IJCRR - 7(5), March, 2015
Pages: 13-20
Print Article
Download XML Download PDF
CLINICO-BACTERIOLOGICAL PROFILE AND ANTIBIOTIC SENSITIVITY PATTERN OF NEONATAL SEPTICAEMIA- A PROSPECTIVE OBSERVATIONAL STUDY
Author: Dipak Madavi, Farookh Aziz, Gopal Agrawal
Category: Healthcare
Abstract:Context: Neonatal septicaemia is most common cause of morbidity and mortality in NICU in developing countries with emergence of antibiotic resistant organisms. For effective management of neonatal septicaemia cases and to formulate antibiotic
policy for NICU, blood culture is most important investigation.
Aims: This study was carried out to study clinical, microbial profile and antibiotic sensitivity pattern of neonatal septicaemia at our institute.
Settings and Design: Present study was a prospective observational study, carried out in the Department of paediatrics, IGGMC Nagpur. Methods & material: 292 neonates admitted with diagnosis of neonatal septicaemia were included in the study. Diagnostic work up included complete hemogram with peripheral blood smear, CRP, blood culture and sensitivity (C/S) and other relevant investigations according to cases. Statistical analysis: Obtained data was analysed and presented. 95 % confidence interval values were also calculated. Results: Out of 292 cases of neonatal septicaemia blood culture was positive in 107(36.64%). Culture positivity in EOS & LOS were 66(34.74%) & 41(40.20%) respectively. In EOS gram negative organisms (83.33%) were common isolates while in LOS gram positive organisms (46.34%) were predominant. Gram positive were sensitive to vancomycin, linezolid while gram negative were sensitive to imipenam, amikacin, piperacillin + tazobactum. Conclusion: Neonatal septicemia is an important cause of morbidity and mortality. This is due to infection by both Gram positive and gram negative bacteria most of which are multi drug resistant especially in the hospital environment. Acinetobacter spp is one of the emerging causes of neonatal sepsis.
Keywords: Neonatal septicaemia, Early onset septicaemia (EOS), Late onset septicaemia (LOS), Antibiotic sensitivity
Full Text:
INTRODUCTION
The term neonatal sepsis used broadly in clinical context encompasses the diagnosis of septicaemia, meningitis, pneumonia, arthritis, osteomyelitis and urinary tract infection in newborn. This excludes local infection of newborn such as omphalitis, pyoderma and conjunctivitis. Prompt recognition, appropriate antimicrobial therapy and judicious supportive care are the key determinants of positive outcome in this serious paediatric emergency1 . It is estimated that almost 20% of all neonates develop infection and approximately 1% die of serious systemic infection. Not surprisingly, sepsis is the commonest admitting diagnosis among neonates at referral facilities1 . The detection of microorganisms in patient’s blood has a great diagnostic and prognostic significance. Many infections in the neonatal and paediatric age group can only be established on the basis of etiologic agent recovered from blood. In the major 16 hospitals of our country, the incidence of neonatal sepsis was 38 per 1000 live births as per the report of National Neonatal Perinatal database2 . This is in contrast with the reported incidence of 1 to 10 per1000 live births in developed countries1 . Over the last few decades, various studies have been conducted to find out causative organisms & their sensitivity patterns in neonatal septicaemia. The results obtained vary from place to place & from period to period in which the studies were conducted 3,4,5. Hence it is important to study neonatal septicaemia in different hospital settings and geographical areas to pin point the microbial aetiology and determine the antimicrobial susceptibility of the microbial isolates for effective management of the cases. It also helps to develop rational antibiotic policy for the NICU. So the present study was undertaken to know the clinicoetiological profile and antibiotic sensitivity pattern of neonatal septicaemia.
MATERIAL & METHODS
This prospective observational study was carried out in the neonatal unit of tertiary care teaching hospital in central India during the period of August 2011 to September 2013 after acceptance from institutional ethical committee. Aims of the study were to study the microbial profile of neonatal septicemia at our institute & to study the antimicrobial resistance & sensitivity pattern of bacterial isolates. Both outborn as well as inborn neonates admitted with diagnosis of neonatal septicemia were included in study after informed written parental consent. As per the criteria by Vergnonoet al5 all the neonates were included in the study. Septicemia was classified into Early onset septicemia (EOS) and late onset septicemia (LOS) as per standard guidelines6 . Diagnostic workup included complete hemogram with peripheral blood smear, CRP, blood culture and sensitivity (C/S). Chest X-ray, Urine C/S, cerebrospinal fluid (CSF) analysis and fungal C/S were done wherever necessary. All specimens were collected before starting antibiotics.
RESULTS
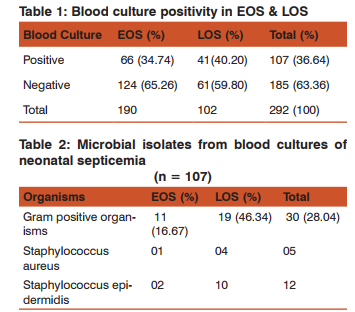
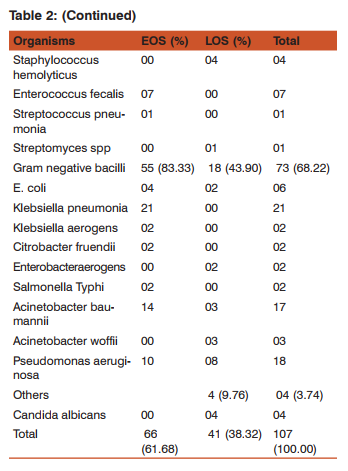
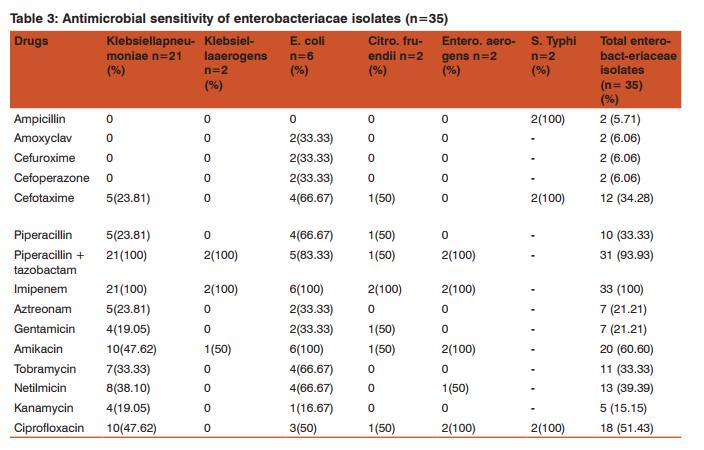
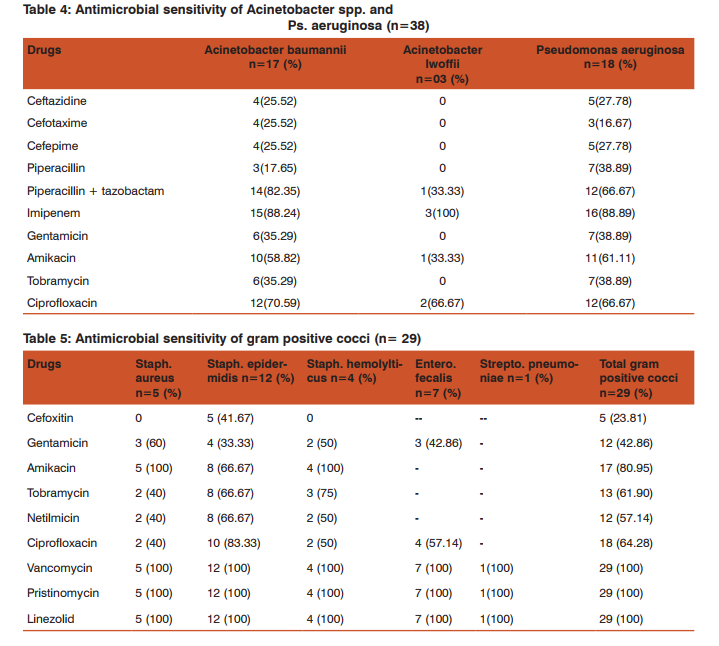
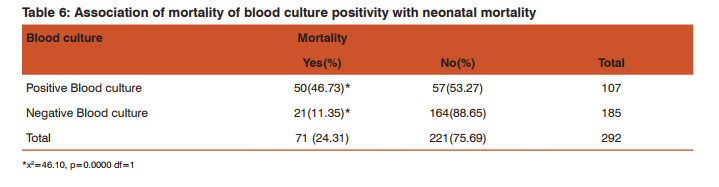
Over the study period, 292 neonates with neonatal septicemia were included in the study. Amongst them, EOS was seen in 190 (65.07%) cases and LOS in 102 (34.93%) cases. Of the total 292 neonatal septicemia cases, 182 (62.33%) were male and 110 (37.67%) were female. Of the total 292 cases, 58.91% were delivered in hospital, 14.38% were delivered at home, Lower segment caesarean section (LSCS) was performed in 21.92% cases and instrumentation was done in 4.79% cases. In the present study, 49 (16.78%) cases have history of maternal fever and mother of 60 (20.55%) cases showed premature rupture of membrane.In present study, most common risk factor observed in neonates in neonatal septicemia was low birth weight (69.18%), followed by prematurity (28.08%). Neonatal resuscitation, lack of breast feeding, superficial skin infection including umbilical sepsis and meconium aspiration were observed in 25.34%, 13.70%, 13.01% and 5.48% neonates respectively. In the present study, most common manifestation observed in neonatal septicemia cases were lethargy (72.60%) and poor sucking (72.60%) while least common were bulging fontanel (8.90%) and convulsions (9.93%). Other manifestations were decreases capillary refill time (21.92%), hypothermia (42.12%) and tachypnea (23.97%). Table 1 shows blood culture positivity in EOS and LOS cases. Amongst total 292 cases of neonatal septicaemia, in 107 (36.64%) cases blood culture was positive, whereas in 185 (63.36%) cases blood culture was negative. Of the total 292 cases of neonatal septicemia, early onset septicemia cases were 190 and late onset septicemia cases were 102. Of the 190 early onset neonatal septicemia cases, blood culture was positive in 66 (34.74%) cases. Similarly, out of 102 late onset neonatal septicemia cases, blood culture was positive in 41 (40.20%) cases. Table 2 shows the microbial isolates from blood culture of neonatal septicemia cases. Table 2 shows that, in the present study, gram negative bacilli were found to be commonest cause of neonatal septicemia (68.22%). Gram positive organisms were found in 28.04% cases. Klebsiella pneumoniae (19.62%), Pseudomonas aeruginosa (16.82%) and Acinetobacter baumannii(15.89%) were the commonest isolates from neonatal septicemia cases. In blood culture positive early onset neonatal septicemia cases (66), gram negative bacilli (83.33%) were common aetiological agents as compared to gram positive cocci (16.67%). Among gram negative bacilli, Klebsiella pneumoniae(31.82%), Acinetobacter baumannii(21.21 %) and Pseudomonas aeruginosa (15.15%) were the common isolates. Among gram positive organisms Enterococcus fecalis(10.61%) was the commonest organism. In blood culture positive late onset neonatal septicemia cases (41), both gram negative bacilli (43.90 %) and gram positive cocci (43.90 %) were isolated in equal number of cases while Candida albicans and Streptomyces spp were isolated in 4 (9.76%) and 1 (2.44%) cases each. S.epidermidis (24.39%) followed by P. aeruginosa (19.51%) formed the common bacterial isolates in LOS. Table 3 shows the antimicrobial sensitivity of enterobacteriaceae isolates from blood culture of neonatal septice-mia cases. It shows that all the enterobacteriaceae isolates (except S. Typhi, where imipenem sensitivity is not advised) are sensitive to imipenem. Except S. Typhi all the isolates were resistant to ampicillin. As many as 93.93% isolates of enterobacteriaceae were sensitive to piperacillin + tazobactam while only 33.33% were sensitive to piperacillin. Among aminoglycosides enterobacteriaceae isolate showed maximum sensitivity to amikacin (60.60%) fallowed by netilmicin (39.39%). All the isolates of Klebsiella pneumonia and Klebsiella aerogens were sensitive to piperacillin + tazobactam and imipenem. Klebsiella isolates in our study showed complete resistance to ampicillin, amoxyclav, 1st and 2nd generation cephalosporins. Among aminoglycosides amikacin showed maximum sensitivity to Klebsiella pneumoniae(47.62%) and Klebsiella aerogens(50%). Among the six isolates of E. coli complete sensitivity was seen with imipenem and amikacin. All the six isolates were resistance to ampicillin. Two isolates each of Citrobacter fruendii and Enterobacter aerogens showed complete resistance to ampicillin, amoxyclav, 1st and 2nd generation cephalosporins, kanamycin and aztreonam. In the present study, two strains of S. Typhi were isolated. Both were sensitive to ampicillin, cefotaxime & ciprofloxacin. Antimicrobial sensitivity of Acinetobacter spp. and Pseudomonas aeruginosa is shown in table 4. It shows that maximum isolates of Acinetobacter baumannii(88.24%), Acinetobacter woffii(100%), and Pseudomonas aeruginosa(88.89%) were sensitive to imipenem. As many as 82.35% strains of Acinetobacter baumannii were sensitive to Piperacillin + tazobactam while 70.59% to ciprofloxacin. Only 25.52% strains were sensitive to ceftazidime, cefotaxime and cefepime. None of the isolate of Acinetobacterl woffii showed sensitivity to ceftazidime, cefotaxime, cefepime, piperacillin, gentamicin and tobramycin. Pseudomonas aeruginosa isolate showed good sensitivity to Piperacillin + tazobactam (66.67%), Ciprofloxacin (66.67%) and Amikacin (61.11%). These isolates showed poor sensitivity to ceftazidime (27.78%), cefotaxime (16.67%) and cefepime (27.78%). Table 5 shows the antimicrobial sensitivity of gram positive cocci isolates from blood culture of neonatal septicemia cases. It shows that gram positive cocci isolates were 100% sensitive to linezolid, vancomycin and pristinomycin. Methicillin resistance was 100% in Staph.aureus and Staph. Hemolyticus while it was 58.33% in Staph. epidermidis. Among the aminoglycosides amikacin showed a maximum sensitivity in Staph. aureus (100%) and Staph. hemolyticus (100%). As many as 8 strains (66.67%) of Staph. Epidermidis were sensitive to amikacin, tobramycin and netilmicin. Table 6 shows mortality of neonate as per positivity of blood culture. Table 6 shows that mortality of neonates in blood culture positive cases was more (46.73%) than the culture negative cases (11.35%). It was found to be statistically significant (p= 0.0000).
DISCUSSION
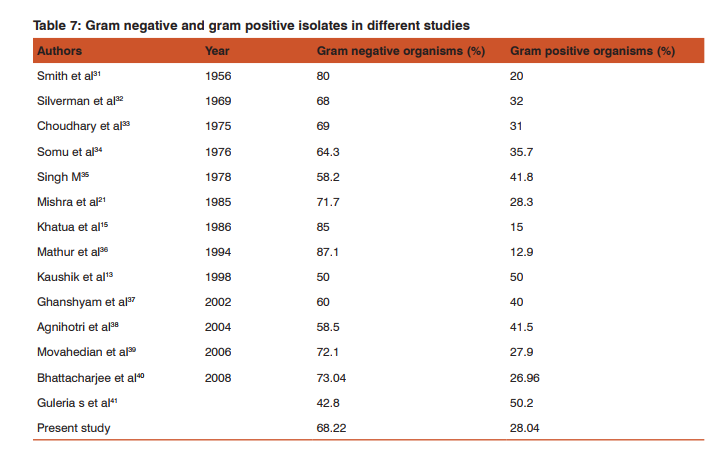
Neonatal septicemia remains a challenging and important problem even with modern drug therapy. It is associated with considerable morbidity and mortality. It is difficult to diagnose the neonatal infection, because of its non-specific clinical signs and symptoms. Microorganism detection has its value as a strong diagnostic method for neonatal septicemia. For the effective management of neonatal septicemia cases, study of bacteriological profile with their antibiotic sensitivity pattern plays a significant role7 . In present study, maternal pyrexia was seen in 16.78% cases. A similar finding was seen by Soman et al8 (18.6%) and Saxena et al9 (17.34%). In the present study, 20.55% of cases had history of premature rupture of membranes for more than 24 hours. A similar finding was seen in Roy et al10 (28.9%), Hossain et al11 (29.2%) & Kuruvilla et al12 (12.8%). Most important neonatal factor predisposing to infection is prematurity. Preterm infants have a 3-10 fold higher incidence of infection than full term normal weight infants.LBW is a well accepted risk factor for neonatal septicaemia13,14.Khatua et al15 and Mondal et al16 stated that LBW infants have low IgG and they are more susceptible to infections. There is little correlation between clinical manifestations and etiological agents4,17,18,19 . Lethargy (72.6%) was most common manifestation in present study similar to Guha et al20 (66.25%), Mishra et al21 (62.52%) & Gupta et al22 (66.7%). Ahmed et al23 (40%) & Buetow et al24 (31.01%) found lethargy in less number of cases. Poor feeding (71.925) was second most common manifestation in present study, a finding similar to Guha et al20 (66.25%), Mishra et al21 (62.52%). Buetow et al25 (19.62%) found that poor feeding was less common. In the present study, blood culture positivity in neonatal septicemia cases was 107 (36.64%), whereas in 185 (63.36%) of cases there was no growth. Culture positivity for aerobic organisms in neonatal sepsis varies widely (19.20% to 76.8%) among different studies7,26,27,28 . These wide variations might be due to the fact that most of the patients receive the antibiotics before they come to the tertiary care hospital. Further, self medication is very common as the medicines are easily available at the counter29. It can also be explained by technique & volume of blood sample collection, methods used for bacterial isolation or presence of anaerobic infection. The negative cultures were presumed to be due to anaerobic infections or antibiotic usage before collection of samples for culture or clinically overdiagnosing the bacterimias as a prelude to avoid the risk of missing any true bacterimias7 . In the present study, the percentage of gram negative septicemia is 68.22% and that of gram positive is 28.04% (Table 1). Observation made by various workers is given in Table 7. The increased susceptibility of neonates to the gram negative bacteria may be explained by the fact that the antibodies against these organisms are primarily IgM type, which do not transfer passively through placenta and are at very low level in blood (about 5% of adult value) at birth, and reaches the adult level by 2 years of age. This is in contrast with IgG type, which are passively transferred to placenta and are almost at adult level at birth and falls gradually reaching lowest level around 3 to 4 months of age after which they start to rise again gradually. Adequate IgG (except IgG 2-subtype) levels at term, afford protection against several gram positive bacteria30. In the present study (Table 1), it was observed that gram negative organisms causing EOS (83.33%) outnumbered gram positive organisms (16.67%). In contrast in LOS gram positive organisms isolates (46.34%) were more common than gram negative organisms (43.90%). The bacteriological profile differs in EOS and LOS and it also differs in developing and developed countries. In developed countries gram positive organism is predominant in both EOS and LOS but Group B streptococci is found more in EOS. In developing countries gram negative organism are predominant in EOS & LOS both.23 Kaushik et al13 had reported that gram negative bacilli predominated in EOS (62.5%) whereas gram positive organisms accounted for majority of LOS cases (58.33%). Chugh et al3 reported 90.31% gram negative bacilli in EOS and 29% positive organisms in LOS. Stoll et al14 stated that majority of EOS 60.7% were caused by gram negative organisms. Antimicrobial sensitivity showed that all the enterobacteriaceae isolates (except S. Typhi) were sensitive to imipenem. Except S. Typhi all the isolates were resistant to ampicillin. As many as 93.93% isolates of enterobacteriaceae were sensitive to piperacillin + tazobactam while only 33.33% were sensitive to piperacillin. Among aminoglycosides enterobacteriaceae isolate showed maximum sensitivity to amikacin (60.60%) followed by netilmicin (39.39%). Twenty three Klebsiella isolates and two isolates each of Citrobacter fruendii and Enterobacteraerogens showed complete resistance to ampicillin, amoxyclav, 1st and 2nd generation cephalosporins, cephamycin and tetracycline. Two strains of S. Typhi were sensitive to ampicillin, cefotaxime, ciprofloxacin and chloramphenicol. There were 21 isolates of Staphylococcus spp., with 5 S. aureus, 12 S. epidermidis and 4 S. hemolyticus. All the 21 Staphylococcus isolates showed 100% sensitivity for vancomycin, linezolid and pristinomycin. For S. aureus and S. hemolyticus maximum resistance (100%) was seen in penicillin G, cefoxitin and erythromycin. All the 7 strains of Enterococcus fecalis were sensitive to vancomycin, linezolid, pristinomycin whereas all were resistant to penicillin G and erythromycin. One isolate of Streptococcus pneumoniae was found to be 100% sensitive to all the drugs (penicillin G, erythromycin, vancomycin, pristinomycin, linezolid, chloramphenicol and tetracycline) tested. In our study, overall mortality rate was 24.31%. Further the mortality in blood culture positive cases of neonatal septicemia was higher (46.73%) as compared to culture negative cases (11.35%) and this difference was statistically significant (p value=0.0000 df=1 ).
CONCLUSIONS
Overall Gram negative bacilli were found to be commonest cause of neonatal septicemia. In EOS gram negative while in LOS gram positive organisms predominate. In EOS, Klebsiella pneumoniae, Pseudomonas aeruginosa and Acinetobacter baumannii whereas in LOS Staphylococcus epidermidis and Pseudomonas aeruginosa were found to be common. Acinetobacter spp is one of the emerging cause of neonatal septicaemia because of the high potential of this genus to develop antibiotic resistance, leading to a considerable selective advantage in environments with widespread and heavy use of antibiotic, especially with relation to hospital environment and nosocomial infections. This was evident in the present study with substantial isolation of this organism in cases of neonatal sepsis. The most effective antibiotic for gram negative isolates was imipenem, while the most effective antibiotic for gram positive isolates was vancomycin. Reserve drugs like linezolid and pristinomycin have not yet developed resistance42. Most of the organisms had good sensitivity to amikacin and ciprofloxacin. It is therefore necessary to generate hospital data on antimicrobial sensitivity of common isolates, provide timely sensitivity report and advise them regarding judicious use of antibiotics.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Paul VK and Singh MB. Neonatal sepsis. In: Meharban Singh, editor. Medical emergencies in children. 3rd ed. New Delhi: Sagar publications; 2000. p.117-35.
2. Aggarwal R, Sarkar N, Deokari AK and Paul VK. Sepsis in the newborn. Indian J Pediatr 2001; 68: 1143-7.
3. Chugh K, Aggarwal BB, Kaul VK and Arya SC. Bacteriological profile of neonatal septicaemia. Indian J Pediatr 1988; 55: 961-5.
4. Gotoff SP, Behrman RE. Neonatal septicemia. J Pediatr 1970; 76: 142-53.
5. Vergnono S, Sharland M, Kazembe P,Mwansambo and Heath PT. Neonatal sepsis: An international perspective. Arch Dis Child Fetal Neonatal Ed 2005; 90: 220-4
. 6. Stoll BJ. Infection of neonatal infant. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds. Nelson Textbook of Pediatrics: The Fetus and the Neonatal Infant. 18th ed. vol. 1. Philadelphia: WB Saunders Company; 2007:798e809.
7. Murty DS & Gyaneshwari M. Blood cultures in paediatric patients: A study of clinical impact. Indian J Med Microbiol 2007; 25; 220-4.
8. Soman M, Green B and Daling J. Risk factors for early neonatal sepsis. Am J Epidemiol 1985; 121: 712-9.
9. Saxena S, Anand NK, Saini L and Mittal SK. Bacterial infections among home delivered neonates: Clinical picture and bacteriological profile. Indian Pediatr 1980; 17:17-24.
10. Roy I, Jain A, Kumar M and Agrawal SK. Bacteriology of neonatal septicemia in a tertiary care hospital of Northen India. Indian J Med Microbiol 2002; 20: 156-9.
11. Hossain MM, Afroza S, Shirin M, Chowdhury NA, Saha SK. Bacterial aetiology of neonatal sepsis in a tertiary care hospital in Bangladesh. Bang J Child Health 2004; 28: 81-5.
12. Kuruvilla KA, Pillai S, Jesudason M and Jana AK. Bacterial profile of sepsis in a neonatal unit in south India. Indian Pediatrics 1998; 35: 851-8.
13. Kaushik SL, Parmar VR, Grover N, Grover PS and Kaushik R. Neonatal sepsis in Hospital born babies. J Commun Dis 1998; 30: 147-52.
14. Stoll B J, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, Lemons JA, Donovan EF, Stark AR, Tyson JE. Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network.Pediatrics 2002; 110: 285–91.
15. Khatua SP, Das AK, Chattergee BD, Khatua S, Ghose B et al. Neonatal septicaemia. Indian J Pediatr 1986; 53: 509-14.
16. Mondal GP, Raghvan M, Bhat BV and Srinivasan S. Neonatal septicaemia among inborn and outborn babies in a referral hospital, Indian J of Pediatr 1991; 58: 529-33.
17. Bhakoo ON, Agarwal KC, Narang A, Bhattacharya S. Prognosis and treatment of neonatal septicemia a clinicopathological study of 100 cases. Indian Paediatr 1974; 11: 519.
18. Tak SK, Bhandari PC. Value of buffy coat examination in early diagnosis of neonatal septicemia. Indian Pediatr 1980; 17: 399.
19. Bhakoo ON, Agarwal KC, Mohini Mahajan C, Walia BNS. Septicemia in infant and children- a bacteriological study. Indian Paediatr 1968; 5: 518.
20. Guha DK, Jaspal D, Das K, Khatri RL, and Srikumar R. Outcome of neonatal septicemia- A clinical and bacteriological profile. Indian Pediatr 1978; 15: 423-7.
21. Mishra JN, Rai MK, Chakraborty S, Prasad S. Study of neonatal septicemia. Indian pediatr 1985; 22: 281-5.
22. Gupta P, Murali MV, Faridi MMA, Kaul PB, Ramachandran VG. Clinical profile of Klebsiella septicemia in neonates. Indian J Pediatr 1993; 60: 565-72.
23. Ahmed ASMNU, Chowdhury MAKA, Hoque M, Damstadt GL. Clinical & Bacteriological profile of neonatal septicemia in tertiary level pediatric hospital in Bangladesh. Indian Pediatr 2002; 39: 1034-9.
24. Erikson M. Neonatal Septicemia. Acta Paeditr Scand 1983; 72: 1-8.
25. Buetow YC, Klein SW, Lane RB. Septicemia in premature infants- The characteristics, treatment and prevention of septicemia in premature infants. Am J Dis Child 1965; 110: 29-41.
26. Dunham EC. Septicemia in the newborn. Am J Dis Child 1933; 45: 229-53.
27. Todd. Septicemia of the newborn- A clinical study of 15 cases. Arch Dis Child 1946; 23: 102.
28. Ananthakrishnan S, Gunasekaran D. Etiology and risk factors for early onset neonatal sepsis. IJMM 2009; 27: 279.
29. Arora U and Devi P. Bacterial profile of blood stream infections and antibiotic resistance pattern of isolates. JK Sci 2007; 9: 185-90.
30. Singh MB. Perinatal infections. In: Care of the newborn. 6th ed. New Delhi: Sagar publications; 2004. p.196-216.
31. Smith and Jenison. Perinatal infections and perinatal death. Lancet 1956; 2: 903.
32. Silverman and Homan. Sepsis of obscuse origin in newborn. Pediatr 1969; 3: 157.
33. Choudhary P, Srivastva G, Agrawal DS, Saini L and Gupta S. Bacteriological study of neonatal infections. Indian Pediatr 1975; 11: 519-28.
34. Somu N, Shetty VS, Moses IG, Raju VB. A critical analysis of septicemia in infancy. Indian Pediatr 1976; 13(6): 443-6.
35. Singh M. Nosocomial bacterial infection among newborn babies. Indian J Pediatr 1978; 45: 313-7.
36. Mathur M, Shah H, Dixit K, Khambadkone S, Chakrapani A. Bacteriological profile of neonatal septicemia cases (for the year 1990-91). J Postgrad Med 1994; 40: 18-20.
37. Ghanshyam DK, Ramachandran VG, and Gupta P. Bacteriological analysis of blood culture isolates from neonates in a tertiary care hospital in India. J Health Popul Nutr 2002; 20(4): 343-7.
38. Agnihotri N, Kaistha N and Gupta V. Antimicrobial susceptibility of isolates from neonatal septicemia. J Infect Dis 2004; 57: 273-5.
39. Movahedian AH, Moniri R and Mosayebi Z. Bacterial culture of Neonatal Sepsis. Iranian J Publ Health 2006; 33: 84-9.
40. Bhattacharjee A, Anupurba S, Gaur A and Sen MR. Prevalence of inducible amp C β-lactamase- producing Pseudomonas aeruginosa in a tertiary care hospital in Northen India. IJMM 2008; 26: 89-98.
41. Guleria S, Kaushal R, Sharma J. Neonatal septicemia Emergence of coagulase negative Staphylococcus as major etiological agent. pediatric infectious disease 2013, http:// dx.doi.org/10.1016/j.pid.2013.10.003 In Press
42. Khaleel M, Wajid M, A Study on Neonatal Septicemia in Blood Culture Isolates and their Antimicrobial Susceptibility Pattern in View of Emerging Drug Resistance. http:// ijhsonline.com 2014; vol 1, issue 3: 52-57.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





