IJCRR - 7(9), May, 2015
Pages: 78-84
Print Article
Download XML Download PDF
HISTOMORPHOLOGICAL ANALYSIS OF GRANULOMATOUS LESIONS IN A TEACHING HOSPITAL, PUDUCHERRY
Author: Sandhya Panjeta Gulia, M. Lavanya, Archana V., S. P. Arun Kumar, Kalaivani Selvi
Category: Healthcare
Abstract:Aims: The present study is done to study the frequency, morphology and to find out the etiology of granulomatous lesions by clinicopathologic correlation wherever possible. Materials and methods: A retrospective analysis of 75 biopsy sections was done from August 2010 \? July 2014. Diagnosis was confirmed by haematoxylin and eosine stained slides alongwith the special stains wherever required. Results: A total of 75 cases of granulomatous lesions were identified of which 42(56.0%) were malesand 33(44.0%) were females. Granulomas due to tuberculosis accounted for the majority of the types of granulomas,i.e,46 cases(61.33%), followed by 7 (9.33%)cases of foreign body granulomas, 5 (6.67%) fungal granulomas, 4 (5.33%) actinomycosis, granulomas of unknown etiology were - 4(5.33%) cases of granulomatous synovitis, 1(1.33%) cases of granulomatous cystitis and 5 (6.67%) cases of non infectious skin granulomas. The granulomatous skin lesions reported were mostly infectious \?3(4.0%) leprosy, 2 (2.67%) lupus vulgaris, 3(4.0%)cases of actinomycosis, 1(1.33%) scrofuloderma, and fungal granulomas \? 2(2.67%) subcutaneous phaeohyphomycosis 1(1.33%) maduramycosis, 1(1.33%) chromoblastomycosis, 1(1.33%)zygomycosis; 5(6.67%)non
infectious skin granulomas reported as granuloma annulare, erythema nodosum and acne agmeneta. Granulomatous lesions of the genitourinary tract constituted 8(10.67%) cases \? 3 (4.0%) tuberculosis of cervix and fallopian tube, 4 (5.33%) tuberculousepididymoorchitis and scrotal abscess; 1 (1.33%) granulomatous cystitis. Tuberculous lesions affecting the gastrointestinal tract were \? 3(4.0%)cases of fistula in ano, 1(1.33%) appendicular tuberculosis and 1(1.33%) case rectum.1(1.33%) case each of tuberculosis of spine and actinomycosis of tonsil was reported. AFB stain was positive in 14 (30.43%) cases of tuberculosis.
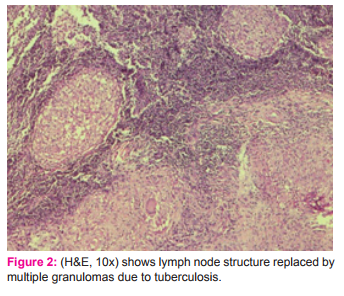
Conclusion: Tuberculosis was the commonest cause of granulomatous lesion and lymph nodes were the most common site affected. Epithelioid type of granuloma was the most common morphology.
Keywords: Epithelioid, Granuloma, Lymph nodes, Tuberculosis
Full Text:
INTRODUCTION
Granulomas are a characterstic microscopic finding of chronic inflammation. Granulomatous inflammation is considered as a response to pathogens and persistent irritants of exogenous and endogenous origin[1]. Granulomas are discrete collections of histiocytes with admixture of multinucleated giant cells and inflammatory cells[2]. The granulomas are formed as a result of series of events that involves the interplay of antigen (persistent endogenous / exogenous) resulting in activation of cell mediated type IV hypersensitivity reaction, activation of macrophages, T and B cell responses with release of chemical mediators of inflammation mainly cytokines. Classification of granulomas based on etiology could be: bacterial, fungal, viral/chlamydial, helminthic, foreign body type and unknown cause[3]. According to the morphology granulomas can be classified as: epithelioid, histiocytic, foreign body, necrobiotic/palisading and mixed inflammatory[3]. It is imperative to find out the correct etiology of the granulomatous lesions to start the appropriate treatment so correlating the clinical history with the histopathological findings proves to be valuable in establishing the correct diagnosis in majority of the cases. The present study was undertaken to find out the frequency, morphology and etiology where ever possible, of granulomatous lesions in the teaching hospital, and to compare with the similar studies.
MATERIALS AND METHODS
A retrospective study conducted in the department of Pathology, Sri Venkateshwaraa Medical College Hospital and Research Centre, Puducherry on the biopsies recieved from August 2010- July 2014 to analyse the frequency of granulomatous lesion. Alongwith routine haematoxylin and eosine stained sections, special stains like acid fast stain, fitefaraco and PAS stain was done wherever required.
RESULTS
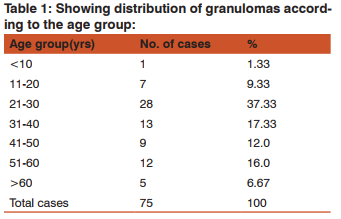
A total of 75 cases of granulomatous lesions were identified out of which 42(56.0%) were male patients and 33(44.0%) were females with M:F ratio of being 1.27:1. The maximum number of cases, 28 (37.33%), were reported in the age group of 21-30 years; only one case was less than 10 years and 5 (6.67%) cases were more than 60 years age(Table 1).
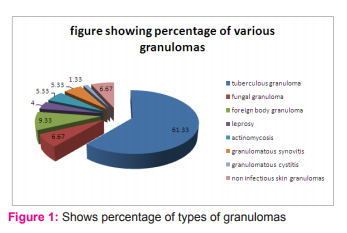
Granulomas due to tuberculosis (Fig. 1) accounted for the majority,i.e,46 cases(61.33%), followed by foreign body granulomas 7 (9.33%), fungal granulomas 5 (6.67%), actinomycosis4 (5.33%). Among the seven cases of foreign body granulomas, the most common etiologic agent was ruptured epidermal cyst with keratin and cholesterol granuloma in 4(5.33%) cases and xanthoma in 3(4.0%)cases. Granulomas of unknown etiology were – 4(5.33%) cases of granulomatous synovitis, 1(1.33%) case of granulomatous cystitis and 5 (6.67%) cases of non infectious skin granulomas.
According to the site of distribution (Table 2)the majority of cases of tuberculosis, 18(24%),were reported in the lymph nodes with 8 (44.44%) cases positive for acid fast stain. Bones and soft tissues accounted for total of 17(22.67%) cases of granulomatous lesions reported as tuberculousosteomyelitis, soft tissue tuberculosis, foreign body granulomas and granulomatous synovitis with no case showing acid fast positivity
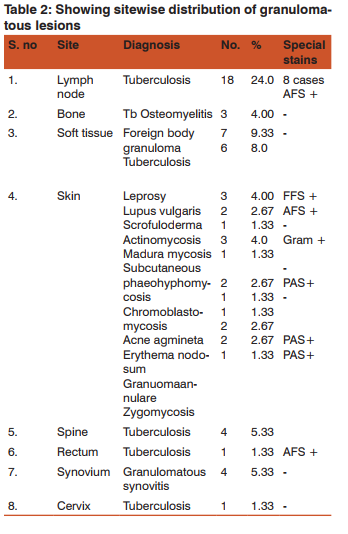
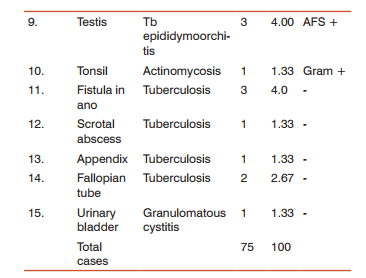
The granulomatous skin lesions reported were mostly infectious –3(4.0%) leprosy, 2 (2.67%)lupus vulgaris which showed acid fast positivity in both cases, 3(4.0%) cases of actinomycosis, 1(1.33%) case ofscrofuloderma, and 5 (6.67 %) cases of fungal granulomas, 2(2.67%) subcutaneous phaeohyphomycosis, 1(1.33%)case of maduramycosis,1(1.33%) case of chromoblastomycosis, 1(1.33%)case of zygomycosis; 5(6.67%)cases of non infectious skin granulomas reported as granuloma annulare, erythema nodosum and acne agmeneta. Granulomatous lesions of the genitourinary tract constituted 8(10.67%) cases – 3 (4.0%) tuberculosis of cervix and fallopian tube, 4 (5.33%) tuberculousepididymoorchitis and scrotal abscess; 1 (1.33%) granulomatous cystitis. Tuberculous lesions affecting the gastrointestinal tract were – 3(4.0%)cases of fistula in ano, 1(1.33%) appendix and 1(1.33%) case in rectum. 1(1.33%) case each of tuberculosis of spine and actinomycosis of tonsil were reported.
DISCUSSION
Majority of granulomatous lesions in our study were seen among the males 42 (56%) as compared to the females 33 (44%) with maximum number of cases in the age group of 21-30 years. These results were similar to the studies done by Adhikari RC et al [4], Permi HS et al [5] and Pawale JS [3] and Patel et al [6]. The present study showed that the etiology of the majority of granulomatous lesions was infectious in 57 (76%) cases which is in accordance to the study done by Bal et al [7]. In the present study the majority of the granulomas, 18(24%) cases, were reported in lymph nodes similar to the findings of Adhikari[4] who also reported lymph nodes (41.1%) as the commonest site of granulomas followed by skin and subcutaneous tissue (22.0%), bones and joints (11.5%), respiratory system (7.7%) and gastrointestinal tract (5.5%). Whereas Permi HS et al [5] in his study reported majority of the granulomas in skin and subcutaneous tissue with 68(24.72%) cases followed by lymph nodes in 59(21.46%)cases. In the study done by Permi HS [5] in 2012, lymph node tuberculosis was reported in 53(40.76%) cases, tuberculosis of bones and synovium in 35(26.92%)cases, cutaneous tuberculosis in 4(3.08%),intestinal tuberculosis in 14(10.76%),sinus tract in 4(3.08%) cases, fallopian tube in 2 (1.54%), bladder in 3 (2.30%) and kidney, lung, breast, epididymis in 1 (0.76%) case each. Patel et al [6] in 2013 reported 55% granulomas in lymph nodes, 5% respiratory tract, 8% skin, 5% GIT, 9% bones and joints, 10% head and neck, 6% reproductive system and 4% others. Whereas in the present study lymph node tuberculosis was reported in 18(24.0%)cases, skin and soft tissue tuberculosis in 9 (12.0%) cases, tuberculous osteomyelitis in 7(9.33%) cases, tuberculosis of rectum in 1(1.33%) case, appendicular tuberculosis in 1(1.33%), tuberculosis in female genital tract in 3(4.0%) cases, and tuberculosisin male genital tract in 4(5.33%) cases. Adults seem to develop tuberculousepididymoorchitis by direct spread from the urinary tract [8]. The usual presentation is painful inflamed scrotal swelling that is difficult to differentiate from acute epididymo – orchitis[9]. The diagnosis requires comprehensive evaluations – histology,cytology and microbiological investigations and further clinical follow up to avoid complications[10]. The most common cause of granuloma in our study was found to be tuberculosis in 61.33% cases which is similar to the findings of the studies done by Adhikari RC [4] et al in 61.7%, Permi HS [5] reported in 47.26%, Pawale JS in 49.41% [3] and Patel et al in 106 (81%) cases [6] who also reported tuberculosis as the commonest cause of granuloma. In the study conducted by Pawale et al [3],ZN stain was positive in 19(22.62%) out of 84 casesof tubercular granuloma. Whereas it was positive in 91(71%) out of 128 cases in the study of Krishnaswamy et al[11]. The study done by Permi HS [5] demonstrated tubercle bacilli in 27(20.74%) out of 130 cases. Whereas the findings of the present study are in contrast to the other studies where out of the total 46 cases of tubercular granulomas, acid fast stain was positive in 14(30.43%) and negative in 32 (69.57%)cases. The liquefaction of necrotic focus is considered to be associated with increased proliferation of AFB and infiltration of neutrophils with a high degree of hypersensitivity reaction [12]. In the study done by Chakrabarti et al [13] it was found out that culture positivity was found only in 13% cases of tuberculosis because of dead and altered organisms in the tissues.
The most common type of granuloma reported in the present study is necrotizing epithelioid type in 46 (61.33%) cases (Fig. 2) with the other types being epithelioid with suppuration (usually seen in fungal granulomas) 5 (6.67%), foreign body granulomas 7 (9.33%), necrobiotic granuloma 2 (2.67%) cases and also mixed inflammatory type (where the differential diagnosis of fungal infections and tuberculosis should be considered ) and histiocytic granulomas. In tuberculosis different types of granulomas can be encountered on histopathology like – epithelioid granuloma without necrosis, chronic nonspecific granuloma, chronic non-specific inflammation, epithelioid granuloma with necrosis and abscess [13]. Adhikari RC [4] also reported epithelioid granuloma as the commonest type in his study. Pawale JS [3] described tuberculoid granuloma 98 (57.65%), histiocytic granulomas in 29 (17.06%), foreign body granulomas in 17 (10.00%), ill defined granulomas in 13 (7.65%), mixed inflammatory granulomas in 11 (6.47%) and necrobiotic granulomas in 2 (1.18%). The commonest morphological pattern found in the study done by Permi HS et al [5] was epithelioid 165 (60% ), foreign body 35 (12.72%), ill defined 29 (10.54%), histiocytic 23 (8.36%), mixed inflammatory 19 (6.9%) and necrobiotic granulomas in 4 (1.45%) cases. Apart from tuberculosis, epithelioid granulomas are also seen in sarcoidosis, leprosy, fungal infections, crohns disease and tumor associated; epithelioid granulomas with suppuration can be seen in fungal infection, tuberculosis, cat-scratch disease and leishmaniasis; histiocytic granulomas found in parasitic infestation and fungal infections; foreign body granulomas seen as a reaction to foreign body; mixed inflammatory granulomas seen in parasiticinfestation, tuberculosis, leishmaniasis and chalazion[4].
In the skin granulomas of unknown etiology, 2 (2.67%) cases each of granuloma annulare and erythema nodosum and 1 (1.33%) case of acne agminata were reported. A case of perforating granuloma annulare was reported in 38 years male with multiple punched out ulcers over the trunk and proximal extremities covered by black eschar for which clinical differential diagnosis of ecthymagangrenosum and papulonecrotictuberculid was suggested. The biopsy picture showed degenerated collagen and mucin material surrounded by histiocytes. The mucin nature was suggested by PAS stain (Fig. 3) which showed a strong positivity. These findings were similar to those described by Pawale et al in their study [3]. These findings were similar to the observation made by Gautam et al[14],Billet A et al[15]and Joana Alexandra[16] reported 4(3.7%) cases of granuloma annulare.

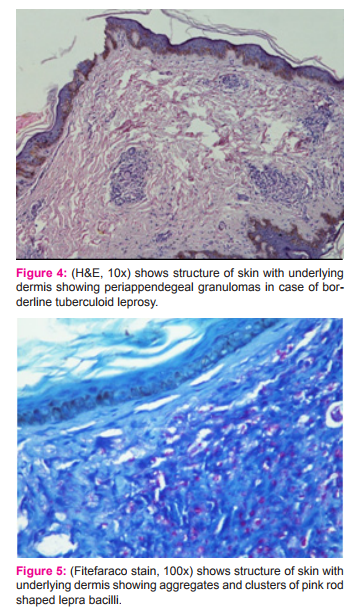
Acne agminata is idiopathic in etiology, though the histopathology shows tuberculoid granulomas, all other relevant investigations for tuberculosis were negative in the case similar to the case reported by Sule[17]. Out of the 30 cases of leprosy the fitefaraco stain was positive in 17(56.66%) and negative in 13(43.33%) cases in the study done by Pawale[3] whereas in the study done by Nayak et al it was positive in 25(44.64%) and negative in 31(55.35%) cases[18]. It was positive in only 9(25.72%) cases and negative in 31(55.36%) cases in the study done by Permi HS et al [5].Whereas in our study, the stain was positive in one case of borderline tuberculoid leprosy (Fig. 4) and (Fig. 5).
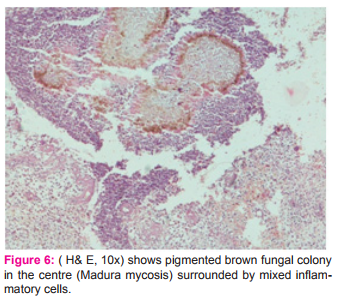
The commonest fungal lesion found in the study done by Pawale et al were 3(30%) cases of madura mycosis followed by 2 cases(20%) rhinosporiodosis, 2 (20%) cases of P.boydii and one case each of histoplasmosis and mucormycosis[3] whereas in the study done by Chavan SS et al rhinosporiodosis formed the majority, 34 (68%), of cases of fungal granulomas followed by madura mycosis in 8(16%)cases[19]. In the study done by Permi HS et al [5] fungal infections were aspergillus in 6(25%),rhinosporiodosis 4(16.6%), chromoblastomycosis in 3(12.5%), pseudolleshcheriaboydii in 2(8.33%), subcutaneous entomphothormycosis in 1(4.16%),mucormycosis in 2(8.33%),cryptococci in 2(8.33%), madura mycosis in 1(4.16%) and candida in 1 (4.16%) case. In the study by Gautam K et al, cutaneous chromoblastomycosis comprised 2.8% cases[14]. Whereas our study showed 2 (2.67%) cases of subcutaneous phaeohyphomycosis, 1 (1.33%) madura mycosis (Fig. 6), 1 (1.33%) zygomycosis, and 1(1.33%) chromoblastomycosis. The H and E stained sections of zygomycosis showed presence of broad septate hyphae with focal bulbous dilatations which was more evidently depicted in PAS stain. It was found that the patient was having diabetes mellitus due to which he developed secondary fungal lesion of cutaneous zygomycosis / mucormycosis. The microscopic picture of chromoblastomycosis sections revealed microabscessesand granulomatous infiltrate in the dermis with multiple brown coloured copper penny bodies.
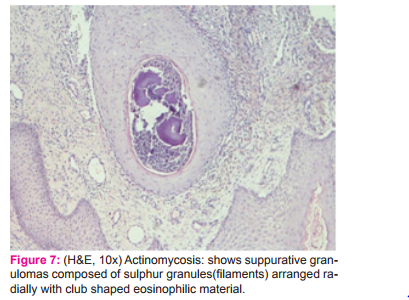
All 4(5.33%)cases of actinomycosis showed suppurative granulomas with central actinomycotic colonies seen on Haematoxylin and Eosine(Fig. 7) stained slides were confirmed by gram staining which showed gram positive filaments. These findings are comparable to the findings ofPawale JS [3], Permi HS et al[5], Mirza M et al[20] which was similar in our study. It is always advisable to search for the organisms in the centre of necrotic granulomas rather than peripheral viable and inflammatory tissue.
In the study conducted by Permi HS [5], foreign body granulomas were encountered in 23 cases – epidermal cyst with keratin and cholesterol granulomas in 13(56.52%) cases, xanthomas 4(17.4%) cases, sinus tract in 2(8.7%) cases, bile induced granulomas in 2(8.7%) cases and gouty arthritis in 2(8.7%) cases. In our study 7 cases of foreign body granulomas were reported and the probable etiologies identified were foreign body reaction to keratin and cholesterol, xanthogranuloma, suture granuloma and granuloma in the sinus tract. In the study of Permi HS et al[5],22(8.0%) cases of granulomas were of unknown etiology, PawaleJS et al[3] reported 11(6.47%) cases of granulomas of unknown etiology, i.e, granulomatous mastitis, granuloma annulare, sarcoidosis, granulomatous orchitis, granuloma in the pleura and mastoid antrum. The granulomas where etiology could not be found out in our study were 5(6.67%)cases - 4 (5.33%) cases of granulomatous synovitis, 2 (2.67%) cases of granuloma annulare, 1 (1.33%) case of acne agminata and 1 (1.33%) case of granulomatous cystitis. The etiology could not be established by doing stains like ZN and PAS hence they were grouped as granulomatous lesions[3,5] The definitive diagnosis to find out the exact etiology of granuloma formation could be made in 70 (93.33 %) cases out of total of 75 cases in the present study after doing special stains. After relevant special stains the etiological diagnosis could be confirmed in 95% cases in the study done by Patel et al [6]. Even after doing the special stains, in some cases, it is not possible to find out the etiology of the granulomatous lesion. hence ancillary studies of culture, serology, PCR may be required for confirmation.
CONCLUSION
The most common cause of granulomatous lesion in our study was tuberculosis with lymph node being the most common site. Majority of the granulomas had infectious etiology. According to the morphology epithelioid type was the predominant granuloma followed by foreign body type.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references in this manuscript. The authors are also grateful to the authors/publishers/editors of all those articles,journals and books from where the literature for this has been reviewed and discussed.
References:
1. Mariano M. Does macrophage deactivating factor play a role in the maintainence and fate of infectious granulomata? Mem. Inst. Oswaldo Cruz, 86:485-487,1991.
2. Weedon D. The granulomatous reaction pattern. In: Weedon D(ed). Skin Pathology, 2nded. Philadelphia: Churchill Livingstone;2002.pp193-220.
3. Jayashree Pawale, Rekha Purani, MH Kulkarni. A Histo- Jayashree Pawale, Rekha Purani, MH Kulkarni. A Histopathological study of Granulomatous Inflammations with an attempt to find the Aetiology. JCDR 2011;5(2):301-306.
4. Adhikari RC, Shrestha KB, Savami G. Granulomatous in- Adhikari RC, Shrestha KB, Savami G. Granulomatous inflammation: A histopathological study. Journal of Pathology of Nepal 2013;3:464-468.
5. Harish S. Permi, Jayaprakash Shetty K, Shetty K Padma, Teerthanath S, Michelle Mathias, Sunil Kumar Y, Kishan Prasad HL,Chandrika. A Histopathological Study of Granulomatous Inflammation. NUJHS 2012;2(1):15-19.
6. Vaidehi Patel, Jasmin Jasani, RajolI. Desai. The histo- Vaidehi Patel, Jasmin Jasani, RajolI. Desai. The histopathological study of granulomatous diseases in various organs to find the exact etiology of granulomas. IJBAR 2013;4(7):478-483.
7. BalA, Mohan H, Dhami GP. Infectious granulomatous dermatitis: aclinocopathologic study. Indian J Dermatol 2006;51:217-20.
8. Madeb R, Marshall J, Nativ O, Erturk E. Epididymal tuber- Madeb R, Marshall J, Nativ O, Erturk E. Epididymal tuberculosis: case report and review of the literature. Urology 2005;65(4):798.
9. Keyur N. Surati, Kaushal D. Suthar, Jainam K Shah. Isolat- Keyur N. Surati, Kaushal D. Suthar, Jainam K Shah. Isolated Tuberculous Epididymo-Orchitis: A Rare and Instructive Case Report. SEAJCRR 2012;1(3):46-50.
10. Vishnu Prasad Shenoy, Shashidhar Viswanath, Annet D Souza, Indira Bairy, Joseph Thomas. Isolated tuberculousepididymo-orchitis: an unusual presentation of tuberculosis. J Infect DevCtries 2012;6(1):92-94.
11. Krishnaswamy H, Job CK. The role of Ziehl Neelson and Flourescent stains in tissue sections in the diagnosis of tuberculosis. Indian Journal of Tuberculosis, 1974;21(10):18- 21.
12. Kunh, IIIC and Askin, F.B. Andersons Pathology, edited by J.M. Kissane, 8th Ed., Mosby Co, St. Louis, 1985, 852.
13. Ashish Kumar Chakrabarti, Krishna Kumar Halder, Shikha Das, Subrata Chakrabarti. Morphological Classification of Tuberuclous Lesions: Preliminary Observations. Ind. JTub 1994;41(139):139-142.
14. Gautam K, Pai RR, Bhat S. Granulomatous lesions of the skin. Journal of Pathology of Nepal 2011;1:81-86.
15. Billet A,Viseux V,Chaby G,Dascotte-Barbeau E,Gontier MF, Deneoux JP, Lok C. Perforating granuloma annulare with transfollicular perforation. Ann DermatolVenereol 2005;132(8-9):678-81.
16. Joana Alexandra Devesa Parente, Jose Alberto Machado Dores, Joao Manuel Pires Arhana. Generalized Perforating Granuloma Annulare: Case Report. Annal Dermatovenerol Croat 2012;20(4):260-262.
17. Sule RR, Athavale NV, Gharpuray MB. Lupus miliar- Sule RR, Athavale NV, Gharpuray MB. Lupus miliaris disseminates faciei. Ind J Dermatol Venereol Leprol 1992;58:102-4.
18. Nayak SV, Shivrudrappa AS, Mukamil AS. Role of fluorescent microscopy in detecting Mycobacterium leprae in tissue sections. Annals of diagnostic pathology 2003;7(2):78-81.
19. Chavan SS. A clinicopathlogical study of fungal lesions encountered in tissue sections (dissertation unpublished), Hubli, Karnataka university, 1998.
20. Mirza M, Sarwar M. Recurrent cutaneous actinomycosis. Pakistan Journal of Medical Sciences 2003;19:230-31.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





