IJCRR - 7(6), March, 2015
Pages: 47-50
Print Article
Download XML Download PDF
FINE NEEDLE ASPIRATION CYTOLOGY OF DE QUERVAIN'S THYROIDITIS - A RARE CASE REPORT
Author: R. Vimal Chander, Sonti Sulochana, S. Chitra
Category: Healthcare
Abstract:Introduction: De Quervain's thyroiditis, also called subacute thyroiditis, accounts for 5 % of the thyroid disorders, clinically characterised by painful diffuse enlargement of the thyroid, and is usually self-remitting. Case Report: We report a case of a 28 year old male presenting with painful enlargement of right lobe of thyroid gland with a diagnosis of De Quervain's thyroiditis on fine needle aspiration cytology. Discussion: This is to illustrate that De Quervain's thyroiditis has to be considered in the differential diagnosis of painful asymmetrical enlargement of thyroid, especially when there are numerous epithelioid granulomas with multinucleated giant cells along with the absence of antithyroid antibodies and rapid response to steroid therapy.
Keywords: Thyroiditis, Subacute thyroiditis, De Quervain’s, Granulomatous thyroiditis
Full Text:
INTRODUCTION
Subacute thyroiditis is a rare self-remitting inflammatory disease of the thyroid, usually caused by viral infection. [1] It accounts for 5 % of the thyroid disorders. On examination, the thyroid is diffusely enlarged and tender. The diagnosis in most cases is self evident based on history, clinical examination, laboratory findings and clinical course of the disease. Rarely, it may present as a nodule or single lobe enlargement. Here we report a case of De Quervain’s thyroiditis in a 28 year old male presenting with enlarged right lobe of the thyroid.
CASE REPORT
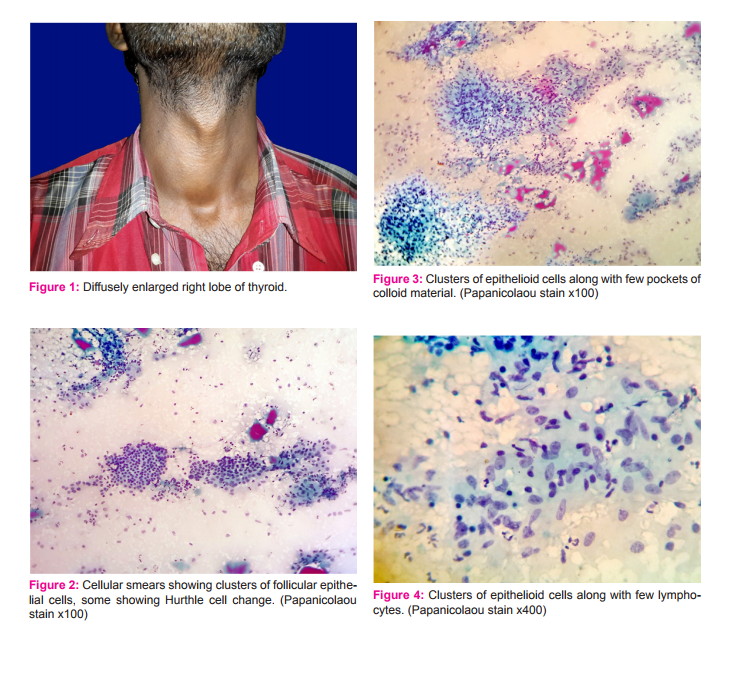
A 28 year old male presented with progressively enlarging swelling in front of the neck for the past 2 years associated with pain. He gave history of fever with sore throat prior to the onset of the swelling. He is not a known diabetic, tuberculosis or other co-morbid conditions. On examination, right lobe of the thyroid was diffusely enlarged and mildly tender. [Figure 1] Cervical lymph nodes were not palpable. Thyroid function tests revealed elevated free Triiodothyronine (free T3) levels (9.2 pg/ml, Normal range: 2.3- 4.2 pg/ml) and free thyroxine (free T4) levels (3.41 ng/l, Normal range: 0.8-1.8 ng/l) and markedly reduced Thyroid stimulating hormone (TSH) levels (0.02 mIU/l, Normal range: 0.3-3.04 mIU/l). Antithyroglobulin antibodies were found to be negative. Ultrasonogram of the neck showed normal left lobe of thyroid and enlarged right lobe with multiple hypoechoic nodules with increased surrounding vascularity. Fine needle aspiration cytology of thyroid was then done. Cytology showed cellular smears with clusters of follicular epithelial cells, some of the cells showing Hurthle cell change, along with numerous clusters of epithelioid histiocytes, macrophages, few lymphocytes and focal areas of neutrophilic debris in the background. [Figures 2 to 6] An impression of De Quervain’s thyroiditis was then made. He was then treated with prednisone 40 mg/day for 10 days and gradually tapered over the next 8 weeks. On follow up, the patient reported resolution of pain and reduction in the size of the swelling. Follow up thyroid function tests after 3 months were found to be within normal limits.
DISCUSSION
De Quervain’s thyroiditis, also called as granulomatous thyroiditis or giant cell thyroiditis, is a rare form of thyroiditis which is spontaneously remitting and considered to be of viral etiology.[1] It presents typically in adults following an upper respiratory tract infection with fever and followed by diffuse and painful enlargement of thyroid.[2] Disruption of thyroid follicles due to inflammation initially releases the preformed thyroid hormones into the circulation producing a transient phase of hyperthyroidism, during which period the thyroid hormones T3 and T4 levels are increased and thyroid stimulating hormone (TSH) values are decreased. Thyroid function returns to normal by 6 to 8 weeks and may be followed by hypothyroidism, which is usually transient.[3] High titres of anti-thyroglobulin and anti-microsomal antibodies, which are so characteristic of Hashimoto thyroiditis, are not seen in De Quervain’s thyroiditis. In a few cases, thyroid may be asymmetrically enlarged which may raise the suspicion of neoplasia and hence may be referred for fine needle aspiration cytology.[4],[5] Cytological features include numerous clusters of epithelioid histiocytes along with multinucleated giant cells along with lymphocytes and degenerating follicular epithelial cells, some may show Hurthle cell change, in a dirty background containing cell debris and colloid. Multinucleated giant cells are numerous and is a more striking finding. Scant unremarkable macrofollicle fragments and colloid are usually present.[6] Granulomas may also be seen in the thyroid as a histiocytic response to hemorrhage, usually as a reaction to spilled colloid adjacent to a neoplasm following aggressive clinical examination (palpation thyroiditis). It can also be seen in fungal infections, sarcoidosis, some types of vasculitis or rarely as a foreign body giant cell reaction.[7],[8] Multinucleated giant cells are also seen in autoimmune thyroiditis, which can be confirmed by increased titres of anti-microsomal and anti-thyroglobulin antibodies.[9] Aspiration of intact follicles (pseudo-giant cells) should not be mistaken for multinucleated giant cells. Multinucleated giant cells along with epithelioid cells and lymphocytes, seen in tuberculosis, a rare infection affecting the thyroid gland, should also be kept in mind as a differential diagnosis in such situations. Tuberculosis of thyroid may present as multiple caseating granulomas, cold abscess with multiple sinuses or as a chronic fibrosing type. Especially, the chronic fibrosing tuberculous lesion of the thyroid may be difficult to distinguish from De Quervain’s thyroiditis. In such cases, demonstration of acid fast bacilli by Zeihl-Neelsen staining would be more useful for confirmation of diagnosis, though it may be often negative in tissue sections. This along with any other clinical manifestations of tuberculosis would be helpful for confirmation.[10] The dirty background may be mistaken for necrosis and this along with degenerative atypia in the follicular epithelial cells may lead to an inappropriate suspicion of malignancy. Rarely, the pale elongated or folded nuclei of the epithelioid histiocytes may be potentially misinterpreted as papillary carcinoma nuclei.[11] Anaplastic carcinoma of thyroid may rarely contain osteoclast-like giant cells as a reactive population, which may cause a diagnostic confusion with a granulomatous process, but it can usually be ruled out owing to the absence of significant nuclear atypia in De Quervain’s thyroiditis.[12]
CONCLUSION
De Quervains thyroiditis is a rare form of inflammation of the thyroid and the differential diagnosis to be considered ranges from various nonneoplastic to neoplastic lesions. This case illustrates that De Quervain’s thyroiditis has to be considered in the differential diagnosis of painful asymmetrical enlargement of thyroid, especially when there are numerous epithelioid granulomas with multinucleated giant cells along with the absence of antithyroid antibodies and rapid response to steroid therapy.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.

References:
1. Sweeney LB, Stewart C, Gaitonde DY. Thyroiditis: an integrated approach. Am Fam Physician. 2014;90(6):389-96.
2. Benbassat CA, Olchovsky D, Tsvetov G, Shimon I. Subacute thyroiditis: clinical characteristics and treatment outcome in fifty-six consecutive patients diagnosed between 1999 and 2005. J Endocrinol Invest. 2007;30(8):631-635.
3. Alfadda AA, Sallam RM, Elawad GE, Aldhukair H, Alyahya MM. Subacute thyroiditis: clinical presentation and long term outcome. Int J Endocrinol. 2014;2014:794943. doi: 10.1155/2014/794943.
4. Fatourechi V, Aniszewski JP, Fatourechi GZ, Atkinson EJ, Jacobsen SJ. Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, study. J Clin Endocrinol Metab. 2003;88(5):2100- 2105.
5. Shabb NS, Salti I. Subacute thyroiditis: fine-needle aspiration cytology of 14 cases presenting with thyroid nodules. Diagn Cytopathol. 2006;34(1):18-23
.6. Shabb NS, Salti I. Subacute thyroiditis: Fine needle aspiration cytology of 14 cases presenting with thyroid nodules. Diagn Cytopathol 2006;34:18-36.
7. Alvi MM, Meyer DS, Hardin NJ, Dekay JG, Marney AM, Gilbert MP. Aspergillus thyroiditis: a complication of respiratory tract infection in an immunocompromised patient. Case Rep Endocrinol. 2013;2013:741041. doi: 10.1155/2013/741041.
8. Wilson RA, Gartner WS Jr. Teflon granuloma mimicking a thyroid tumor. Diagn Cytopathol 1987;3:156-8. 9. Shabb NS, Tawil A, Gergeos F, Saleh M, Azar S. Multinucleated giant cells in fine-needle a
spiration of thyroid nodules: their diagnostic significance. Diagn Cytopathol. 1999;21(5):307-312.
10. Kataria SP, Tanwar P, Singh S, Kumar S. Primary tuberculosis of the thyroid gland: a case report. Asian Pac J Trop Biomed. 2012 Oct;2(10):839-40.
11. Azer P, Zhai J, Yu R. Atypical de Quervain’s thyroiditis masquerading as papillary thyroid cancer. Endocrinol Nutr. 2013 Mar;60(3):158-9.
12. B, MacFarlane J, Chan N. Osteoclastoma-like anaplastic carcinoma of the thyroid: diagnosis by fine needle aspiration cytology. Acta Cytol 1990; 34:248-50.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





