IJCRR - 7(7), April, 2015
Pages: 35-39
Print Article
Download XML Download PDF
FUNCTIONAL AND RADIOLOGICAL OUTCOME OF UNCEMENTED BIPOLAR ARTHROPLASTY
IN UNSTABLE INTERTROCHANTERIC FRACTURES OF THE ELDERLY
Author: Jalaluddeen Mahin Vaidyar, Sandeep Shibli, U. Hashir Safwan, Shabir Kassim
Category: Healthcare
Abstract:Background: Bipolar hemiarthroplasty is an effective option for unstable intertrochanteric fractures in the elderly. This study evaluated the functional and radiological outcome following uncemented hemiarthroplasty in elderly unstable intertrochanteric fractures Methods: 25 hips were followed for a period of 1 year after hemiarthroplasty with a blast coated revision stem (Orthovasive). The mean age was 77 and mean follow up 16 months. The modified Merle D'Aubigne score was assessed for function and radiological results were assesses using a range of indices. Results: At the last follow up the mean Merle D'Aubigne score was 14.5. Twenty cases (80%) regained their preoperative walking ability postoperatively. Radiologically, there were 15 cases (60%) of bone in growth and 10 cases (40%) with stable fibrous fixation. Endosteal new bone formation was found in 10 (40%) patients. There were no cases with progressive subsidence or significant changes in alignment. Conclusions: The functional and radiological outcome after 1 year followup in unstable intertrochanteric fractures in elderly patients with uncemented bipolar arthroplasty was satisfactory.
Keywords: Elderly, Unstable intertrochanteric fracture, Uncemented bipolar arthoplasty
Full Text:
INTRODUCTION
Severely displaced and comminuted intertrochanteric fractures are common in elderly patients with osteoporosis. Traditionally, they have been treated by internal fixation which have often had complications of nonunion, implant failure and screw cutout.1,2 Bipolar arthroplasty being an alternative to internal fixation , allows for rapid rehabilitation of the elderly patient.3 Controversy regarding use of cement in arthroplasty is there. Cemented fixation has the advantage of giving immediate stability in aged patients.4 Cementless fixation has the distinct advantage of avoiding cardiovascular toxicity of cement which may be disastrous in the elderly.5 The present study aims to evaluate the functional and radiological outcome of uncemented bipolar hemiarthroplasty in patients over the age of 70 years with unstable intertrochanteric fractures.All patients were implanted with cylindrical corundum blasted proximal and isthmic fixing stems
METHODS
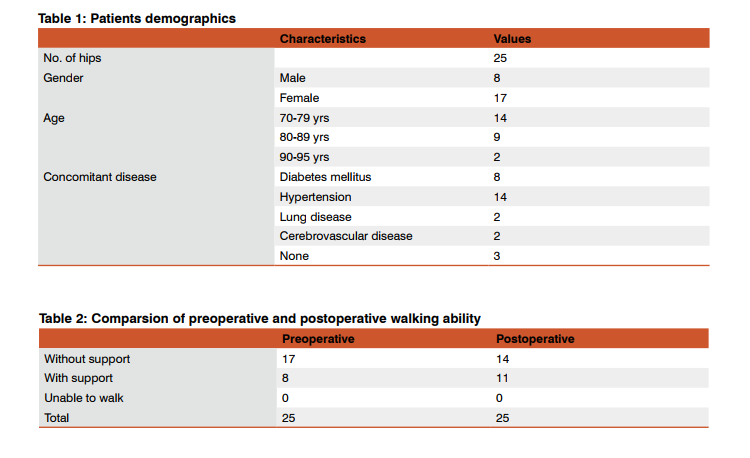
Uncemented bipolar arthroplasty using the corundum blasted revision stem (orthovasive, biorad medisys) and 22.2/28 mm femoral head with corresponding femoral cup ( INDUS) was performed on 25 patients with unstable intertrochanteric fractures in patients over the age of 70 who were walking with or without a walking aid at our institution between January 2010 and December 2014. All the above patients could be followed up for 1 year and were included in our study. All patients had AO type A2 or A3 fractures which are associated with high rates of internal fixation failure. The mean age of the patients was 77 (range, 70 to 90 years). There were 17 females (68% ) and 8 males (32%). The mean follow-up period was 16 months (range, 12 to 20 months). The mean time from fracture to surgery was 2 days. 18 patients (72%) had multiple morbidities. (Table 1)
Operative technique
Surgery was performed by the same team in all cases under spinal anaesthesia in all cases. An uncemented corundum blasted revision femoral stem (Orthovasive, Biorad medisys) was inserted through the posterolateral approach. A bipolar femoral cup(indus) and a corresponding 22.2 or 28 mm femoral head was used.Depending on whether the abductor mechanism was in continuity, trochanteric fragment was fixed by tension band wiring. Patient was made to sit up with legs dangling on the side and quadriceps muscle strengthening begun on day 1. All patients were started on partial weight bearing with quadrangular walker and full weight bearing within 4 days and 1 month respectively.
Functional outcome assessment
The modified Merle Dáubigne scores 6) at the last followup were classified into four categories; excellent, good, fair and poor.Preoperative and postoperative walking abilities were compared.
Radiological assessment
On the postoperative radiographs, proximal canal fit was deemed good if the stem filled the proximal canal more than 75% and distal fit was good if there was a gap less than 1 mm between the stem and inner cortex.7,8) The femoral stem stability was classified into fixation by bone ingrowth, stable fibrous fixation, and unstable prosthesis according to the criteria of Engh et al.9,10)The changes in the alignment and subsidence of the femoral components were measured from after surgery to the last follow-up; ≥ 3° of valgus or varus and ≥ 5 mm longitudinal change were considered significant.3 The radiolucent line, bone resorption, endosteal new bone formation and osteolysis were examined in the seven zones described by Gruen et al.11) A radiolucent line denoted the radiolucent area around the stem surrounded by radiodense lines, and was considered present if it occupied ≥ 50% of any zone.12)Loosening of the femoral stem was defined as the appearance of a radiolucent line progressive or > 1 mm in all zones, or the presence of continuous subsidence or migration of the femoral stem.
RESULTS
The mean Modified Merle D ‘aubigne score at the last follow up was 14.5. Six (24%)patients had an excellent score, 11(44%)patients had a good score, 6(24%) patients had a fair score and 2(8%)patients had a poor score. Of the 25 patients, 8 (32%) and 17 (68%)patients could walk with and without aid before surgery respectively. Of the 17 patients , 14 could still walk without support after surgery , but of these 3 needed a walking aid . Of the 8 patients who needed a walking aid before surgery, 6 patients used the same aid after surgery and 2 patients needed to use a quadrangular walker. None of the patients were unable to walk. Overall, 20 out of 25 patients regained their preoperative walking ability.(Table 2) All patients achieved either a proximal or isthmic fit or both. The proximal fit, the isthmic level press fit and both were seen in 7(28%), 11(44%) and 7 (28%) respectively. The stability of the femoral stem at the final follow up were classified according to the criteria of Engh et al. There was fixation by bone ingrowth in 15 patients(60%) and stable fibrous fixation in 10 patients(40%). There were no unstable prostheses. A radiolucent line was observed in 3 patients and mainly in Gruen zones 2 and 7; in zone 2 in 1 patient and in zone 7 in 2 patients. Endosteal new bone formation was observed in 10 patients, mainly in Gruen zones 4, 5 and 6 . Bone resorption was noted in 12 patients(48%) and mostly in Gruen zones 1 and 7. None of the cases showed a change in alignment of the implant more than 3 degrees, valgus or varus. The amount of femoral stem subsidence was 1 and 2 mm in 5 and 7 patients respectively. Deep infection occured as a postoperative complication in one patient which healed uneventfully by debridement and lavage . No heterotopic ossification was seen in any case. No intraoperative femoral fracture or death occured during surgery. There were no dislocations or embolic episodes . There was one death due to myocardial infarction at 8 months followup in a patient with previous cardiac illness.
DISCUSSION
Elderly patients with unstable intertrochanteric fractures have severe comminution and displacement. These fractures are less amenable to open reduction and fixation often leading to fixation failure or nonunion.2)The inability to mobilize early in the postoperative period often leads to postoperative complications and high mortality. Hemiarthroplasty is invariably the most effective primary treatment method for unstable intertrochanteric fractures with respect to early postoperative mobilization.3,4,13,14) In patients with poor bone quality , cemented implants have the distinct advantage of offering initial implant stability.13,15,16) The high death rate in arthroplasty patients undergoing cemented fixation 5) can be prevented by use of cementless implants.But implant migration due to lack of osteointegration, thigh pain and bone resorption as a result of increased stiffness can be a problem 17,18). But recent reports are encouraging in that , by promoting osteointegration of cementless implants , there has been no increase of implant failure rates , even in elderly patients with osteoporosis. 17)In our study, initial press fit fixation was achieved in all patients either at the proximal canal or isthmus, and fixation by osteointegration or fibrous fixation after a 1 year follow up was observed, even though minimal subsidence was observed in few patients. This indicates the high Osteointegration rates in the diaphysis of osteoporotic elderly patients with blast coated implants. There were no incidents of stem loosening,progression of subsidence or alignment changes. Bone resorption was mainly noted in gruen zones 1, 2 and 7, which did not produce any fracture or loosening.In elderly patients with multiple co morbidities , early ambulation within one week is essential for preventing complications . Early mobilisation is feasible only with initial press fit fixation. In a study comparing hemiarthroplasty and internal fixation, better results were seen in the hemirthroplasty group with respect to limping and use of walking aids in patients with limited walking ability before surgery. 14)The use of a cylindrical implant as in our study for isthmic or diaphyseal fixation is necessary in elderly patients with intertrochanteric fractures where proximal femorl fit is difficult to achieve. The orthovasive stem , owing to the cylindrical shape makes isthmic or diaphyseal fixation regardless of the Dorr type. 19). In our study , initial press fit at the isthmus was achieved in 60 % of patients in whom proximal fixation was not possible. The prevention of complications associated with bed rest such as Deep vein thrombosis and subsequent embolism , bed sores were achieved by the initial press fit fixation, the subsequent mobilisation and intensive quadriceps femoris muscle rehabilitation. The overall functional recovery was deemed satisfactory in view of all patients walking with or without aid at final followup excepting one patient who was bedridden with a cerebrovascular accident. Cemented fixation is associated with the highest mortality rate in arthroplasty patients 20) , which is a concern in elderly patients.In our study, uncemented fixation in unstable intertrochanteric fractures using a cylindrical implant resulted in satisfactory results due to avidance of cement related complications and early mobilisation due to achievement of initial on table press fit stability. CONCLUSION The short term results of uncemented bipolar hemiarthroplasty with a cylindrical stem in elderly patients with unstable intertrochanteric fractures yielded satisfactory results. Further studies with long term follow up should be done to determine long term functional outcome.
ACKNOWLEDGEMENTS
Authors acknowledge the immense help received from the scholars whose articles are cited and included in the references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
SOURCE OF FUNDING
Self –funded. Funded at the faculty level using the faculties’ own source of funds.
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest
ETHICAL CLEARANCE
Ethical clearance for this study has been obtained from the Highland Hospital Institutional and Ethics committee
References:
1. Haidukewych GJ, Israel TA, Berry DJ. Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am. 2001;83(5):643–650.
2. Kang SY, Lee EW, Kang KS, et al. Mode of fixation failures of dynamic hip screw with TSP in the treatment of unstable proximal femur fracture: biomechanical analysis and a report of 3 cases. J Korean Orthop Assoc. 2006;41(1):176– 180.
3. Hwang DS, Kwak SK, Woo SM. Results of cementless hemiarthroplasty for elderly patients with unstable intertrochanteric fractures. J Korean Hip Soc. 2004;16(3):386–391.
4. Rothman RH, Cohn JC. Cemented versus cementless total hip arthroplasty: a critical review. Clin Orthop Relat Res. 1990;(254):153–169.
5. Christie J, Burnett R, Potts HR, Pell AC. Echocardiography of transatrial embolism during cemented and uncemented hemiarthroplasty of the hip. J Bone Joint Surg Br. 1994;76(3):409–412.
6. Merle d’aubinge R, Postel M. Functional results of hip arthroplasty with acrylic prosthesis. J Bone Joint Surg [Am] 1954;36-A:451–75.
7. Kang JS, Moon KH, Park SR, Sun SH. Long-term results of total hip arthroplasty with an AML hip prosthesis. J Korean Hip Soc. 2004;16(1):17–23.
8. Kim YH, Kim VE. Cementless porous-coated anatomic medullary locking total hip prostheses. J Arthroplasty. 1994;9(3):243–252. [PubMed]
9. Engh CA, Bobyn JD, Glassman AH. Porous-coated hip replacement: the factors governing bone ingrowth, stress shielding, and clinical results. J Bone Joint Surg Br. 1987;69(1):45–55. [PubMed]
10. Engh CA, Massin P, Suthers KE. Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop Relat Res. 1990;(257):107–128. [PubMed]
11. Gruen TA, McNeice GM, Amstutz HC. “Modes of failure” of cemented stem-type femoral components: a radiographic analysis of loosening. Clin Orthop Relat Res. 1979;(141):17–27. [PubMed]
12. Kim YM, Kim HJ, Ahn JH, Kim KH, Kang SB. Early postoperative periprosthetic radiological findings in cementless THRA: comparison between porous-coated implant and hydroxyapatite-coated implant. J Korean Orthop Assoc. 1997;32(4):1005–1014.
13. Stern MB, Angerman A. Comminuted intertrochanteric fractures treated with a Leinbach prosthesis. Clin Orthop Relat Res. 1987;(218):75–80. [PubMed]
14. Moon CY, Ji JH, Park SE, Kim YY, Lee SW, Kim WY. Comparison of the clinical outcomes between internal fixation and primary hemiarthroplasty for treating unstable intertrochanteric fracture in the elderly. J Korean Hip Soc. 2008;20(4):273–277.
15. Green S, Moore T, Proano F. Bipolar prosthetic replacement for the management of unstable intertrochanteric hip fractures in the elderly. Clin Orthop Relat Res. 1987;(224):169– 177.
16. Haentjens P, Casteleyn PP, De Boeck H, Handelberg F, Opdecam P. Treatment of unstable intertrochanteric and subtrochanteric fractures in elderly patients: primary bipolar arthroplasty compared with internal fixation. J Bone Joint Surg Am. 1989;71(8):1214–1225.
17. Andress HJ, Kahl S, Kranz C, Gierer P, Schurmann M, Lob G. Clinical and finite element analysis of a modular femoral prosthesis consisting of a head and stem component in the treatment of pertrochanteric fractures. J Orthop Trauma. 2000;14(8):546–553. [PubMed]
18. Maloney WJ. Femoral fixation in older patients: uncemented is reasonable in many patients. 74th Annual Meeting of the American Academy of Orthopaedic Surgeons; 2007 Feb 14-18; San diego, CA, USA.
19. Dorr LD, Faugere MC, Mackel AM, Gruen TA, Bognar B, Malluche HH. Structural and cellular assessment of bone quality of proximal femur. Bone. 1993;14(3):231–242.
20. Parvizi J, Holiday AD, Ereth MH, Lewallen DG. The Frank Stinchfield Award: sudden death during primary hip arthroplasty. Clin Orthop Relat Res. 1999;(369):39–48.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





