IJCRR - 7(9), May, 2015
Pages: 28-32
Print Article
Download XML Download PDF
STUDY OF SACRUM AND ITS IMPORTANCE IN EPIDURAL BLOCK
Author: P. Sasikala, Arunkumar S. Bilodi
Category: Healthcare
Abstract:Aim of study: The objective of study is on sacrum for sacral hiatus due to its importance in epidural anesthesia.Place of study: This study was done in the department of anatomy at Velammal medical college hospital and research institute,Madurai, India.Period of study: This study was done during the month of February 2015.Materials and methods: 30 dry unknown human sacra from department of anatomy constituted the materials for the present study. Their dimensions were measured and sacral index were calculated for each sacrum. Shape, composition of sacrum, shape of sacral hiatus, level of sacral hiatus and curvature of the sacrum were noted down. Conclusion: Anatomical knowledge of sacral hiatus will be of great help in administering caudal analgesia through sacral hiatus.
Keywords: Sacral hiatus, Epidural block, Equilateral triangle
Full Text:
INTRODUCTION
Sacrum is a triangular bone having fusion of 5 sacral vertebrae. Normally, there is inverted U shaped gap in the posterior wall sacral canal called sacral hiatus. This sacral hiatus is due to failure of fusion of 5th sacral laminae that meet in median plane [1]. Vinod Kumar and Pandey S.N studies showed maximum sacral composition of 5 segments amounting to 69.8%. The sacral hiatus shows discrepancies in sizes and shapes [2]. Therefore Anatomy of sacral hiatus has said to increase the reliability and success of caudal epidural block [3]. Hiatus is covered by the skin, subcutaneous fatty layer and saccrococygeal membrane [4]. It has been reported that failure of caudal epidural block is due to absence of hiatus seen in 7.7% [5].
MATERIALS AND METHODS
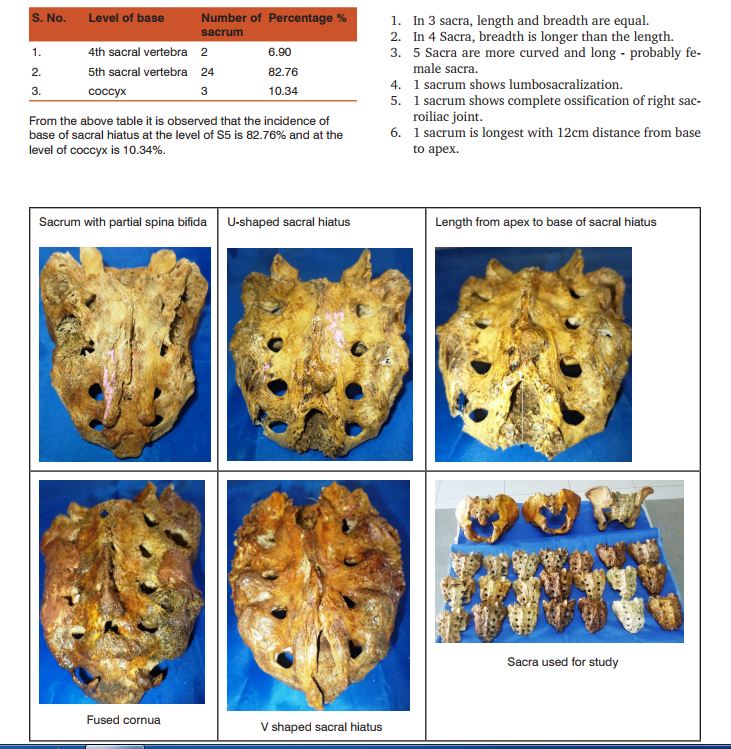
In the present study thirty human dry unknown sacrum of unknown sex were studied. Their length, breadth were measured and sacral index were calculated. Observations were made on sacral hiatus on their shapes and length. Observation was done on dorsal aspect of sacrum. Any irregularities of bones, shapes of hiatus, level of the apex and base of the sacral hiatus were analyzed. Depth of hiatus was also noted. Length of sacral hiatus was measured. Angulation of maximum curvature measured.
Observation and results
Table 7: Location of base of sacral hiatus
 Other observations are
Other observations are
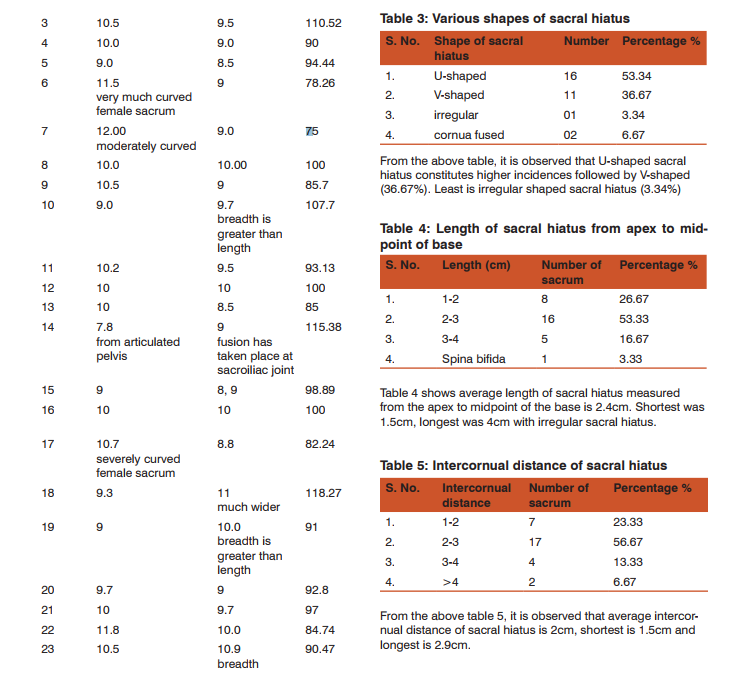
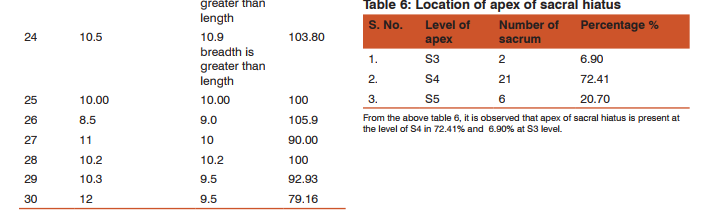
From the above table it is observed that the incidence of base of sacral hiatus at the level of S5 is 82.76% and at the level of coccyx is 10.34%.
Other observations are
1. In 3 sacra, length and breadth are equal
. 2. In 4 Sacra, breadth is longer than the length.
3. 5 Sacra are more curved and long - probably female sacra.
4. 1 sacrum shows lumbosacralization.
5. 1 sacrum shows complete ossification of right sacroiliac joint.
6. 1 sacrum is longest with 12cm distance from base to apex.
DiscussionCaudal epidural block is a procedure used in surgeries of anorectal and perineal in labour and also in lower limbs regions. So it is important to know the anatomy around sacral hiatus so as to carry out procedures without any hindrance [6]. Anupriya et al studies have shown maximum incidences of sacral hiatus of inverted V and U shaped 35.85 % and 26.42% [3]. It is very important to know the apex of sacral hiatus for the safety of the dura. In the studies of Anupriya et al, apex is found most commonly at the level of S4 (68.67%), 21.57% at the level of S5, S3 in 39.8 % [3]. From the present study, it is observed that location of apex of sacral hiatus is present at the level of S4 in 72.41% and least percentage is seen in 6.90% at S3 level. The position of base of sacral hiatus is also important. Position has varied from S4 to coccyx. In Anupriya et al studies it is S5 seen in 62.26%. It was lowest location of coccyx in their studies 24.53%, while in Nagar studies it was 72.6% [7], in Anjali studies it was 61.40% [8]. Present studies has shown base of sacral index in 82.76% at S5 level while in at level of coccyx it is found in 10.34%. Regarding maximum curvatures, Anupriya et al studies showed maximum curvatures of 53 dry sacrum. 40 sacrum showed maximum curvatures at the level of S3 in 75.47%, 12 bones at S4 foramen level in 22.64%, only one bone showed S5 level in 1.9% [3]. While in Anjali et al level of S3 in 80% of cases [8]. In the present study maximum curvatures were seen in 5 sacra (16.67%) at S3 and two sacra showed moderate curvatures (6.67%). Caudal Epidural Injections have proved more success, effective with less dose of local anesthesia and less vascular puncture by the practitioners [9, 10]. To manage low back pain, injections of corticostertoids by epidural route have been accepted as non surgical way of treatment [11]. Yoon JS et al have reported abnormality of the sacral hiatus makes canulation difficult and sometimes impossible in 5-10% of cases [12]. It is by guidance of ultra sound, anatomical details of the sacral hiatus, bilateral sacral cornua, apex of the sacral hiatus, anterior and posterior walls of the sacral canal and sacrococcygeal ligament can be detected clearly [13, 14, 15]. Since sacrum is a component of axial bone and pelvic girdle it is the most important bone for the identification of sex. It is sacral index that helps in determining the sex of sacra [16]. In the present study mean sacral index is 102.5 and the mean width of sacrum is 9.7. There are different shapes and sizes of sacral hiatus. There may be absence of sacral hiatus due to fusion of laminae in the midline or failure of fusion causing incomplete bony dorsal wall of sacral canal [17]. The various shapes of sacral hiatus in India were studied by Kumar et al. (1992).They were Inverted V, inverted U, dumbbell, irregular, bifid, absent, and other shapes. It was inverted V shape which was very commonly found [18]. In the present study sacral hiatus are U shaped 53.34%, V shaped 36.6%, Irregular 3.34%, cornua fused 6.67%. X-Rays of lumbosacral spine will be of useful in identifying the absence of sacral hiatus, shapes of sacral hiatus and level of SH apex and base [19]. Importance of sacral hiatus Sacral Hiatus is very important part of sacrum which has anatomical variations. Less than 3 mm depth of sacral hiatus causes difficulty in the insertion of the needle. Its different shapes, surrounding bony irregularities and defects in dorsal sacral canal should be studied in order to avoid failure of epidural block. Hence detailed knowledge of sacral hiatus is essential. (Agarwal et al) [20]. It is the genetic and racial factors that cause incidences of variations [21]. X Rays of lumbosacral spine will be of useful in identifying the absence of sacral hiatus, various shapes of sacral hiatus and levels of base and apex of sacral hiatus [19]. In the surgeries done by orthopedic surgeons caudal epidural block is used both as diagnostic and therapeutic tool. Failure rate is 35% is mainly due to variations of sacral hiatus and surrounding structures [22]. The incidence of variations may be due to genetic and racial factors. Exact location of sacral hiatus in caudal epidural block determines its success rate. The variabilities provided in this study should be kept in mind before giving Caudal Epidural Block. Further clinical trials are required to compare the existing techniques and our anatomical description to provide more data to support the results of this study.
CONCLUSION
The study on sacral hiatus gives us information of sacral hiatus regarding its patency and suitable for epidural block. If it is blocked, then epidural block cannot be carried out. So this study gives knowledge of sacral hiatus about its shape, extent etc especially for anesthetists, surgeons and gynecologists (spinal analgesia).
Carry home message
Anatomical knowledge of sacral hiatus has brought accomplishment of caudal epidural block.
ACKNOWLEDGEMENT
Authors thank colleagues from Department of Anatomy for their invaluable guidance and contribution of outstanding ideas. Authors would also thank authors of reference articles which are quoted in this article.
References:
1. Gray, Henry, 1825-1861; Williams, Peter L (Peter Llewellyn); Bannister, Lawrence H. 38th ed. / chairman of the editorial board, Peter L. Williams; editorial board, Lawrence H. Bannister ... [et al.]. New York : Churchill Livingstone, 1995. NLM ID: 9503696 [Book]
2. Kumar V, Pandey SN, Bajpai RN, Jain PN, Longia GS. Morphometric study of sacral hiatus. J Anat Soc India. 1992;41:7–13.
3. Anupriya A, Sophia MM. Anatomical study of sacral hiatus in south Indian population and its clinical significance in caudal epidural anesthesia. NJCA. 2014; 3(3): 128-136.
4. Sekiguchi M, Yabuki S, Satoh K, Kikuchi S. An anatomic study of the sacral hiatus: a basis for successful caudal epidural block. Clin J Pain. 2004 Jan-Feb;20(1):51-4. PubMed PMID: 14668657.
5. BLACK MG. Anatomic reasons for caudal anesthesia failure. Curr Res Anesth Analg. 1949 Jan-Feb;28(1):33-9. PubMed PMID: 18105828.
6. Brown DL. Atlas of Regional Anesthesia: Elsevier Health Sciences; 2010.
7. Nagar SK. Shah Medical College, Jamnagar, Gujarat: A study of sacral hiatus in dry human sacra. J Anat Soc India. 2004;53:18–21
. 8. Aggarwal A, Aggarwal A, Harjeet, Sahni D. Morphometry of sacral hiatus and its clinical relevance in caudal epidural block. Surg Radiol Anat. 2009 Dec;31(10):793-800. doi: 10.1007/s00276-009-0529-4. Epub 2009 Jul 4. PubMed PMID: 19578805.
9. Marhofer P, Schrögendorfer K, Koinig H, Kapral S, Weinstabl C, Mayer N. Ultrasonographic guidance improves sensory block and onset time of three-in-one blocks. Anesth Analg. 1997 Oct;85(4):854-7. PubMed PMID: 9322469.
10. Marhofer P, Schrögendorfer K, Wallner T, Koinig H, Mayer N, Kapral S. Ultrasonographic guidance reduces the amount of local anesthetic for 3-in-1 blocks. Reg Anesth Pain Med. 1998 Nov-Dec;23(6):584-8. PubMed PMID: 9840855.
11. Abdi S, Datta S, Trescot AM, Schultz DM, Adlaka R, Atluri SL, Smith HS, Manchikanti L. Epidural steroids in the management of chronic spinal pain: a systematic review. Pain Physician. 2007 Jan;10(1):185-212. Review. PubMed PMID: 17256030.
12. Yoon JS, Sim KH, Kim SJ, Kim WS, Koh SB, Kim BJ. The feasibility of color Doppler ultrasonography for caudal epidural steroid injection. Pain. 2005 Nov;118(1-2):210-4. Epub 2005 Oct 4. PubMed PMID: 16213088.
13. Blanchais A, Le Goff B, Guillot P, Berthelot JM, Glemarec J, Maugars Y. Feasibility and safety of ultrasound-guided caudal epidural glucocorticoid injections. Joint Bone Spine. 2010 Oct;77(5):440-4. doi: 10.1016/j.jbspin.2010.04.016. Epub 2010 Sep 24. PubMed PMID: 20869897.
14. Chen CP, Wong AM, Hsu CC, Tsai WC, Chang CN, Lin SC, Huang YC, Chang CH, Tang SF. Ultrasound as a screening tool for proceeding with caudal epidural injections. Arch Phys Med Rehabil. 2010 Mar;91(3):358-63. doi: 10.1016/j. apmr.2009.11.019. PubMed PMID: 20298824.
15. Najman IE, Frederico TN, Segurado AV, Kimachi PP. Caudal epidural anesthesia: an anesthetic technique exclusive for pediatric use? Is it possible to use it in adults? What is the role of the ultrasound in this context? Rev Bras Anestesiol. 2011 Jan-Feb;61(1):95-109. doi: 10.1016/S0034- 7094(11)70011-3. Review. PubMed PMID: 21334512.
16. Hardlika A. Practical anthropometry. Philadelphia: Winster Institute; 1939. Quoted by Krogman 1962
. 17. Letterman GS, Trotter M. Variations of the male sacrum: Their significance in caudal analgesia. Surg Gynecol Obstet. 1944;78:551–5.
18. El-Monem AH, Neven MG. A morphological study of the sacral hiatus. Zagazig University Medical Journal (ZUMJ) 2006;12:2877–86.
19. Mustafa MS, Mahmoud OM, El Raouf HH, Atef HM. Morphometric study of sacral hiatus in adult human Egyptian sacra: Their significance in caudal epidural anesthesia. Saudi J Anaesth. 2012 Oct-Dec;6(4):350-7. doi: 10.4103/1658-354X.105862. PubMed PMID: 23493625; PubMed Central PMCID: PMC3591553.
20. Aggarwal A, Aggarwal A, Harjeet, Sahni D. Morphometry of sacral hiatus and its clinical relevance in caudal epidural block. Surg Radiol Anat. 2009 Dec;31(10):793-800. doi: 10.1007/s00276-009-0529-4. Epub 2009 Jul 4. PubMed PMID: 19578805.
21. Chhabra N. An Anatomical Study of Size and Position of Sacral Hiatus; Its Importance in Caudal Epidural Block.. IJHSR. 2014; 4(12): 189-196. 22. Mayuri J, Vijay G, Vasudha N, Anita G, Asha P. Anatomical Study Of Sacral Hiatus In Dry Isolated Sacra. J Res Med Den Sci. 2014; 2(2): 43-46. doi:10.5455/jrmds.20142210
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





