IJCRR - 7(10), May, 2015
Pages: 75-78
Print Article
Download XML Download PDF
CLINICO LABORATORY PROFILE OF SCRUBTYPHUS AT A RURAL TERTIARY CARE HOSPITAL IN SOUTH INDIA
Author: Saleem M., Shivekar S., Gopal R.
Category: General Sciences
Abstract:Scrub typhus is a reemerging rickettsial infection caused by Orientia tsutsugamushi transmitted through the bite of larval forms of a trombiculid mite. The clinical presentation of scrub typhus mimics other acute febrile illnesses thus making it difficult to diagnose clinically. The present work is a retrospective study of clinico - laboratory profile of seropositive cases of scrub typhus presenting to our hospital over a period of 2 months. The clinical and laboratory profile of all cases of scrub typhus positive by ELISA (IgM) over a period of 2 months were studied retrospectively. Out of 364 cases tested for scrub typhus, 103(27.57%) were positive for scrub typhus by serology. The incidence was high among women than men. The most common symptoms reported were fever with chills and rigor followed by diarrhea and vomiting. Among the laboratory parameters thrombocytopenia and elevated serum transaminase was the most common abnormality. Majority of them responded to doxycycline. Scrub typhus is an important cause of acute undifferentiated pyrexial illness, therefore all the clinically suspected cases should be confirmed by a relatively sensitive method and specific test. In present study one third of clinically suspected cases were turned out positive for
scrub typhus by serology.
Keywords: Scrub typhus, Rural hospital, South India
Full Text:
INTRODUCTION
Scrub typhus is a Rickettsial infection caused by Orientia tsutsugamushi, mainly transmitted by the bite of larvae of a trombiculid mite. (1) The symptoms of scrub typhus are indistinguishable from other illnesses like leptospirosis, malaria, and dengue fever.(2) Epidemics of scrub typhus have been documented worldwide. In India, Goa, North eastern states and south India have reported the disease. (3-9). It is wide spread in Japan, Taiwan, China, South Korea, Nepal, Australia and Indonesia (10-12) The common symptoms and signs seen in scrub typhus cases is fever, chills with rigors , mylagia, headache and rash with dysfunction of organs such as kidney (acute renal failure), liver (hepatitis), lungs (acute respiratory distress syndrome, central nervous system (meningitis),GIT (vomiting and diarrhea) or circulatory collapse with haemorrhagic features (13). Eschar is a characteristic features of scrub typhus (14, 15). Although it is characteristic, many studies have reported scrub typhus without eschar.(4) Puducherry is a small coastal town surrounded by many villages from Tamil Nadu. Presently there is an increase in number of cases of scrub typhus presenting with fever, rash and hepatorenal involvement. In the present study, the clinical profile and laboratory findings of these patients were studied.
MATERIALS AND METHODS
The present retrospective study was carried out in a rural tertiary care hospital of Puducherry, South India. All patients who tested positive for IgM antibody against the 56kDa protein of O.tsutsugamushi by ELISA during the study period of two months, were included in this study. A total number of 364 blood samples were received for serological testing for scrub typhus from the patients with fever from various outpatient departments, emergency services and indoor patients of our hospital. All the samples were screened for IgM antibodie by using ELISA kit (Scrub Typhus Detect TM, InBios International USA). Clinical and laboratory test results of all positive cases were studied from case records.
RESULTS
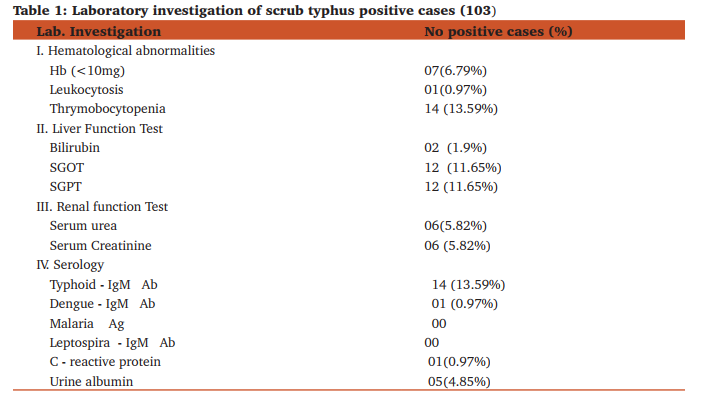
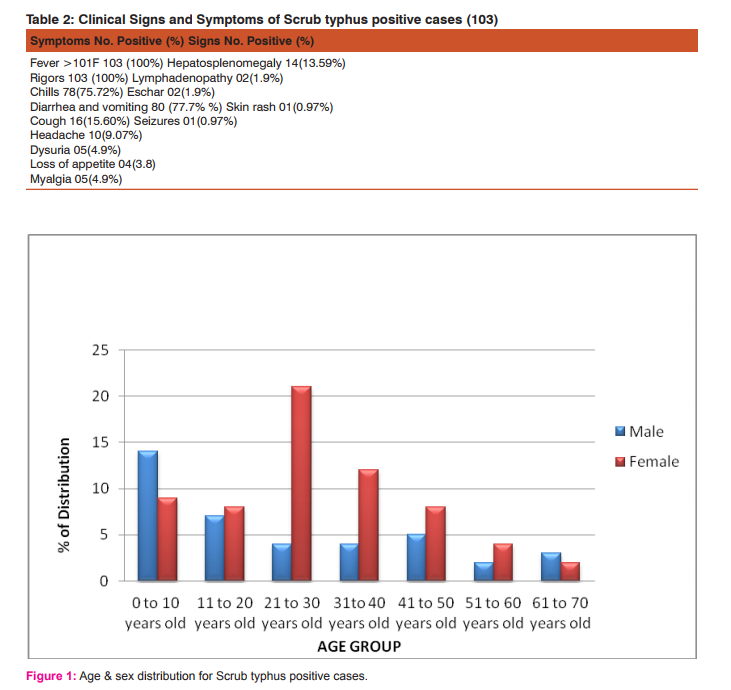
The patients attending our hospital are mostly from the rural areas of Puducherry and adjacent areas of Tamil Nadu (Villupurum district). Out of 364 cases studied, 103(27.6%) tested positive for scrub typhus. All the positive cases were in the age group of 1 – 70 years. There were 64 (62%) women and 39 (38%) men. (Figure 1) Table 1 shows the signs and symptoms of positive cases. In the present study most of the patients presented with one or more of the following symptoms viz fever, chills, rigors, cough, headache, diarrhea, vomiting, loss of appetite, and myalgia. The most common sign was hepatosplenomegaly and lymphadenopathy. Eschar and skin rashes were present only in three cases. Table 2 shows the laboratory findings of these patients. Thrombocytopenia, leukocytosis, elevated liver enzymes i.e. SGOT and SGPT, raised serum urea and creatinine were the common findings. Serum bilirubin was elevated only in two cases. The result of present study showed maximum cross reactivity between typhoid and scrub typhus. one case was positive for dengue IgM antibody also . A majority of the patients responded dramatically to treatment with doxycycline.
DISCUSSION
In India scrub typhus has been reported from the period of World War II. The first major outbreak was recorded among the soldiers deployed along the India- Myanmar border.(16) Ever since subsequently scrub typhus has been observed all over the country. In the present study 103 (27.57%) patients with fever were diagnosed as scrub typhus. A similar positivity was also observed in other area i.e. Goa (34%) (4) North Western India (24.7%) (17) and Tirupati (39%).(18) In the present study scrub typhus seropositivity was comparatively high in women. This may be because of occupational exposure to the vector in the fields. Clinically patients with scrub typhus present with acute febrile illness with non-specific signs and symptoms (19). In our study, the commonest presentation seen was fever with chills (100%), rigors (75%) and cough with respiratory distress. The other predominant symptoms were diarrhea, vomiting and abdominal pain. Hepatosplenomegaly and lymph node enlargement was also observed in few cases. Eschar with skin rash is diagnostic feature of scrub typhus, (20,21) however, in our study only three patients had eschar. A similar presentation was also reported in earlier studies RR. The clinical presentation of scrub typhus mimics dengue and leptosprosis (22). In the present study gastrointestinal symptoms were frequently reported among scrub typhus patients, which probably is a differentiating feature from similar infections. Similar to other studies (14, 23) majority of patients had elevated serum transaminases, serum urea and creatinine without evidence of multiorgan involvement; however serum bilirubin was normal in all patients except two. Other laboratory findings noted were thrombocytopenia and leukocytosis. Widal test showed maximum positivity (13.6%) among the scrub cases. This shows the possibility of production of cross reacting antibodies between the two pathogens. Even though 56 kDa protein is specific to scrub typhus a detailed molecular study typhus has to be carried out to assess the antigenic piracy between these two pathogens. (24) In conclusion Scrub typhus is a reemerging rickettsial infection in most parts of India with increasing case reports in the last one decade. Scrub typhus should be considered in the differential diagnosis of all cases of acute undifferentiated pyrexia. Early diagnosis and treatment reduces the morbidity and mortality associated with the disease.
ACKNOWLEDGEMENT
Authors acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
References:
1. Mahajan SK. Scrub typhus. J Assoc Physicians India 2005; 53: 954-8.
2. Kothari VM, Karnad DR, Bichile LS. Tropical infections in the ICU J Assoc Physicians India 2006; 54 : 291-8.
3. Chogle AR. Diagnosis and treatment of scrub typhus - the Indian scenario. J Assoc Physicians India 2010; 58 : 11-2.
4. Kedareshwar PS, Rodrigues S, Nevrekar RP, Dias L, Dias A, Vaz M and Gomes E. Scrub typhus in patients reporting with acute febrile illnessat a tertiary health care institution in Goa Indian J Med Res, 2012 Dec;136: 1020-24.
5. Sharma A, Mahajan S, Gupta ML, Kanga A, Sharma V. Investigation of an outbreak of scrub typhus in the himalayan region of India Jpn J Infect Dis 2005; 58 : 208-10
.6. Batra HV. Spotted fevers and typhus fever in Tamil Nadu. Indian J Med Res 2007; 126 : 101-3.
7. Mathai E, Lloyd G, Cherian T, Abraham OC, Cherian AM. 4. Serological evidence for the continued presence of human rickettsioses in southern India. Ann Trop Med Parasitol 2001; 95 : 395-8.
8. Ittyachen AM. Emerging infections in Kerala: a case of scrub typhus Natl Med J India 2009; 22 : 333-4.
9. Varghese GM, Abraham OC, Mathai D, Thomas K, Aaron R, 5. Kavitha ML, et al. Scrub typhus among hospitalised patients with febrile illness in South India: magnitude and clinical predictors J Infect 2006; 52: 56-60.
10. Lee YS, Wang PH, Tseng SJ, Ko CF, Teng HJ, 2006. Epidemiology of scrub typhus in eastern Taiwan Jpn J Infect Dis 2004; 59: 235–238.
11. Nagano I, Kasuya S, Noda N, Yamashita T. Virulence in mice of O. tsutsugamushi isolated from patients in a new endemic area in Japan. Microbiol Immunol 1996 ; 40: 743– 47.
12. Zhang LJ, He S, Jin YM, Li L, Li XM, Liu LY, Yu HL, Yu Q, Chen CF, Wang SW,. A rapid, sensitive and reliable diagnostic test for scrub typhus in China. Indian J Med Microbiol 2011; 29: 368–371.
13. Buddha BT, Belbase RH, Zimmerman MD, Woods CW, Reller LB, and Murdoch DR. Clinical Features of Scrub Typhus. Clin Infect Dis 2006; 42 (10): 1505-06.
14. Kim DM, Won KJ, Park CY, Yu KD, Kim HS, Yang TY, Lee JH, Kim HK, Song HJ, Lee SH, Shin H. Distribution of eschars on the body of scrub typhus patients: a prospective study. Am J Trop Med Hyg. 2007 May;76(5):806-9.
15. Sourabh Aggarwal; Alka Sharma; Vishal Sharma. Eschar: a cutaneous clue to scrub typhus. Braz J Infect Dis 2012; 16(4) 407-408.
16. Singh P. Scrub typhus, a case report: Military and regional significance. Med J Armed Forces India 2004;60:89-90.
17. Sinha P, Gupta S, Dawra R, Rijhawan P. Recent outbreak of scrub typhus in North Western part of India Indian. Journal of Medical Microbiology 2014; 32(3): 247-50.
18. Ramyasree A, Kalawat U, Rani ND, Chaudhury A. Seroprevalence of Scrub typhus at a tertiary care hospital in Andhra Pradesh Indian J Med Microbiol 2015;33:68-72.
19. Rajapakse S, Rodrigo C, Fernando D. Scrub typhus: pathophysiology, clinical manifestations and prognosis Asian Pac J Trop Med. 2012 Apr;5(4):261-4.
20. Lee SH, Kim DM,Cho YS,Yoon SH, and Shim SK.Usefulness of Eschar PCR for Diagnosis of Scrub Typhus J Clin Microbiol. 2006 Mar; 44(3): 1169–1171.
21. Kundavaram AP, Jonathan AJ, Nathaniel SD, Varghese GM. Eschar in scrub typhus: a valuable clue to the diagnosis M. J Postgrad Med. 2013 Jul-Sep;59(3):177-8.
22. Girija S, Rajan A, Sathiyanarayanan J, Mangaiyarkarasi T. , Saban P, Sunil S, Gopal R Scrub typhus- An emerging disease in South India IJRRMS 2013;3(4):11-13.
23. Sankhyan N , Saptharishi LG, Sasidaran K, Kanga A and Singh SC. Clinical profile of scrub typhus in children and its association with hemophagocytic lymphohistiocytosis Indian Pediatrics , 2014 august ;(51): 15651-653.
24. Chao CC, Huber ES, Porter TB, Zhang Z, and Ching WM. Analysis of the Cross-Reactivity of Various 56 kDa Recombinant Protein Antigens with Serum Samples Collected after Orientia tsutsugamushi Infection by ELISA Am J Trop Med Hyg 2011 Jun 1; 84(6): 967-72.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





