate and controlled insertion torque of 20-30Ncm which was slowly increased to 40-50Ncm . First turn of the implant was placed without irrigation and later continuous irrigation was done for cooling. Soft tissue reduction was done all around. Skin wound edges were sutured to underlying periosteum to coapt dead space; the skin flap was sutured back in its original position. Healing cap was placed and compression dressing using umbilical tape was given for 7 days. Suture removal was done after seven days and Patients were kept on regular two weekly follow up. ( Figure 2) After waiting for 3-6 months (depending on bone quality) for osseointegration the Baha processor was snapped on to the abutment and the hearing improvement was documented using pure tone audiometry and plotted as Baha aided audiogram. (Figure 3)
Results
In our study mean age of the patients was 13.33 years ranging from 3 months to 31 years of age and a male: female ratio was 4:1. Bilateral congenital microtia – anotia was found in 53.3% of patients compared to unilateral microtia – anotia in 46.7% of cases.(Table1)Among the 14 unilateral cases, out of total 30, right sided deformity was found in 64.3% of patients. The distribution of patients showed male predominance.( Table 2) Grade III microtia was the most common congenital external ear malformation in our study. External auditory canal atresia is present in 83% of cases. Conductive hearing loss was most common type of hearing loss being present in 86.7% subjects. (Figure 4) Maximum number of subjects with grade III microtia fell in the hearing threshold of moderately – severe hearing loss i.e.55-70 decibels. Rest 13.3% of subjects had presented with mixed hearing loss. Pure sensorineural hearing loss was seen in one patient. ( Table 3)
Out of 30 patients, 22 patients were given hearing rehabilitation either in the form of bone anchored hearing aid – soft -band or Baha implant. 9 patients underwent Baha surgery. Out of the nine patients, 7 underwent single staged procedure. The side of the implantation was decided on the cochlear function, temporo-parietal suture line thickness as well as on the handedness of the patient. Among the nine implanted patients, 8 underwent right sided surgery and one left sided surgery as on the right side patient complained of discharge from the redundant EAC.
13 patients were given Baha- soft-band for amplification of hearing among which 6 were infants who were given soft- band for early language development. Rest of the 7 patients were given Baha- soft band till they were arranging funds for Baha- surgery
It was observed that 5 patients with unilateral microtia with mild to moderate conductive hearing loss did not opt for Baha soft band or implant, as the other ear was completely normal and they could manage with unilateral hearing loss. 3 patients had bilateral profound hearing loss that did not have any benefit following Baha trial.
The mean pre- rehabilitation air- bone gap of all 22 patients was 50.9 Db ± 10.5 dB. Post rehabilitation Baha aided air bone gap, after 3 months of use, was 27.5 dB ± 11.2 dB. Mean post rehabilitation improvement, calculated by subtracting mean post rehabilitation Baha aided threshold from mean pre rehabilitation air conduction threshold, was 23.4 dB. Closure of the air- bone gap was observed in one patient. Thus, bone anchored hearing aid is a reliable method of rehabilitation in patients with congenital external ear deformity.
The complications observed were skin infection (Holgers grade 2)( Figure 5) around the site of implant in two patients. This settled following two weeks of oral antibiotic and meticulous wound care and cleaning. One of the patients developed skin overgrowth due to more thickness of scalp (Holgers grade 4) and also the abutment height was inadequate. The patient had to undergo revision surgery to replace the abutment. And one of the patients underwent failure of osseointegration and was reimplanted later on the opposite side.
Discussion
Microtia is found in approximately 0.03 percent of all newborn infants.1 It is associated with atresia or stenosis of the external auditory canal and frequently with ossicular abnormalities. The etiology of microtia-anotia is poorly understood. There is strong evidence supporting the significance of environmental causes for microtia-anotia, such as altitude and gestational exposure to retinoid, alcohol, thalidomide and, mycophenolatemofetil. In many cases it occurs as a mutation without any precipitating factors. However, none of our patients had any of the above predisposing factors or any positive family history.
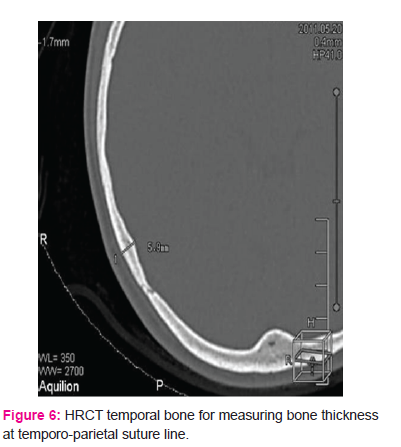
The recommended tests for hearing evaluation are pure tone audiometry (PTA), BC BERA (Brainstem-evoked response audiometry) and Behavioural Audiometry. A HRCT scan was done to determine the anatomy of the bony structures and middle and inner ears and bone thickness which is usually measured behind the temporo-parietal suture line. ( Figure 6)
In order to characterise the severity of microtia, many grading systems have been developed. We followed Marx’s microtia classification.7 Grade III microtia was the most common congenital external ear malformation in our study. External auditory canal atresia is present in 83% of cases.
Microtia surgery is technically difficult, and not infrequently, the results are somewhat disappointing. The surgery should be performed by individuals with special expertise.5 Auricular reconstruction is an elective procedure. The deformity can usually be masked by a longer hair style. Generally, the slight deformity of a grade I microtia may be cosmetically acceptable.1 Reconstruction of a moderately deformed grade II microtia must be individualized. Correction of a severe grade III microtia may require multiple surgery as well as need for additional incision on chest for rib graft. Ear prosthesis can also be an option for some individuals with microtia-anotia.1 There can be difficulties in matching the appearance of the other ear, and it is just for cosmesis.
Congenital conductive hearing loss caused by a malformation of the middle or external ear resulting in external auditory canal atresia is effectively managed with a Bone Anchored Hearing Aid (Baha). Such people have option of bone conduction hearing aids but they have to be worn on the head using a steel spring headband or included in the frame of a pair of glasses, hence they are uncomfortable as patients complain of pain and headaches due to the constant pressure of the headband, cumbersome, obtrusive and insecure.8 Also, the sound quality is poor as the skin acts as a barrier for the sound to travel to the inner ear. The Baha system can be a real solution for people with this type of impairment. The Baha implant is directly integrated to the skull bone. Because of this direct interface, the Baha offers significantly better sound quality than that of a traditional bone conductor. The Baha sound processor works without pressure on the skin avoiding headache and soreness associated with the conventional bone conductor. Baha offers excellent wearing comfort and a better aesthetic result.8 The surgery can only take place once the skull is at least 2.5 mm thick.9 In the meantime the child with bilateral atresia can be fitted with a soft band around the head called the Baha soft band; these are available in colourful patterns. This is offered at the age of 3-6 month. These small babies often tolerate this arrangement very well.10
The Baha is a surgically implantable system for treatment of hearing loss that works through direct bone conduction. It has been used since 1977, and was cleared by the FDA in 1996 as a treatment for conductive and mixed hearing losses in the United States. It consists of three components: a titanium implant, an external abutment and an electronic sound processor.
The pioneering work in osseointegration was done by Branemark et al.11 in 1965. Nine years later, Tjellstrom et al12 introduced the concept of direct bone conduction using a skin-penetrating coupling from an osseointegrated titanium implant in the mastoid bone.9 Tjellstrom and Granstrom13 modified the original technique of two staged procedure into a single-stage procedure.
Baha is used for conductive or mixed hearing loss with good cochlear reserve. It is a very effective hearing option for children with conductive hearing loss.14-16 The major limitation is the relative thinness of the paediatric skull (average 3mm) which requires shorter screw lengths. Also, the surgeon is faced with continuous growth of the skull, and the fact that the majority of children who are candidates for this type of hearing aid often have abnormal skull contour.17-19
In our retrospective review of 30 cases of congenital external ear deformity, we found that bilateral microtia – anotia is more common compared to unilateral variety, as those with bilateral condition seek for the help more often. Patients with bilateral hearing loss warrant early intervention to prevent delay in development of speech. Hearing amplification is provided either by Baha band or Baha surgery, depending on age and bone thickness. Also, patients with Baha band can be later considered for surgery.
Patients with bilateral profound mixed hearing loss cannot be benefitted by using Baha and are candidates for cochlear implants. Even cochlear implant is challenging due to associated middle and inner ear anomalies. Baha surgery can be done either as single staged or double staged depending on age and bone thickness. In case the required thickness is less than 3 mm, then two-staged surgery is planned. However, even patients with adequate bone thickness may have soft bone, demanding staged procedure. The mean improvement in our series was 23.4 dB. The Closure of the air- bone gap was observed in one patient. Thus, we can conclude that Baha is a reliable method of rehabilitation in patients with congenital external ear.
The risks associated with Baha surgery were skin infection around the site of implant seen in 1 out of 9 implanted patients, skin overgrowth in 1 patient and Baha extrusion in 1 patient.
Conclusion
Hence in this retrospective analysis we conclude Baha is an excellent option for hearing rehabilitation in patients with congenital conductive hearing loss. Candidates for Baha band are children less than 5 years of age, those with bone thickness less than 3mm and the ones awaiting Baha surgery. Surgical outcome doesn’t change whether we do a single or a staged procedure. Baha is proved to be one of the simplest surgery to perform and the easiest to fail if the surgery is not done meticulously and the implant is not perpendicular to scalp.
Acknowledgement: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Disclosure of potential conflicts of interest: None of the authors have any conflict of interest
Ethical approval: All procedures performed were in accordance with the ethical standards of the·institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed consent: Informed consent was obtained from the patient included in this study.
Role of funding source: None




References:
1) Simon C. Parisier MD, Jose N. Fayad MD, Charles P. Kimmelman MD.Microtia, Canal Atresia, and Middle Ear Anomalies. Ballenger’s Otorhinolaryngology and Head and neck surgery (16th edition): 997-1008.
2) van der Pouw CT, Mylanus EA, Cremers CW. Percutaneous implants in the temporal bone for securing a bone conductor: surgical methods and results. Ann Otol Rhinol Laryngol. 1999 Jun; 108(6):532-6.
3) de Wolf MJ, Hol MK, Huygen PL, Mylanus EA, Cremers CW. Clinical outcome of the simplified surgical technique for Baha implantation. Otol Neurotol. 2008; 29(8):1100-8.
4) de Wolf MJ et al. Nijmegen results with application of a Bone-Anchored Hearing Aid in children: Simplified Surgical Technique Ann Otol Rhinol Laryngol. 2008; 117(11):805-14.
5) Bovo R. Simplified technique without skin flap for the bone-anchored hearing aid
(Baha®) implant Acta Otorhinolaryngol ItaI 2008; 28:252-255.
6) Wilkinson EP, Luxford WM, Slattery WH, De la Cruz A, House JW, Fayad JN. Single vertical incision for Baha implants surgery: Preliminary results. Otolaryngology-Head and Neck surgery 2009, 1401 573-578.
7) Samuli Suutarla microtia academic dissertation department of Otorhinolaryngology University of Helsinki Finland and cleft and craniofacial centre Helsinki University Hospital, Finland 2014.
8) Baha implant University of Maryland Medical Centre umm.edu/programs/hearing/services/bone-anchored-devices. Jul 15, 2014
9) Tjellstrom A, Hakansson B. The bone anchored hearing aid (BAHA) design principles, indications and long-term clinical results. Otolaryngol Clin North Am 1995; 115:1–20.
10) Papsin BC, Sinmanna TK, Albert DM, Bailey CM. Surgical experience with bone-anchored hearing aids in children. The Laryngoscope, 1997: 104(6):801-6.
11) Branemark PI, Adell R, Breine U, Hansson BO, Lindstrom J, Ohlsson A. Intra-osseous anchorage of dental prostheses. I. Experimental studies. Scand J Plast Reconstr Surg. 1969; 3(2):81–100.
12) Tjellstrom A, Hakansson B, Lindstrom J, Branemark PI, Hallen O, Rosenhall U, et al. Analysis of the mechanical impedance of bone-anchored hearing aids. Acta Otolaryngol. 1980; 89(1–2):85–92.
13) Tjellstrom A, Granstrom G. One-stage procedure to establish osseointegration: a zero to five years follow-up report. J Laryngol Otol. 1995; 109(7):593–598.
14) Papsin BC, Sirimanna TK, Albert DM, Bailey CM. Surgical experience with bone-anchored hearing aids in children. Laryngoscope. 1997; 107(6):801–806.
15) Powell RH, Burrell SP, Cooper HR, Proops DW. The Birmingham bone anchored hearing aid programme: paediatric experience and results. J Laryngol Otol Suppl. 1996; 21:21–29.
16) Stevenson DS, Proops DW, Wake MJ, Deadman MJ, Worrollo SJ, Hobson JA. Osseo integrated implants in the management of childhood ear abnormalities: the initial Birmingham experience. J Laryngol Otol.1993; 107(6):502–509. nchored hearing aids in children. Laryngoscope. 1997; 107(6):801–806.
17) Tjellstrom A, Granstrom G. One-stage procedure to establish osseointegration: a zero to five years follow-up report. J Laryngol Otol. 1995; 109(7):593–598.
18) Granstrom G, Tjellstrom A. The bone-anchored hearing aid (BAHA) in children with auricular malformations. Ear Nose Throat J. 1997; 76(4):238–7.
19) Granstrom G. Osseo integrated implants in children. Acta Otolaryngol Suppl. 2000; 543:118–121.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





