IJCRR - 7(3), February, 2015
Pages: 08-12
Print Article
Download XML Download PDF
FISSURES AND LOBES OF LUNG - AN ANATOMICAL STUDY AND ITS CLINICAL SIGNIFICANCE
Author: Amit Magadum, Daksha Dixit, Shilpa Bhimalli
Category: Healthcare
Abstract:Introduction: The fissures facilitate the movement of the lobes in relation to one another, which accommodates greater distention and movement of the lobes during respiration. The fissures may be complete, incomplete or absent altogether. Aim of the Study: To study the morphology of fissures and lobes, to note the variations, to compare them with previous studies and to find their clinical significances. Materials and Methods: Forty pairs of lungs obtained from formalin-fixed adult cadavers removed during routine dissection at J. N. Medical College, Belagavi were studied. These lungs were meticulously observed for the patterns of lobes and fissures, variations were noted and photographed. Results: In the present study oblique fissure was absent in 10% of right lungs and 7.5% of left lungs. Incomplete horizontal fissure was seen in 52.5% of right sided lungs. Conclusion: This study also shows that parenchymal fusion of various extents is a very common entity of oblique fissure of lung. This implies that a variety of genetic and environmental factors might affect development of these fissures.
Keywords: Cadavers, Lobectomy, Fissure, Parenchymal fusion
Full Text:
INTRODUCTION
The lungs are the essential organs of respiration. Fissures are an integral part of human lung. Right lung has 2 fissures; oblique and horizontal, dividing it into superior, middle and inferior lobes. Left lung has only oblique fissure dividing it into superior and inferior lobes1 . The lung fissures ease the movement of the lobes, which helps in greater distention and movement of the lobes during respiration2 . Thus, they help in a more uniform expansion of the whole lung. The fissures may be complete, when the lobes remain held together only at the hilum by the bronchi and pulmonary vessels, or they may be incomplete when there are areas of parenchymal fusion between the lobes, or, they may be absent altogether2 . In the region of an incomplete fissure, the adjacent lobes are connected by a sizeable chunk of pulmonary tissue as the cleft fails to reach the hilum. Parenchymal fusion of varied extent along the floor is also found in case of incomplete fissures3 . Accessory fissures of the lung are commonly observed in lung specimens, but are often unappreciated or misinterpreted on radiographs and computerized tomographic (CT) scans4 . Anatomically, an accessory fissure is a cleft of varying depth lined by visceral pleura. These accessory fissures usually occur at the boundaries of the broncho-pulmonary segments. As per Godwin, the most common accessory fissures are the inferior accessory fissure4 . Radiologically an accessory fissure appears as a thin white line, resembling the major or minor fissure, except for its location4 . A fissure appearing complete on X-ray might be seen as an incomplete one on CT scan5 . The knowledge of anatomical variations of the lobes and fissures of lung is important for identifying broncho-pulmonary segments and surgical resections involving individual segments.
AIM OF THE STUDY
Aim of the present study was to examine lung specimens with respect to the morphology of fissures and lobes, to note the variations, to compare them with previous studies and to find their clinical significances.
MATERIALS AND METHODS
Forty pairs of lungs obtained from formalin-fixed adult cadavers removed during routine dissection at J. N. Medical College, Belagavi were studied. The specimens having pathological lesions, marks of previous surgery, and those that were damaged during removal were excluded from the study. Of the 80 lung specimens, 40 were of the right side and 40 were of the left. These lungs were examined for the patterns of lobes and fissures. Later, variations in these lungs were observed and photographed. The anatomical classification based on the degree of completeness of the fissures proposed by Craig and Walker6 was followed to determine the presence and completeness of fissure (table 1).
RESULTS
The observations regarding incidence of oblique and horizontal fissures are shown in table 2. Figure 1 shows absence of horizontal fissure & grade 3 oblique fissure in right lung. Grade 3 horizontal fissure of right lung is seen in figure 2. Accessory fissures of lung are shown in figure 3, 4 and 5.
EMBRYOLOGICAL BASIS:
In prenatal life fissures separate individual broncho-pulmonary segments. All fissures gradually get obliterated. The fissures along the inter-lobar planes persist and give rise to major (oblique) and minor (horizontal) fissures7 . Absence or incompleteness of a fissure could be due to obliteration of these prenatal fissures either completely or partially. Incomplete fissures indicate partial fusion between lobes. Accessory fissures could be the result of non-obliteration or persistence of the prenatal fissures. Any variation in the morphological pattern of the fissures indicates variations from normal pattern of development of lung8 .
DISCUSSION
The present study showed that, in majority of cases the fissures were incomplete, more on the right side than on the left (Table 2). These findings were compared with those of other studies as shown in table 4. Increased incidence of incomplete oblique fissures on the right side might indicate early commencement of fusion of the prenatal fissures which may proceed further before birth, leading to fusion along floor of the oblique fissure9. Table 4 shows wide variability which may be due to the regional variation. In the present study oblique fissure was absent in 10% of right lungs and 7.5% of left lungs. Dutta S et al9 reported absence of oblique fissure in 11.4% of right lungs and 8% of left. But Medlar EM et al 10 reported absence of oblique fissure as 4.8% and 7.3% in specimens of right and left lungs respectively. These results do not match with our data as oblique fissure was absent more on the right side.
Surgically the gradation of fissure is important. The surgeon approaches to ligate the vessels and bronchi through the depth of the fissure. Grade 1 oblique fissure facilitates the approach while doing lobectomy and video assisted thoracoscopic surgery15. But otherwise the lung parenchyma has to be dissected to reach those structures leading to intra-operative hemorrhage and more postoperative complications16. On the other hand, while performing right upper lobectomy, middle lobe has the chance of undergoing torsion if the oblique fissure is of grade 1 variety. So, preventive fixation of the middle lobe is essential to avoid this complication17. An incomplete fissure is also a cause for postoperative air leakage during lobectomies6. In the present study incomplete horizontal fissure was seen in 52.5% of right sided lungs which was comparable with the results of study done by Prakash et al13 (50%). The presence of fissures in normal lung enhances uniform expansion, and their position could be used as reliable landmarks in specifying lesions within the thorax, in general, and within the lungs in particular18. Accessory fissures of the lung are commonly observed in lung specimens, but are often unappreciated or misinterpreted on radiographs and CT scans. In the present study superior accessory fissures were observed more commonly on the left side (3 specimens) than on the right side (1 specimen). Also, in our study we found 2 inferior accessory fissures in right sided lungs. Accessory fissures can be mistakenly confused with areas of linear atelectasis, pleural scars, or walls of bullae4 . In patients with endobronchial lesion, an accessory fissure might alter the usual pattern of lung collapse and pose difficulty in diagnosing a lesion and its extent. Pneumonia in a particular lobe is contained within the confines of the lobe by complete fissures. In patients with incomplete fissures, pneumonia may spread to adjacent lobes through the parenchymal continuation19.
CONCLUSION
The results of present study and its comparison with the previous studies showed a wide range of difference in occurrence of fissures among different populations. This implies that a variety of genetic and environmental factors might affect development of these fissures. This study also shows that parenchymal fusion of various extents is a very common entity in oblique fissure of lung.
ACKNOWLEDGEMENT
The authors are highly thankful to the KLE University’s J. N. Medical College, Belagavi, for providing the necessary support and infrastructure facility to carry out this study. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of Funding: Nil
Conflict of interest: Nil

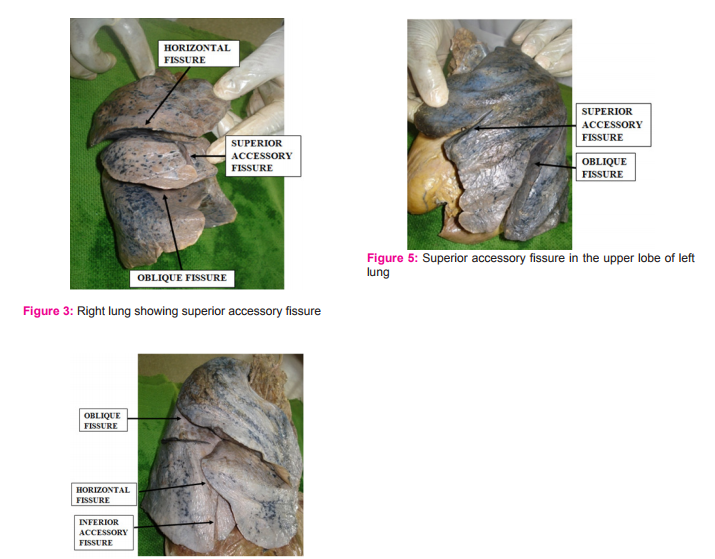
Figure 4: Right lung showing Inferior accessory fissure
References:
1. Gatzoulis M A. Thorax. In: Gray’s Anatomy. 40th ed. Edinburg: Churchill Livingstone: 2008, p.993-94.
2. Meenakshi S, Manjunath K.Y, Balasubramanyam V. Morphological variations of the lung fissures and lobes. Indian J. Chest Dis Allied Sci 2004; 46: 179-182.
3. Rosse C, Gaddum-Rosse P. Hollinshed’s Textbook of Anatomy. Philadelphia: Lipincott-Raven; 1997: 441-61.
4. Godwin JD, Tarver RD. Accessory fissures of the lung. Am J Roentgenol.1985;144:39-47.
5. Berkmen T, Berkmen YM, Austin JH. Accessory fissures of the upper lobe of the left lung: CT and plain film appearance. Am J Roentgenol 1994;162: 1287-93.
6. Craig SR, Walker WS. A proposed anatomical classification of the pulmonary fissures. J R Coll Surg (Edin).1997;42: 233-34.
7. Larsen WJ. Human Embryology. New York: Churchill Livingstone; 1993; p.111-30.
8. Modgil V, Das S, Suri R. Anamolus lobar pattern of right lung: a case report. Int. J. Mophol. 2006; 24: 5-6.
9. Dutta S, Mandal L, Mandal SK, Biswas J, Ray A, Bandopadhyay M. Natural fissures of lung- anatomical basis of surgical techniques and imaging. Nat J Med Res. 2013; 3(2): 117-21.
10. Medlar EM. Variations in interlobar fissures.AJR. 1947; 57 :723-25.
11. Lukose R, Paul S, Sunitha DM, et al. Morphology of the lungs: variations in the lobes and fissures. Biomedicine 1999;19:227-32.
12. Bergman RA, Afifi AK, Miyauchi R. Variations in peripheral segmentation of right lung and the base of the right and left lungs. In: Illustrated Encyclopedia of Human Anatomic Variation.http://www.anatomyatlases.org/AnatomicVariants/OrganSystem/Text/LungsTrachea.shtml (28th of November, 2010).
13. Prakash, Bhardwaj AK, Sashirekha M, Suma HY, Gowtham Krishna G, Singh G. Lung Morphology: a cadaveric study in Indian Population. Ital J Anat Embryol. 2010; 115(3): 235- 40.
14. Nene AR, Gajendra KS, Sarma MVR. Lung lobes and fissures: a morphological study. Anatomy 2011; 5: 30-38.
15. Jennifer M.J. Richards, Joel Dunning, Jonathan Oparka, Fiona M. Carnochan, William S. Walker. Video–assisted thoracoscopic lobectomy:The Edinburg posterior approach. Annals of Cardiothoracic Surgery.2012;1(1).
16. John A.Waldhausen,William S.Pierce, David B.Campbell. Thoracic Surgery.In: Surgery of the Chest. 6th ed. Mosby,St Louis,Missouri.1996. p.134.
17. Pimpec-Barthes F L, Arame A, Pricopi C, Riquet M. Prevention of middle lobe torsion or bronchial plication using anti-adhesive membrane: a simple,safe and uncomplicated technique. Eur J Cardiothoracic Surg.2011;39(6):1059- 1069.
18. Kent EM, Blades B. The surgical anatomy of the pulmonary lobes. J Thoracic Surg.1942; 12 : 18-30.
19. Tarver RD. How common are incomplete pulmonary fissures, and what is their clinical significance? ARJ Am J Roentgenol.1995;164:761.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





