IJCRR - 7(10), May, 2015
Pages: 66-70
Print Article
Download XML Download PDF
PREVALENCE OF DIFFERENT MENSTRUAL IRREGULARITIES IN WOMEN WITH ABNORMAL UTERINE BLEEDING(AUB)- AN OBSERVATIONAL STUDY
Author: Tabassum Kotagasti
Category: General Sciences
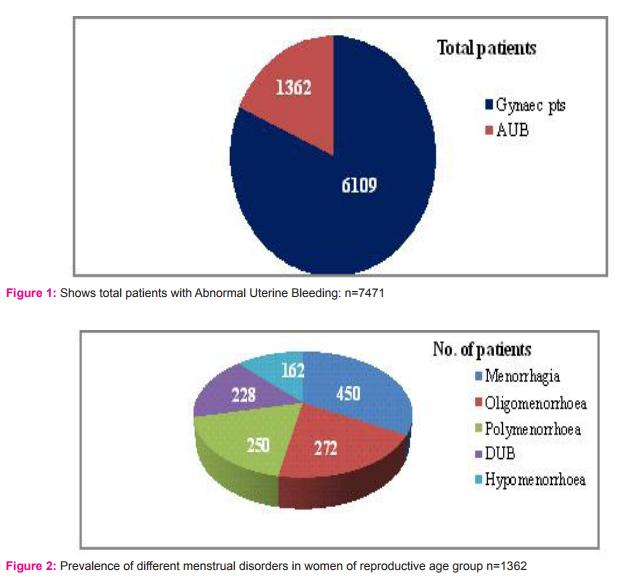
Abstract:Introduction: Abnormal Uterine Bleeding (AUB) is a term which refers to menstrual bleeding of abnormal frequency, duration or quantity. It is a common gynecological complaint accounting one third of outpatient visits to gynecologist. Abnormal Uterine Bleeding includes Oligomenorrhoea, Polymenorrhoea, Hypomenorrhoea, Menorrhagia, Metrorrhagia and Dysfunctional Uterine Bleeding. This paper elicits the prevalence of different menstrual disorders among women with Abnormal Uterine Bleeding. Objective: To observe the prevalence of different menstrual irregularities in patients with Abnormal Uterine Bleeding. Methodology: The study was carried out in the Gynaec out Patient Department of National Institute Unani Medicine Hospital during the years of 2014\?2015.Total 1362 patients of Abnormal Uterine Bleeding were included in the study on basis of clinical sign and symptoms and history. Results: Among 7471 Gynaec patients 1362 (18.23%) patients were found with Abnormal Uterine Bleeding (AUB) and out of 1362 patients of Abnormal Uterine Bleeding highest were with menorrhagia i.e. 450 (33%) and least were with hypomenorrhoea i.e. 162 (11.89%). Prevalence of menorrhagia was highest between the ages of 25-34 years. Conclusion: It is concluded that the prevalence of menorrhagia is high among all Abnormal Uterine Bleeding and it affects woman health status, quality of life and social integration. It is suggested that menstrual complaints should be thoroughly evaluated
and treated on a top priority.
Keywords: Abnormal uterine bleeding, Menstrual irregularities, Different age group, Prevalence
Full Text:
INTRODUCTION
Menstrual disorders are common gynecological problem for medical visits among women of reproductive age.(1) Heavy menstrual bleeding affects up to 30% of women in their reproductive period.(2)Abnormal Uterine Bleeding may be defined as any variation from the normal menstrual cycle such as changes in regularity and frequency, duration of flow or amount of flow and it accounts for one third of patients to visits gynecologists. (3) It occurs in 9-14% of women between menarche to menopause, significantly impacting quality of life and imposing financial burden.(4-6) Abnormal Uterine Bleeding by definitions may be subdivided into subcategories based on volume of menstruation, regularity, frequency, duration, chronicity and reproductive status. International Federation of Gynecology and Obstetrics revised terminology system, for Abnormal Uterine Bleeding in reproductive age women was introduced in 2011.(7)Previously terms such as Menorrhagia, Menometrorrhagia, Oligomenorrhoea, Polymenorrhoea, Hypomenorrhoea and Dysfunctional Uterine Bleeding were used. Now it is referenced as Polyp, Adenomyosis, Leiomyoma, Malignancy and Hyperplasia- Coagulopathy, Ovulatory dysfunction, Endometrial, Iatrogenic and Not yet classified. Abnormal Uterine Bleeding may be due to some pelvic pathology. (8) In different menstrual disorders menorrhagia is a common gynecological condition which adversely affects quality of life of many women. Heavy menstrual bleeding or menorrhagia is the most common complaint among Abnormal Uterine Bleeding. It has been defined as excessive menstrual blood loss more than 80ml and it significantly interferes with the woman’s physical, social and emotional status. It can occur alone or in combination with other symptoms.(9, 10)Over 5% of women ages between 30-49 years consult gynecologist each year with this complaint.(11) There are a number of etiological factors responsible for Abnormal Uterine Bleeding and gynecological evaluation is essential. History and physical examination will help to establish the causes to adapt management to the individual patient to prevent unnecessary invasive procedures which may have their limitations. In this paper the prevalence of different menstrual disorder, especially of menorrhagia was worked out among patients with Abnormal Uterine Bleeding.
METHODOLOGY
The present study was undertaken in Gynae Out Patient Department, National Institute of Unani Medicine Hospital, Bangalore during the year of 2014-2015 to find out prevalence of menstrual disorders in reproductive age women with Abnormal Uterine Bleeding. In this study out of 7471 patient of different gynaec complaints 1362 (18.23%) patients both unmarried and married were found with various menstrual disorders. A detailed history regarding the age, menstrual irregularities like frequency of cycle, duration of flow and amount of flow were enquired and were recorded. The data presented in the study are based on clinical examination and on history.
RESULTS
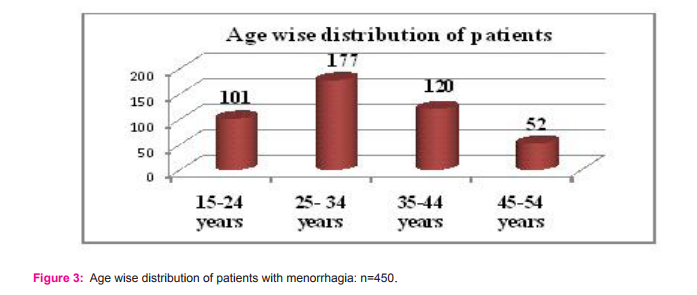
In the present study it was observed that the prevalence of menorrhagia was high as compared to other Abnormal Uterine Bleeding, followed by oligomenorrhoea, polymenorrhoea, Dysfunctional Uterine Bleeding and hypomenorrhoea. The observed data are as: Out of 7471gynecological patients1362 were found with Abnormal Uterine Bleeding. (Figure.1). Out of 1362 patients of Abnormal Uterine Bleeding, 450 (33%) patients had menorrhagia followed by 272 (19.97%) had oligomenorrhoea, 250 (18.35%) had polymenorrhoea, 228 (16.74%) patients had dysfunctional uterine bleeding and least i.e. 162 (11.89%) patients had hypomenorrhoea. (Figure.2) Out of 450 patients of menorrhagia maximum patients were found in the age group of 25-34 years i.e. 177 (39.33%) followed by 120 i.e. 26.66% in the age group of 35- 44 years, 101 patients i.e. 22.44% were in the age group of 15-24 years and least were in the age group of 45-54 years i.e. 52 (11.55%). (Figure.3)
DISCUSSION
In the present study out of 1362 patients with Abnormal Uterine Bleeding the highest prevalence of patients were with menorrhagia i.e. 450(33%) followed by 272 (19.97%) patients with oligomenorrhoea, 250 (18.35%) patients with polymenorrhoea,228(16.74%) patients with dysfunctional uterine bleeding and least i.e. 162 (11.89%) patients were with hypomenorrhoea found. According to studies conducted in India by Bang RA, Bhatia JC, Jayaseelam et al. among women of reproductive age group the prevalence of oligomenorrhoea or cycles longer than 35 days ranged from 8-22%. (12-17) Reports of irregular bleeding in the past three months in the WHO multicentric study ranged from 8-83%. In their study Hernandez I, Cervera-Aguilar R et al they reported the frequency of irregular cycles as 9-16 %.( 18) However, the highest prevalence of irregular cycles was reported 30% in a selected population of Vietnamese factory workers. (19) In Lebanon 15% of women reported menstrual irregularity at their last gynecological visit. (20) In the adolescent study the frequency of oligomenorrhoea was reported to be 1.1% in Chile, 4.5% in Nigeria(21) 8% in Turkey (22) and 42% in Thailand. (23) Menorrhagia accounts for 12% of gynecological referrals for surgical intervention. A study by Coulter A, Bradlow J, Agass M, et al. revealed that 60% of women underwent a hysterectomy within five years of referral.(24) In the present study among other Abnormal Uterine Bleeding the highest prevalence of menorrhagia was seen between the ages of 25-34 years, but Coulter A, Kelland J, Peto V et al. reported in their study that the prevalence of heavy bleeding was 15% in the age group of 30-40 years. (25) The prevalence of Abnormal Uterine Bleeding is estimated to be 11-13% and it increases 24% with age in those aged 36-40 years. (8)A survey was done in woman age between 18-50 years the rate was 53 per 1000 women. (26)Abnormal Uterine Bleeding and menorrhagia directly affects women’s quality of life (27-30) and ultimately has a significant impact on health. (31) In developing countries prevalence Abnormal Uterine Bleeding appears to affect about 5-15% of women of reproductive age and probably a higher percentage of women in older age groups. Data on prevalence of Abnormal Uterine Bleeding is limited, but it is a major cause of gynecological morbidity, affecting up to 1 in 5 women at some point during their reproductive lifespan. (32) Nine to fourteen percent of reproductive age women have blood loss that exceeds 80 ml(33)and Abnormal Uterine Bleeding is a leading indication or hysterectomy, the most common major gynecological operation in women. (34, 35) Abnormal Uterine Bleeding is of more concern, because excessive or prolonged bleeding may cause undue disruption of women’s daily activities. Prolonged and excessive bleeding may provoke serious medical consequences or exacerbate anaemia and in a certain percentage of cases may eventually be life threatening if left untreated.
CONCLUSION
The present study revealed the prevalence of menorrhagia is high in patients with Abnormal Uterine Bleeding. The highest prevalence of menorrhagia was seen between the ages of 25-34 years. Patients presenting with menstrual irregularities must be screened properly as incidence of menorrhagia is high in reproductive age group. Frequency of menstrual disorders and their impact on women’s health status, quality of life and social integration suggest that proper evaluation and treatment should be given a higher priority. Prophylactic treatment should focus on reducing the quantity of blood loss in addition iron supplement prevents or reduces the risk of bleeding complications in haemostatic challenges such as surgery.
ACKNOWLEDGMENT
The author acknowledged all the editors and authors of the journal for choosing their articles for reference
Conflict of interest: The author has no conflict of interest
Source of funding: For this study funding is not required. It is based on observation of the collected data.
References:
1. Kjerulff KH, Erickson BA, Langenberg PW. Chronic gynecological conditions reported by US women: findings from the national health interview survey, 1984 to 1992. Am. J Public Health, 1996; 86:195–9.
2. Market Opinion and Research International (MORI). Women’s health in 1990.Research study conducted on behalf of Parke-Davis Laboratories]. London: MORI; 1990.
3. Barnard K, Frayne SM, Skinner KM, Sullivan LM. Health status among women with menstrual symptoms. J Women’s Health (Larchmt), 2003; 12:911-9.
4. Cote I, Jacobs P, Cumming D. Work loss associated with increased menstrual loss in the United States. Obstet Gynecol, 2002; 100:683–7
. 5. Mahmoud Aseel Ghazi Rifat, Endometrial Histo-pathological Changes in Women with Abnormal Uterine Bleeding in Kirkuk City, a Clinico-pathological Study, Medical Journal of Babylon, Vol. 10, No. 3, 2013, 1023
6. Mary Gayle Sweet, MD, Tarin A. Schmidt-Dalton, MD, Patrice M. et al, Evaluation and Management of Abnormal Uterine Bleeding in Premenopausal Women, Am Fam Physician, 1;85(1), 2012, 35-43.
7. Millar W. Hysterectomy, 1981/82 to 1996/97. Health Rep, 2001; 12:9–22.
8. Frick KD, Clark MA, Steinwachs DM, Langenberg P, Stovall D, Munro MG et al. Financial and quality-of-life burden of dysfunctional uterine bleeding among women agreeing to obtain surgical treatment. Women’s Health Issues, 2009; 19:70–8.
9. Committee on Practice Bulletins—Gynecology. Practice bulletin no. 128: diagnosis of Abnormal Uterine Bleeding in reproductive-aged women. Obstet Gynecol, 2012; 120:197.
10. National Collaborating Centre for Women’s and Children’s Health; National Institute for Health and Care Excellence. NICE guideline CG44: heavy menstrual bleeding. London: Royal College of Obstetricians and Gynecologists, 2007.
11. Effective health care. The management of menorrhagia, Effective Health Care Bulletin 2013, 9:1-14.
12. Matteson KA, Boardman LA, Munro MG, Clark MA. Abnormal Uterine Bleeding: a review of patient-based outcome measures. Fertil Steril, 2009; 92:205.
13. Bang RA, Bang AT, Baitule M, Choudhary Y, Sarmukaddam S, Tale O.High prevalence of gynecological diseases in rural Indian women. Lancet, 1989; 1:85-88.
14. Jeyaseelan L, Rao PS. Effect of occupation on menstrual cycle length: causal model. Hum Biol, 1995; 67:283– 290.
15. Bhatia JC, Cleland J, Bhagavan L, Rao NSN. Levels and determinants of gynecological morbidity in a district in south India. Stud Fam Plann, 1997; 28:95– 103.
16. Hernandez I, Cervera-Aguilar R, Verdara MD, Ayala AR. Prevalence and etiology of secondary amenorrhea in a selected Mexican population. Ginecol Obstet Mex, 1999; 67:374- 376.
17. Nunez Troconis J, Amesty N, Sandoval J. Trastornos menstruales en estudiantes universitarias. Amenorrhoea, Oligomenorrea. Rev Obstet Ginecol Venez, 1990; 50:138– 141.
18. Deeb M, Ghorayeb F, Kabakian-Khasholian T, Yeretzian J, Aswad N. Measuring gynecological morbidity: evaluating two different data sources from Beirut. Healthc Women Int, 2003; 24:254- 265.
19. Walraven G, Ekpo G, Coleman C, Scherf C, Morison L, Harlow SD. Menstrual disorders in rural Gambia. Stud Fam Plann, 2002; 33:261–268.
20. Intermediate Technology Bangladesh. Investigation into the Sanitary, Protection Needs of Poor Women in Bangladesh. Dhaka: Intermediate Technology Bangladesh, 1992.
21. Matsuda S, Luong NA, Hoai NV et al. A study of complaints of fatigue by workers employed in Vietnamese factories with newly imported technologies. Ind. Health, 1997;35:16- 28
22. Fakeye O, Adegoke A. The characteristics of the menstrual cycle in Nigerian schoolgirls and the implications for school health programmes. Afr J Med Med Sci 1994; 23:13-17.
23. Vicdan K, Kukner S, Dabakoglu T, Ergin T, Keles G, Gokmen O. Demographic and epidemiologic features of female adolescents in Turkey. J Adolesc Health 1996; 8:54-58.
24. Coulter A, Bradlow J, Agass M et al. Outcomes of referrals to gynaecology outpatient clinics for menstrual problems: an audit of general practice records. Br J Obstet. Gynaecol,1998:789–796.
25. Coulter A, Kelland J, Peto V et al. Treating menorrhagia in primary care. An overview of drug trials and a survey of prescribing practice. Int. J Technol Assess Health Care,1995, 11:456–471.
26. Kadir RA, Lukes AS, Kouides PA, Fernandez H, Goudemand J. Management of excessive menstrual bleeding in women with hemostatic disorders. Fertil Steril, 2005; 84: 1352–9.
27. Kjerulff KH, Erickson BA, Langenberg PW. Chronic gynecological conditions reported by US women: findings from the National Health Interview Survey, 1984 to 1992. Am J Public Health, 1996; 86:195.
28. Barnard K, Frayne SM, Skinner KM, Sullivan LM. Health status among women with menstrual symptoms. J Women’s Health (Larchmt), 2003; 12:911–9.
29. Cote I, Jacobs P, Cumming D. Work loss associated with increased menstrual loss in the United States. Obstet Gynecol, 2002; 100:683–7.
30. Millar W. Hysterectomy, 1981/82 to 1996/97. Health Rep, 2001; 12:9–22.
31. Frick KD, Clark MA, Steinwachs DM et al. Financial and quality-of-life burden of dysfunctional uterine bleeding among women agreeing to obtain surgical treatment. Women’s Health Issues, 2009; 19:70–8.
32. Coulter A, Noone A, Goldacre M. General practitioners’ referrals to specialist outpatient clinics. BMJ, 1989; 299:304– 308.
33. Hallberg L, Hogdahl AM, Nilsson L, Rybo G. Menstrual blood loss- a population study. Variation at different ages and attempts to define normality. Acta Obstet Gynecol Scand, 1966; 45:320–351.
34. Bernstein SJ, McGlynn EA, Siu AL. The appropriateness of hysterectomy, a comparison of care in seven health plans. Health Maintenance Organization Quality of Care Consortium. JAMA, 1993; 269: 2398– 2402.
35. Santha Ram NV, Murthy NVA. Abdominal hysterectomies at area hospital, Point Fortin, Trinidad, West Indies. Int J Gynecol Obstet, 1989; 28:137–141.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





