IJCRR - 7(9), May, 2015
Pages: 20-27
Print Article
Download XML Download PDF
THREE DIMENSIONAL EVALUATION OF CONDYLAR HEAD INCLINATION WITH RESPECT TO RAMUS AMONG POST PUBERTAL CLASS II PATTERNS
Author: Abhilasha Goyal, R. H. Kamble, Sunita Shrivastav, Narendra Sharma
Category: Healthcare
Abstract:Objective: To assess the condylar head inclination with respect to ramus in Angle's Class II division 1 and division 2 skeletal patterns using Digital Volume Tomography. Material and method: The sample consisted of 45 post pubertal patients who were divided on the basis of clinical and cephalometric analysis into three groups - skeletal Class I, Class II division 1 and Class II division 2. The selected cases underwent Digital Volume Tomography and the images obtained were used to assess condylar head inclination, mediolateral and anteroposterior thickness of the condylar head on right and left sides for all the three groups. ANOVA, Least significance difference and Paired student's t test were done. Results: The Class II division 2 group showed significantly more anteriorly angulated condyles as compared to those of Class II division 1 and Class I groups on both right and left sides. Class II division 1 group showed significantly smaller mediolateral dimension as compared to Class I and Class II division 2 groups. The anteroposterior dimension was not significantly different in all three groups studied. Conclusion: There exists a variation in the condylar morphology in the various skeletal malocclusions examined. The individuals with Class II division 2 malocclusion had a tendency towards having more anteriorly angulated condyles. Also the mediolateral dimension of condylar head of individuals with Class II division 1 malocclusion is smaller than Class II division 2 and Class I malocclusions.
Keywords: Condyle, Class II malocclusion, DVT
Full Text:
INTRODUCTION
In dentofacial orthopaedics, thorough knowledge of the skeletal and dental components that contribute to a particular malocclusion is essential as these may influence the approach to treatment. Form and function are considered to be closely linked, also it follows that the morphology of the temporomandibular joint (TMJ) might be related to functional forces. The role of mandibular growth has specially intrigued practitioners due to its variability and relative unpredictability. There are several factors that could affect the TMJ morphology and position, such as age, sex, facial growth pattern, pathological or functional alterations, decreased or increased muscular activity, and dental occlusion changes.1-4 As a result of these changes, there is a remodelling and reconfiguration of the TMJ surfaces as an adaptation response.5 However, the amount of this remodelling will depend on the mechanical and functional conditions to which adjacent structures are faced.4, 5 Studies evaluating maxillary and mandibular skeletal and dental positions and vertical components of Class II patients have reported conflicting results. Most of the studies selected Class II patients on a dental basis, but patients with a dental Class II malocclusion may have a Class I or a Class II skeletal pattern.6 Few studies evaluated patients with both skeletal and dental Class II malocclusion.7-9 The only exceptions are the studies by Gianelly et al10, who studied the position of condyle in the fossae in Class II patients with deep-bite and no overjet, and the study by Ricketts, 11-12 in which the Class II group were studied. He stated that those with skeletal Class II division 2 malocclusions, when compared with normal Class I or Class II division 1 subjects have larger masticatory muscles that are oriented in a more anterior direction. It shows that TMJ loading in patients with skeletal Class II division 2 patterns differs from those having other dentofacial morphologies. It has been claimed that Class II division 2 malocclusions do not exhibit a distinct skeletofacial pattern, and, with the exception of the maxillary central incisor position, there is no other difference in morphology when compared with Class II division 1 subjects. This view, however, has been challenged by others who claim that Class II division 2 malocclusion is a distinct dentoskeletal entity.13 As the mandible and the TMJ can be loaded differently in persons with varied dentofacial morphologies, one could hypothesize that the condyle might differ between people with various malocclusions. There is no doubt that scarce information exists on the morphologic assessment of the dentofacial complex and the factors that may or may not contribute to its growth. Three-dimensional high resolution imaging allows the quantification of facial bone tissues in approximately real dimensions (1:1 ratio) without significant magnification, distortion or superimposition providing clear visualization of the areas of interest and opening new perspectives for analyzing these joints with any difficulty. The purpose of this study was to determine the relationship between condylar characteristics measured using preorthodontic three dimensional reconstructions of post pubertal Class II patients and their skeletal malocclusions.
MATERIALS AND METHOD
Sample selection
Forty five patients, ranging in age from 18 to 40 years, were selected from the outdoor patients Department of Orthodontics, Sharad Pawar Dental College and students of Datta Meghe Institute of Medical Sciences (DU), Sawangi (M), and Wardha. The selected patients were divided into three groups based on clinical and cephalometric examination as Group 1- Skeletal Class I, Group 2- Skeletal Class II division 1 and Group 3- Skeletal Class II division 2 comprising of 15 patients each. The cephalometric criteria used for dividing the sample into Skeletal Class I and Skeletal Class II are described in Table 1.
Radiographic analysis
The lateral cephalograms were taken by a Planmeca proline cc (Finland) machine. Tracings were digitized and analyzed using Vistadent software. The selected cases, after cephalometric evaluation, were subjected to Digital Volumetric Tomography. The samples were scanned using Phillips Allura Xper FD20 3D RA, Digital Subtraction Angiography unit (Netherlands) with exposure parameters of 80 kVp, 10 Ma and 4-5 sec with Field of View- 12” 270? rotation. The images were obtained with the patients in maximum dental intercuspation and the head positioned so that the Frankfort horizontal plane was perpendicular to the floor. Three dimensional (3D) images, as well as, multiplanar reconstruction (MPR) images were obtained using 3D RA software at computer work station, which were then evaluated using Intruis Suite R2 software.
For each sample a total of 3 measurements (for right and left side each) were calculated:
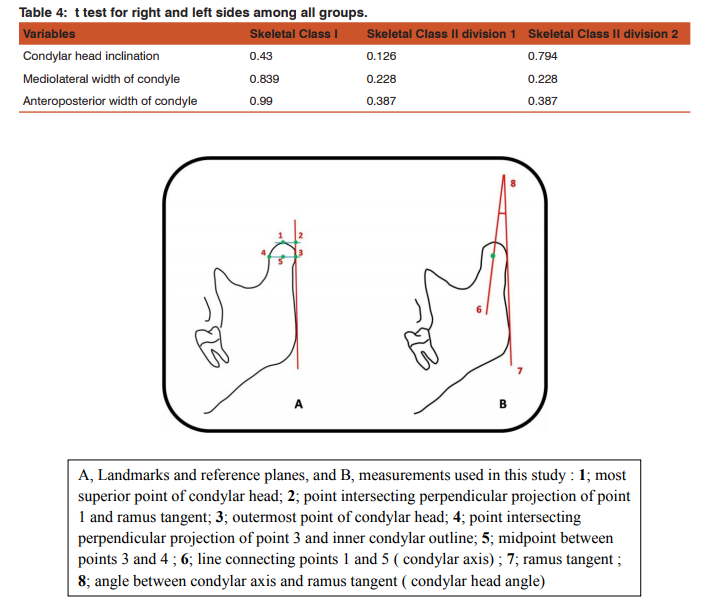
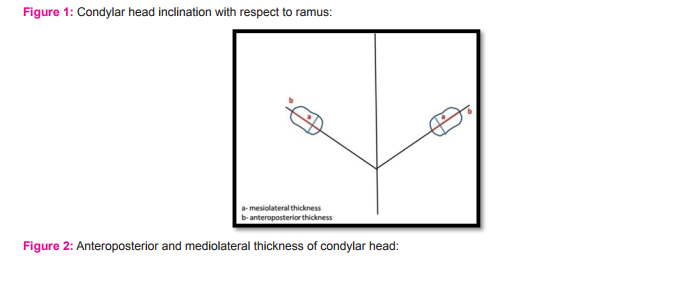
1. Condylar head inclination with respect to ramus This measurement was completed according to the format described by Sug-Joon Ahn et al 14 (F ig.1)
2. Mediolateral thickness of condylar head Measured as the largest mediolateral dimension. (Fig.2a)
3. Anteroposterior thickness of condylar head Measured as the largest anteroposterior dimension. (Fig.2b)
 One Way Anova test revealed statistically significant values (p value=0.001*) between the groups and within the groups. Significant findings were obtained when Group 1 was compared to Group 2 and Group 3 (p value=0.001). Also, when Group 2 was compared to Group 3 the values were statistically significant with (p value=0.001).) Statistical analysis
Statistical analysis
Descriptive statistics for all variables were studied. Group differences were tested with one-way ANOVA and Multiple Comparison Least Significant Difference test. Paired Student t-test was used for each measurement to evaluate the average of differences between the sides for each element of the sample of all the groups.
RESULTS
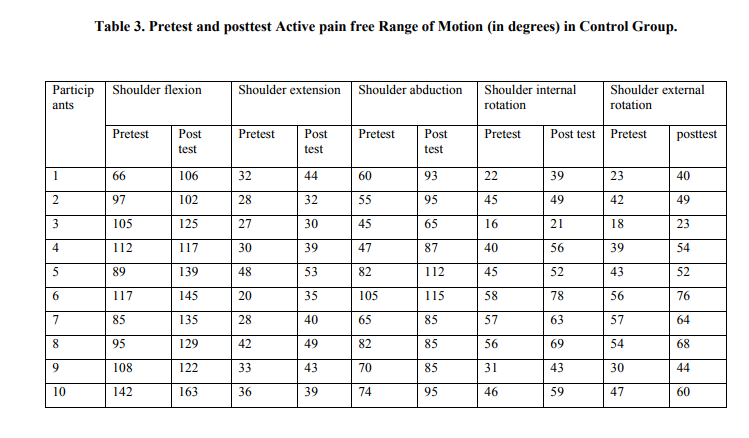
Statistical description of the condylar head inclination and dimensions of condyle according to skeletal pattern are given in Table 2 and 3. With respect to the condylar head inclination (for both right and left sides) One Way Anova test revealed statistically significant values (p value=0.001*) between the groups and within the groups. Significant findings were obtained when Group 1 was compared to Group 2 and Group 3 (p value=0.001). Also, when Group 2 was compared to Group 3 the values were statistically significant with (p value=0.001).
For the thickness of condyle mediolaterally, for both right and left sides, it was observed that there is statistically significant difference when comparing Group 1 to Group 2(p value=0.01) and Group 2 to Group 3(p value=0.01). No statistically significant difference was found when comparing Group 1 to Group 3(p value=0.09). A statistically non significant difference was identified regarding the anteroposterior thickness of the condyle when the three groups were compared. A paired Student’s t test showed no statistical difference between right and left sides for all the variables. (Table 4)
DISCUSSION
Understanding the TMJ morphology in the Class I and Class II groups remains a challenge for orthodontists. In literature it has been stated that the condyle and the fossa might differ in shape and their interrelations among people with various malocclusions while the mandible and the temporomandibular joint can be loaded differently in persons with diverse dentofacial morphologies. The difficult visualization of the TMJ (due to its complex anatomy and the superimposition of adjacent structures) might be a factor responsible for the discrepancies in the results of different studies concerning this joint. Nowadays other methods are used for evaluating 3-dimensional morphology of the skeletal structures of TMJ such as cone beam computed tomography (CBCT), multi slice computed tomography (MSCT) and Digital Volume Tomography (DVT). All of these provides an optimal imaging of the osseous components of the TMJ and gives a full size truly volumetric 3D description in real anatomical (1:1) size. The evidence of its accuracy was evaluated by Anuraag B. Choudhary et al15 who assessed the diagnostic quality of images generated using the then newly developed digital volume tomography (DVT) system and comparing them with conventional images obtained from patients with maxillofacial trauma. The results and statistical analysis clearly indicated that the diagnosis of maxillofacial traumatic injuries involving the midface and mandibular condylar region (condylar head) is significantly enhanced using Digital Volume Tomography compared with conventional radiographs. Condylar head inclination with respect to ramus in all three groups on right and left sides, were evaluated. The Class II division 2 group showed significantly more anteriorly angulated condyles as compared to those of Class II division 1 and Class I groups on both right and left sides (Fig 3). This shows altered glenoid fossa relationship in the experimental group. The Class II division 1 group had increased anterior condylar angulation as compared to Class I group but less as compared to Class II division 2 groups. Findings of this study can be explained by the research done by Gail Burke et al1 who evaluated the correlation between the skeletal growth pattern and condyle glenoid fossa relation using preorthodontic lateral cephalograms and tomograms of 136 preadolescent Class II patients. He stated that patients with vertical facial morphologic characteristics displayed posteriorly angled condyles whereas anteriorly angled condyles were significantly correlated to the patients with a horizontal facial morphology. Similar findings were obtained by Elias G. Katsavrias16 who studied the shapes of the condyle and the glenoid fossa in patients with Class II division 1, Class II division 2, and Class III malocclusions. Axially corrected tomograms of 189 patients were used (109 Class II division 1, 47 Class II division 2, and 33 Class III). The Class III group had a more elongated and anteriorly inclined condylar head with a wider and shallow fossa. In the present study the Class II division 2 group consisted of predominantly horizontal growers while the Class II division 1 group consisted of a mixed sample of vertical and horizontal growers. This explains the increased angulation in the Class II division 1 group than the Class I group. Also the methodology used in the previous studies was different from the one used in this study. Although no significant difference was found between the right and left sides for condylar head inclination, the mean value obtained for the right side in all three groups were greater than that of the left side. This asymmetry may be attributed to side preferences during mastication. To the best of our knowledge to date, no study has been conducted to study the condylar head inclination with respect to ramus in skeletal Class II division 1 and Class II division 2 cases. The previous studies only concentrated on the association of growth pattern in Class II cases with the condylar head inclination. The correlation obtained between condylar head inclination and facial morphology is consistent with results previously reported in early literature. Posterior inclination of the condyles has been shown to dominate the individuals with the Classic long face syndrome, and anterior inclination of the condylar head can be associated with counter-clockwise mandibular rotators.17 It has also been reported in the literature that reduced condylar growth represents clockwise rotation of the mandible in relation to the cranial base.18 Proliferation of condylar cartilage and endochondral ossification of the condyle occurs via a complex of biomechanical interactions. The magnitude, direction and duration of the resultant condylar growth may be influenced by genetic determinants as well as intrinsic and extrinsic control factors.
Animal studies have shown that mandibular protrusive appliances can result in increased chondrocytic proliferation and subsequent osseous development of the condyle in a posterior and posterosuperior direction.19-22 the magnitude of the temporomandibular joint’s adaptability and subsequent alteration will also be dependent upon maturational age, adaptive potential and neuromuscular function.1 The dimension of the condyle showed statistically significant results for mediolateral dimension of the condyle. On comparison of Class II division 1 showed significant values when compared with Class I and Class II division 2 whereas the values were not significant when Class I and Class II division 2 were compared. Overall, the mean for Class II division 2 was greater than that on Class I and Class II division 1 respectively for both mediolateral and anteroposterior dimensions of the condyle (Fig 4). Krisjane et al23 studied the TMJ parameters in Class II and Class III patients using volumetric three dimensional imaging and they concluded that there were no statistically significant differences in the anteroposterior width of the condyle in both the groups. These findings are in favour of the present study. We found a statistically significant difference in the mediolateral dimension of the condyle; the values being least for Class II division 1and greatest for Class II division 2 samples. This variation may be attributed to the mixed sample present in the Class II division 1 group (horizontal and vertical growers). However no significant difference was found when Class I and Class II division 2 group were compared. The axial view is most appropriate to assess the symmetry between the condyles in the anteroposterior and mediolateral aspects because it shows both condyles in the same image. This also permits measuring the real dimensions of the condyles. The dimensions of the condyle showed no statistically significant differences between the right and left sides. These findings of symmetry are supported by various studies present in the literature. Cohlmia et al24 assessed the temporomandibular joint in Class I, Class II division 1, Class II division 2 and Class III patients and found that the anteroposterior thickness of the condylar head was not significantly different between the right and left sides in the sample studied. Vitral et al25 and Rodrigues et al26 using the same methodology, found similar results in a Class II division 1 subdivision and Class I sample , respectively. Also the results of study by Rodrigues et al26 on a sample of Class II division 1 and Class II malocclusion support the findings of the present study. These results seem to confirm the statement of Ben-Bassat et al27 that the occlusal features might be associated with TMJ structure remodelling to create symmetrical relationships. Contrasting results were shown in the study done by Vitral et al28 on subjects with normal occlusion. He found statistically significant difference in the linear measurement of the mediolateral diameter of the condylar process between the right and left sides.
CONCLUSIONS
The individuals with Class II division 2 malocclusion had a tendency towards having more anteriorly angulated condyles as compared to individuals with Class II division 1 and Class I malocclusions. Individuals with Class II division 1 malocclusion showed significantly smaller mediolateral dimension as compared to Class I and Class II division 2 individuals. The anteroposterior dimension was not significantly different in the three groups examined.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. Authors are also grateful to the authors / editors / publishers of all those articles, journals and books from where the literature has been reviewed and discussed.


References:
1. Gail Burke, Paul Major, Kenneth Glover and Narasimha Prasad. Correlations between condylar characteristics and facial morphology in Class II adolescent patients. Am J Ortho Dentofac Orthop. 1998; 114 (3): 328-336.
2. Ishibashi H, Takenoshita Y, Ishibashi K, Oka M. Age-related changes in the Human mandibular condyle: a morphologic, radiologic and histologic Study. J Oral Maxillofac Surg. 1995; 53(9):1016–23.
3. Yale SH, Allison BD, Hauptfuehrer JD. An epidemiological assessment of mandibular condyle morphology. Oral Surg Oral Med Oral Pathol. 1966; 21(2): 169–77. 4. Kurusu A, Horiuchi M, Soma K. Relationship between occlusal force and mandibular condyle morphology. Angle Orthod. 2009; 79(6):1063–9.
5. Arnett GW, Milam SB, Gottesman L. Progressive mandibular retrusion idiopathic condylar resorption-Part II .Am J Orthod Dentofacial Orthop. 1996; 110(2):117– 27.
6. M. Ozgar Say?n, Hakan Turkkahramana. Cephalometric Evaluation of Nongrowing Females with Skeletal and Dental Class II, division 1 Malocclusion. Angle Orthod. 2005; 75:656–660
.7. Hunter WS. The vertical dimensions of the face and skeletodental retrognathism. Am J Orthod. 1967; 53:586–595.
8. Bacon W, Eiller V, Hildwein M, Dubois G. The cranial base in subjects with dental and skeletal Class II. Eur J Orthod. 1992; 14:224–228.
9. Ishii N, Deguchi T, Hunt NP. Craniofacial morphology of Japanese girls with Class II division 1 malocclusion. J Orthod. 2001; 28:211–215.
10. Gianelly AA, Petras JC, Boffa J. Condylar position and Class II deep-bite, no-overjet malocclusions. Am J Orthod Dentofacial Orthop. 1989; 96:428-32.
11. Ricketts RM. Variations of the temporomandibular joint as revealed by cephalometric laminagraphy. Am J Orthod. 1950; 36: 877-98.
12. Ricketts RM. Tomographic research studies of the temporomandibular joint and occlusion. In: Provocations and perceptions in craniofacial orthopaedics. Dental science and facial art. Denver: Rocky Mountain Orthodontics; 1989. p. 901-46.
13. Elias G. Katsavrias. Morphology of the temporomandibular joint in subjects with Class II division 2 malocclusions. Am J Orthod Dentofac Orthop. 2006; 129:470-8.
14. Sug-Joon Ahn,Tae-Woo Kim, Dong-Yul Lee, and Dong-Seok Nahm. Evaluation of internal derangement of temporomandibular joint by panoramic radiographs compared with panoramic resonance imaging. Am J Orthod Dentofacial Orthop.2006; 129:479-85
15. Anuraag B. Choudhary , Mukta B. Motwani , Shirish S. Degwekar , Rahul R. Bhowate , Panjaj J. Banode , Abhilasha O. Yadav and Aarti Panchbhai. Utility of Digital Volume Tomography in Maxillofacial trauma. Journal of Oral and Maxillofacial Surgery. 2011 June; 69 (6):135-140.
16. Elias G. Katsavrias, Demetrios J. Halazonetis. Condyle and fossa shape in Class II and Class III skeletal patterns: A morphometric tomographic study. Am J Ortho Dentofac Orthop. 2005; 128:337-46.
17. Bjork A, Skieller V. Facial development and tooth eruption: An implant study at the age of puberty. Am J Orthod. 1972; 62:339-83.
18. Bjork A, Skieller V. Normal and abnormal growth of the mandible: A synthesis of longitudinal cephalometric implant studies over a period of 25 years. Eur J Orthod. 1983;5: 1-46,
19. Stockli PW, Willert HG. Tissue reactions in the temporomandibular joint resulting from anterior displacement of the mandible in the monkey. Am J Orthod .1971; 60:142- 55.
20. McNamara JA Jr. Neuromuscular and skeletal adaptations to altered function in the orofacial region. Am J Orthod .1973; 64:578-606?
21. McNamara JA Jr, Hinton RJ, Hoffman DL. Histologic analysis of temporomandibular joint adaptation to protrusive function in young adult rhesus monkeys (Macaca mulatta). Am J Orthod. 1982; 82:288-98.
22. McNamara JA Jr, Bryan FA. Long-term mandibular adaptations to protrusive function: an experimental study in Macaca mulatta. Am J Orthod. 1987; 92:98-108.
23. Zane Krisjane, Ilga Urtane, Gaida Krumina, Katrina Zepa. Three-dimensional evaluation of TMJ parameters in Class II and Class III patients. Stomatologija, Baltic Dental and Maxillofacial Journal. 2009, Vol. 11, No. 1.
24. Jeff Cohimia, Joydeep Ghosh, Pramod K. Sinha, Ram S. Nanda and G. Frans Currier. Tomographic assessment of temporomandibular joint in patient with malocclusion. Angle Orthod. 1996; 66(1): 27-36.
25. Robert Willer Farinazzo Vitral, Carlos de Souzza Telles. Computed tomographic evaluation of TMJ alteration in patients with Class II division 1 subdivision malocclusion: condylar symmetry. Am J Ortho Dentofac Orthop. 2002 April; 121: 396-375.
26. Andreia Fialho Rodrigues, Marcelo Reis Fraga and Robert Willer Farinazzo Vitral. Computed tomography evaluation of the temporomandibular joint in Class I malocclusion patients: Condylar symmetry and condyle-fossa relationship. Am J Orthod Dentofacial Orthop. 2009;136:192-8
27. Ben-Bassat Y, Yaffe A, Brin I, Freeman J, Ehrlich Y. Functional and morphological-occlusal aspects in children treated for unilateral posterior cross-bite. Eur J Orthod 1993; 15: 57-63.
28. Robert Willer Farinazzo Vitral, Marcio Jose da Silva Campos, Andreia Fialho Rodrigues and Marcelo Reis Fragac. Temporomandibular joint and normal occlusion: Is there anything singular about it? A computed tomographic evaluation. Am J Orthod Dentofacial Orthop. 2011; 140:18-24.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





