IJCRR - 7(7), April, 2015
Pages: 32-34
Print Article
Download XML Download PDF
ISCHEMIC STROKE IN AN ATRIAL SEPTAL ANEURYSM INDIVIDUAL- A CASE REPORT
Author: Sahid Imam Mallick, Sauvik Dasgupta, Auriom Kar, Soumava Mukherjee, Sneha Jatan Bothra, Mansi Das, N. B. Debnath
Category: Healthcare
Abstract:An atrial septal aneurysm (ASA) is a well recognized but rare cardiac defect where there is localized saccular deformity of atrial septum that bulges in to either right or left atrium. It may be present isolated or in presence of other defects. ASA can be diagnosed by tranthoracic (TTE) or transesophageal (TEE) echocardiography. In most situations it is diagnosed incidentally and often consider as benign entity. However, atrial arrhythmias and arterial embolisms are the complications ASA may present with. Here we present a 40 years male patient presents with right middle cerebral artery ischemic stroke with left sided hemi paresis,
seizures and altered sensorium. All blood parameters and Doppler imaging showed normal study. Echocardiography revealed a moderate atrial septal aneurysm. Patient was treated with anti coagulation and discharged in stable condition.
Keywords: Atrial septal aneurysm (ASA), Ischemic stroke, Echocardiography
Full Text:
INTRODUCTION
Atrial septal aneurysm (ASA) is a congenital malformation of the septum primum layer of the interatrial septum but differences between interatrial pressure forces have also been reported as a cause of its development.1 Atrial septal aneurysm may be isolated or associated to another anomaly and their commonest association is patent foramen ovale (PFO). Other associations are atrial septal defect, mitral valve prolapsed, tricuspid valve prolapse, marfans syndrome, sinus of valsalva aneurysm and aortic dissection. The widespread availability of TTE and TEEhas identified ASA with increasing frequency.2 Although these abnormalities are considered clinically benign entities, they have been independently associated with ischemic stroke.3 According to Hanley’s diagnostic criteria, atrial septum is considered to be aneurysmal, when a dilated segment protrudes at least 15 mm beyond the level surface of the atrial septum.1
CASE REPORT
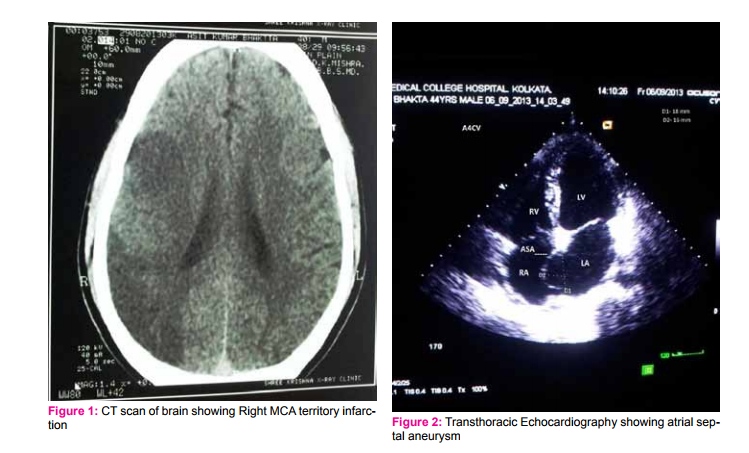
A 40 years male patient with no previous significant medical history presented with sudden onset history of seizures and left-sided hemi paresis followed by altered sensorium. On admission patient’s physical examination revealed right facial palsy, grade III-IV mid systolic mummur better heard at apex, left upper and lower limb grade II power with extensor planter response on left side, pulse was 78/minutes, regular and blood pressure was 116/70 mmHg. All peripheral pulses were palpable. Patient was drowsy at the time of admission, but arousable. Per abdomen and respiratory system examination did not reveal any abnormality. Electrocardiogram showed normal sinus rhythm. Chest X-ray showed normal cardiac size and clear lung field. Laboratory findings including complete blood count, liver function test, kidney function test, lipid profile and coagulopathy screening were all normal. CT scan of brain showed acute ischemic infarction on right middle cerebral artery territory. Carotid Doppler study was normal and lower limbs Doppler study excluded presence of any deep venous thrombosis. Tranthoracic echocardiography (TTE) showed an atrial septal aneurysm. An echo contrast study with agitated saline was performed to exclude presence of any patent foramen ovale (PFO). A transesophageal echocardiography (TEE) was adviced, but patient’s bystanders denied further investigation after explaining details of examination procedure. Patient was put on anti epileptic drugs and subsequently anti coagulated with warfarin. Patient was improved and discharged 8 days after admission with minimal residual neurological deficit.
DISCUSSION ASA is a congenital malformation of the septum primum layer of the interatrial septum and it is an infrequent finding in adult patients. ASA formation may be secondary to raised interatrial pressure gradients, producing a bulging septal shift toward the low-pressure side1 , however, it has been also found in patients with normal atrial pressures, 4 suggesting a primary (congenital?) malformation. According to autopsy study by Silver and Dorsey,1 patient having a protrusion of the aneurysm >10 mm beyond the plane of the atrial septum into either the right or left atrium considered to be having atrial septal aneurysm. However, according to diagnostic criteria of ASA proposed by Hanley and coworkers2 considered the atrial septum to be aneurysmal when a dilated portion protruded at least 15 mm beyond the plane of the atrial septum or when the atrial septum showed phasic excursions during the cardio respiratory cycle ≥15 mm with the base of the aneurysm ≥15 mm. In the largest series of cases of ASA diagnosed by TEE, Pearson and coworkers5 considered a septum aneurysmal when it had an excursion >10 mm into either the left or right atrium or a sum of the total excursion into the left or right atrium >10 mm, with a base width ≥15 mm. In our patient aneurismal protrusion was about 16 mm. The frequency of ASA in adult population is quite low (2.2%) 1 . Many authors suggested that ASA either alone or with combination of other defects may cause ischemic stroke due arterial embolism which is based on clinical studies demonstrating a statistical association between ASA and previous ischemic cerebral and/or peripheral embolic events. It has been speculated that ASA is a direct source of thrombus formation6 . This is supported by anecdotal findings demonstrating thrombotic material within the aneurysmal sac in patients at autopsy1 or cardiac surgery7 .Several studies suggested a possible relationship between ASA and ischemic stroke1, 5. The mechanism of stroke in patients with ASA remains poorly understood8 . Cerebral embolism might result from paradoxical embolism of venous thrombi across a right to left shunt, passage of a thrombus created on the left atrial side of the aneurysm 9 . Schneider et al6 reported a thrombus in 2 of 23 consecutive patients with ASA; in 1, thrombotic material appeared to override a PFO, suggesting paradoxical embolism; in the second, a thrombus was attached to the left atrial side of the aneurysm. In this patient CT brain demonstrated infarction possibly reflected cryptogenic stroke in a atrial septal aneurysm as no other possible causes of ischemic stroke was found.
CONCLUSION
Though there are no definitive mechanism documented for ischemic stroke in ASA patients, but isolated ASA may be a possible risk factor for ischemic stroke. Large scale prospective studies are required to understand the mechanism between atrial septal aneurysm and ischemic stroke.
ACKNOWLEDGEMENTS
The authors are grateful to the participants who voluntarily took part in the study. Authors wish to acknowledge the support provided by the Department of General Medicine, Nil Ratan Sircar Medical College, Kolkata for encouraging research and its publication. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Silver MD, Dorsey JS. Aneurysms of the septum primum in adults. Arch Pathol Lab Med. 1978; 102:62–5.
2. Hanley PC, Tajik AJ, Hynes JK, Edwards WD, Reeder GS, Hagler DJ, et al. Diagnosis and classification of atrial septal aneurysm by two dimensional echocardiography: Report of 80 consecutive cases. J Am Coll Cardiol.1985; 6:1370–82.
3. Gallet B, Malergue MC, Adams C, Saudemont JP, Collot AM, Druon MC, et al. Atrial septal aneurysm a potential cause of systemic embolism. Br Heart J. 1985; 53:292–7.
4. Hauser AM, Timmis GC, Stewart JR, Ramos RG, Gangadharan V, Westveer DC, Gordon S. Aneurysm of the atrial septum as diagnosed by echocardiography: analysis of 11 patients. Am J Cardiol. 1984; 53:1401-1402.
5. Pearson AC, Nagelhout D, Castello R, Gomez CR, Labovitz AJ. Atrial septal aneurysm and stroke: a transesophageal echocardiographic study. J Am Coll Cardiol. 1991; 18:1223-1229.
6. Schneider B, Hanrath P, Vogel P, Meinertz T. Improved morphologic characterization of atrial septal aneurysm by transesophageal echocardiography: relation to cerebrovascular events. J Am Coll Cardiol.1990; 16:1000-1009.
7. Grosgogeat Y, Lhermitte F, Carpentier A, Facquet J, Alhomme P, Tran TX. Aneurysme de la cloison interauriculaire révélé par une embolie cérébrale. Arch Mal Coeur. 1973; 66:169-177.
8. Mugge A, Daniel WG, Angermann C, Spes C, Khandheria BK, Kronzon L, et al. Atrial septal aneurysm in adult patients.A multicenter study using transthoracic and tarnsoesophageal echocardiography. Circulation.1965; 91:2785–92.
9. El-Chami MF, Hanna IR, Helmy T, Block PC. Atrial septal abnormalities and cryptogenic stroke: A paradoxical science. Am Heart Hosp J. 2005; 3:99–104.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





