IJCRR - 7(3), February, 2015
Pages: 39-42
Print Article
Download XML Download PDF
AN AGGRESSIVE PRESENTATION OF EXOPHYTIC MARJOLIN'S ULCER AND IMPORTANCE OF RADIOTHERAPY IN ITS TREATMENT
Author: Ravindra Nandhana, Sivasankar Kotne, PB Anand Rao, Surendra Manam, SPV Turlapati
Category: Healthcare
Abstract:Marjolin's ulcer is a rare squamous cell cancer that is most often associated with chronic burn wounds. Wide local excision or amputation remains the first treatment of choice. We present here a case of squamous cell carcinoma of thumb in a 39 year old female. In view of aggressive spread to regional nodes we feel the need for thorough evaluation of regional lymph nodes before
surgery and consider adjuvant concomitant chemoradiation and need to include infraclavicular (deltopectoral) lymph nodes in treatment volume in view of direct drainage of lymphatics from thumb malignancy.
Keywords: Chronic fistulas, Exophytic papillary carcinoma, Cell carcinoma
Full Text:
INTRODUCTION
Marjolin’s ulcer is a malignant tumor that usually develops in a chronic skin lesion (especially burn scars in 75% cases, also include vaccination scars, venous stasis ulcers, chronic fistulas and osteomyelitis scars, etc.).(1) Pathologically most of cases are squamous cell carcinoma, few cases are basal cell carcinoma and malignant melanoma.(2) The incidence of burn scar undergoing malignant transformation has been reported to be 0.77 – 2 %.(3)Marjolin’s ulcer is of two clinical types – 1) flat, indurated, infiltrative, ulcerative carcinoma (most common) and 2) exophytic papillary carcinoma. Exophytic form is infrequent and generally less severe with low probability of metastasis. Well differentiated exophytic lesions have a better prognosis than poorly differentiated infiltrating forms. When confined to scar the growth is slow and it can be completely cured. Once it breaks free of scar it metastasizes rapidly to the regional nodes.(4)
CASE REPORT
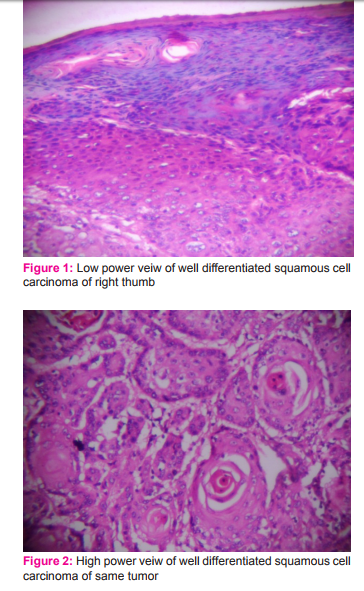
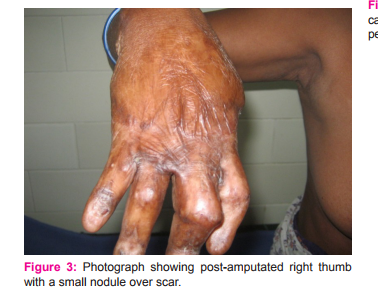
We present here a case of marjolin’s ulcer of right thumb in a 39 year old female. She initially presented to a private practitioner with complaints of large exophytic growth on dorsal aspect of distal phalange of right thumb on a 15 year old post burn scar. She underwent amputation of thumb. Histopathology reported as well differentiated squamous cell carcinoma invading into underlying tissues (Figure 1 and 2). One month after surgery she developed axillary lymph nodes and a small ulcerated lesion at the surgical site for which she was referred to GSL Medical College, Rajahmundry Andhra Pradesh (Figure 3 and 4). In view of axillary lymph node metastasis and local recurrence, revision amputations of 1st metacarpal and axillary lymph node dissection were performed. Histopathological examination showed negative margins with squamous cell carcinomatous deposits in right axillary lymph nodes (Figure 5). By the time patient planned for adjuvant radiotherapy she developed infraclavicular swelling(Figure 6). Hence excision of right infraclavicular lymph node was done. Histopathological examination showed squamous cell carcinomatous deposits in right infraclavicular lymph nodes (Figure 7). In view of rapid progression adjuvant radiotherapy was given to right axillary, infraclavicular and supraclavicular regions. Patient is under follow-up for last 6 months without any further recurrence.
DISCUSSION
Etiology of marjolin’s ulcer is not yet clear.(5) Squamous cell carcinomas resulting from the marjolin’s ulcer have a greater tendency to metastasis than squamous cell carcinoma resulting from other causes. Poorly differentiated squamous cell carcinomas have a greater tendency to spread to lymph nodes earlier. Regional node metastasis and recurrence after surgery is not uncommon. Metastasis to regional lymph nodes is seen in 30% cases and local recurrence occurs in 17% cases.(6) Surgery (wide local excision or amputation) is remains the first treatment of choice. Marjolin’s ulcer should be excised with a 2 cm margin of normal healthy tissue (which may necessitate amputation with lesion involving joint space).(7) Sentinel lymph node biopsy is recommended in patients with squamous cell carcinoma. Lymph node block dissection should be done if nodes are clinically palpable or sentinel lymph node biopsy positive and analyzed pathologically. Prophylactic lymph node resection has not been recommended.(8) radiotherapy is not indicated because of poorly vascularized tumor tissue. Radiotherapy must be used as an adjuvant therapy only and should not replace aggressive resection. Indications of radiotherapy include 1) Inoperable lymph node metastasis, 2) high grade lesions with positive lymph nodes after regional lymph node dissection (RLND), 3) Tumor diameter greater than 10 cm, with positive lymph nodes after RLND, 4) High grade lesions, with tumor diameter greater than 10 cm and no positive lymph nodes after RLND, 5) Lesions of head and neck, with positive lymph nodes after RLND.(9)
CONCLUSION
In view of aggressive spread to regional nodes we feel the need for thorough evaluation of regional lymph nodes before surgery and consider adjuvant concomitant chemoradiation and need to include infraclavicular (deltopectoral) lymph nodes in treatment volume in view of direct drainage of lymphatics from thumb malignancy.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/ editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.


References:
1. Wojciech MW, Andrzej LK, et al. Two Different Cases of Marjolin’s Ulcer and Recommendations for Practice. The Open Surgical Oncology Journal, 2010; 2: 83-85.
2. Interesting Case Series, Chronic Ulcer. Correspondence: williamaboumd@hotmail.com William Abouhassan, MD, Johns Hopkins Burn Center, Johns Hopkins University, Baltimore, Md.
3. Copcu, Eray. Marjolin’s Ulcer: A Preventable Complication of Burns? Plastic & Reconstructive Surgery, July2009; 124(1): 156e-164e.
4. Aydogdu E, Yildirim S, Akoz T. Is surgery an effective and adequate treatment in advanced Marjolin’s ulcer? Burns. Jun2005; 31(4):421-31.
5. Ifeanyi IO, BismarkOkwor, Wilson IBO. Penetrating scalp Marjolin’s ulcer involving bone and dura mater in a Nigerian hospital: Case report and literature review. Burns (2009), doi:10.1016/j.burns.2009.04.010.
6. Dr A. Ero?lu, S. Çamlibel. Risk factors for locoregional recurrence of scar carcinoma British Journal of Surgery 1997; 84(12): 1744–6.
7. AbdolazimGhalambor. Marjolin ulcer: How much of safety margin needs resection along marjolin ulcer squamous cell carcinoma in recurrence cases Pak J Med Sci MayJune 2007; 23(3): 394-397.
8. Eastman AL, Erdman WA, Lindberg GM, Hunt JL, Purdue GF, Fleming JB. Sentinel lymph node biopsy identifies occult nodal metastases in patients with Marjolin’s ulcer. J Burn Care Rehabil. 2004; 25(3): 241- 245.
9. Ozek C, Cankayali R, Bilkay U, Cagdas A. Marjolin’s ulcers arising in burn scars. J Burn Care Rehabil 2001;22:384-9
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





