IJCRR - 7(10), May, 2015
Pages: 43-48
Print Article
Download XML Download PDF
IS CAROTID ATHEROSCLEROSIS AN INDICATOR OF GENERALIZED ATHEROSCLEROSIS: AN AUTOPSY STUDY
Author: Lokesh Haswani, Harendra Kumar M.L., Kiran J.
Category: General Sciences
Abstract:Background: Atherosclerosis is one of the major causes of morbidity and mortality worldwide. Autopsy study is a gold standard for atherosclerosis. None of the study done on autopsy to prove the carotid atherosclerosis has the generalized nature. Objective: To examine the association between carotid atherosclerosis with coronary, aorta and renal arteries in non cardiac patients using histological analysis. Methods: We histologically examined 91 patients died of non cardiac cause. Atherosclerotic lesion in carotid, coronary, aorta and renal arteries were noted and graded according to modified AHA classification of atherosclerosis using morphological descriptions (2000).
Results: Mean of carotid atherosclerosis was 11.5\?0.71, in coronary it was 37.33\?7.57, in aorta the mean we found was 27\?9. The mean of renal artery atherosclerosis was 2.75\?0.71. The association of carotid atherosclerosis with coronary, aorta and renal arteries was statistically significant (p < 0.05).
Conclusion: In present study we conclude that if carotid atherosclerosis is present, patient will be having coronary, aortic atherosclerosis but patient might have renal atherosclerosis. If carotid atherosclerosis is absent it doesn't mean that patient won't be having atherosclerosis in any other vessels.
Keywords: Atherosclerosis, Autopsy, Carotid artery
Full Text:
INTRODUCTION
Atherosclerosis is a major cause of morbidity and mortality worldwide and it account for one third of all deaths from heart disease.[1] The most serious outcome of atherosclerosis are stroke, myocardial infarction and death. [2] Autopsy is a tool of real value rather than an exercise of tradition, when done selectively and efficiently. [2] Autopsy series are often quoted as an unbiased information source. [3] As study of atherosclerosis in the living population is difficult in many ways including its cost-effectiveness, autopsy studies have been regarded as one good way of dealing with the problem. [4] Given the limited ability of current clinical imaging methods to visualize the vessel wall, as opposed to the lumen, we are highly dependent on autopsy material for describing various different stages of atherosclerosis. [5] Atherosclerosis is a generalized vascular disease. [6] Although there is asymmetry in involvement of various arteries in atherosclerosis but the disease usually proceeds in parallel in various organ system in our body. [3] Once the disease apparent in one territory, there is increased risk of adverse events in the vascular territories including those supplying the brain, kidneys, mesentery, and limbs. [8] Atherosclerosis has the distinctive topographical distribution in the intimal surface of each artery of various organs.[7] Hypothesis which explain the difference in atherosclerotic lesions in every organ are hemodynamic stresses related to arterial geometry; anatomic, cellular or biochemical variation in arterial wall, particularly in the endothelium, smooth muscle cell mutations leading to monoclonal proliferation and infectious agent. [7] Atherosclerosis affects the Indian population at a younger age than in any other ethnic groups with more severe and extensive angiographic involvement. [8] By imaging technique only few superficial vessels like carotid can be studied for the atherosclerosis. [9] Sever al radiological studies show that carotid intima media thickness can be regarded as an indicator of generalized atherosclerosis which can predict the future cardiovascular and cerebrovascular events. [9, 10] Radiological studies had shown that there is close association of carotid atherosclerosis with aortic and coronary artery atherosclerosis. [9] Several studies done angiographically had shown that renal artery atherosclerosis usually exits as one manifestation of generalized atherosclerosis. [11] So it is very important to see whether the extent of disease correlates in different arterial beds same as in carotid artery or not. [12] Till now none of the radiological or autopsy study had correlated carotid atherosclerosis with coronary aorta and renal atherosclerosis. So here the study had been conducted, to see whether the carotid atherosclerosis can be correlated with the atherosclerosis of other major vessels using gold standard technique of histomorphological analysis on the autopsy specimens. So that carotid atherosclerosis can be used as a screening tool to predict the future cardiovascular, cerebrovascular and kidney disease. This is to help to start early intervention for these diseases and thus decreases the disease burden.
MATERIAL AND METHODS
Patient selection
The study was descriptive, cross sectional done on the autopsy cases in which patient died without morphological evidence of atherosclerotic catastrophe, during the period of January 2011 to August 2013.
Histological preparation: Specimen of heart and the whole length of aorta along with carotids, upto the bifurcation of common carotid artery and the renal arteries was removed and fixed in 10% formalin. The heart was dissected by inflow outflow technique, along the direction of flow of blood and aorta along the posterior surface. The three major coronary arteries were identified and cut transversely at 0.5 cm intervals until their entry into the musculature. Bits from the suspicious or definite atherosclerotic lesions were taken. All arteries were processed by routine tissue processing and stain with hematoxylin and eosin stain.
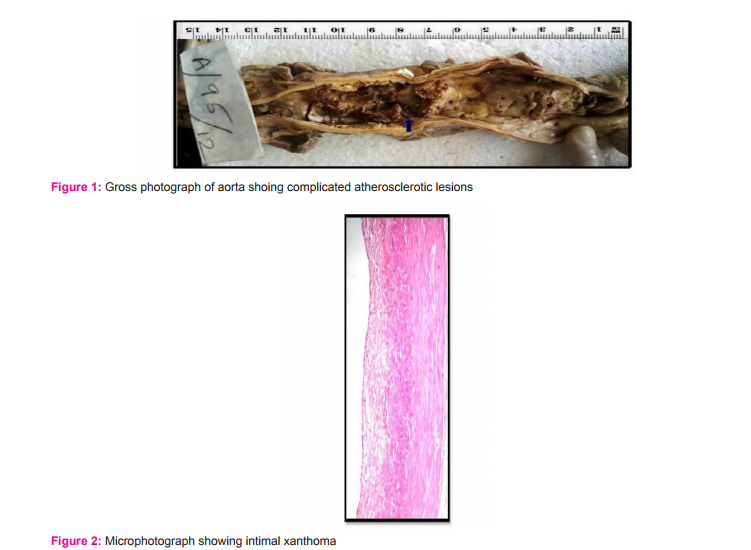
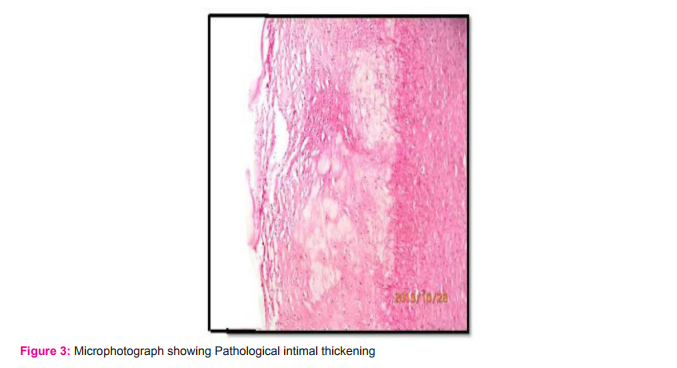
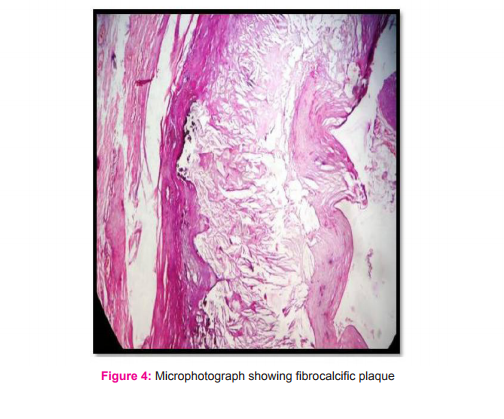
Pathological Assessment and Morphological Analysis: The microscopic grading of atherosclerosis was done according to the modified American Heart Association Classification(AHA) of atherosclerosis using morphological descriptions (2000) which is better than the earlier AHA classification with regard to the description of intermediate lesions which was prone for future development of complicated atherosclerosis.[5] The atherosclerotic lesions were divided into non-atheromatous lesions (Intimal thickening and Intimal Xanthoma) and progressive atheromatous lesions like [Pathological intimal thickening (PIT), Thick Fibrous cap atheroma (FCA) and Thin fibrous cap atheroma (TFCA), Calcified nodule (CN) and Fibrocalcific plaque (FCP)]. (Figure-2,3,4)
Statistical Analysis: Statistical analysis was done using chi square test using SPSS software.
RESULTS
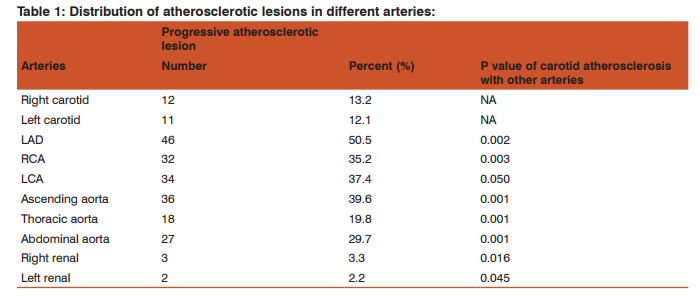
In the present study, the ages ranged from 7 to 72 years and mean age were 39.23±14.24 years. Number of males and female were 67(74%) and 24 (26%) respectively. The most common cause of death was road traffic Accidents 42(46.1%), followed by poisoning 21(23.1%), then hanging and burns 5(5.5%) each. For comparing the atherosclerosis between the arteries, we have divided our results into two broad category i.e Non atherosclerotic lesion (NAL) and progressive atherosclerotic lesion (PAL) which was given in the classification because most NAL has potential to regress.[7] In present study, the atherosclerosis(which has PAL) in carotid was 12.6%. In case of coronaries atherosclerosis in LAD is about 51% followed by RCA 35% and last LCA was 37%. Atherosclerosis was 40% in ascending aorta, 20% in thoracic aorta and 30% in the abdominal aorta Atherosclerosis in renal arteries was only 3 %.The number and percent of PAL in all arteries was given in the (Table-1) When comparing the association of significance of atherosclerosis in carotid with coronaries, aorta and renal arteries, the P value was < 0.05, which was statistically significant.
DISCUSSION
Atherosclerosis is generalized systemic disease, affected by multiple risk factors such as age, gender, race, smoking, personality, hyperlipidemia etc. Atherosclerosis usually proceeds in parallel in various organ systems but there is asymmetry in involvement of various arteries by this disease. [3] The reason may be that the magnitude of the effect of each risk factor varies among the arterial beds for example- smoking selective augments abdominal aorta and thoracic more commonly affect the younger age group. [7] Many earlier studies had mention that carotid intima media thickness can be regarded as an indicator of generalized atherosclerosis. [9, 10] So it is very important to see whether the extent of disease cor-relates in different arterial beds same as in carotid artery or not. [12]
Association between carotid and coronary atherosclerosis: In the present, study mean of carotid atherosclerosis was 11.5±0.71 (12.6%) and mean of coronary atherosclerosis was 37.33±7.57 (41%). Nazarat et al had reported 50% and 85% of carotid and coronary atherosclerosis respectively. [14] Most Indian studies has shown steep rise in coronary atherosclerosis after second decade of life. [13] Advanced lesion in the coronary artery start appearing as early as in third decade. [15] In present study the none of the patient less than 34 years had carotid atherosclerosis. Prati et al. also reported none of the carotid atherosclerosis in less than 30 years. [16] Both above studies show that carotid atherosclerosis may start appearing after fourth decade compare to coronary which show steep rise after second decade. It was observed in our study that the coronary arteries were invariably involved showing atherosclerosis when carotid artery was affected and the percentage distribution of both arteries being involved when carotid artery showed atherosclerotic changes was 100%. The association between two arteries was statically significant.
Association between carotid and aortic atherosclerosis: The mean of aortic atherosclerosis was 27±9(29.9%) which was higher compared to the carotid atherosclerosis which was observed in this study. Earliest age of aortic atherosclerosis was observed is 20 year, whereas earliest age of carotid atherosclerosis was observed at 40 years. Siraj Ahmed et al had observed earliest aortic atherosclerosis in the second decade. [17] When carotid had atherosclerotic lesion 100% of patient had aortic involvement and most frequently associated with the ascending and abdominal aorta. Kallikazaros et al had found74.3% of incidence of carotid plaque in the subgroup with aortic plaque.[18] and also found that absence of carotid plaque may not reflect the absence of aortic plaque. [18] The association between the two arteries were statically significant.
Association between carotid and renal artery atherosclerosis: The mean of renal artery atherosclerosis was 2.75 ± 0.71(2.7%) which was much lower compared to the carotid atherosclerosis observed in our study. Only 25% of cases of carotid atherosclerosis had renal atherosclerosis. The difference may be due to the prevalence of renal artery atherosclerosis was much lower than the carotid atherosclerosis. Kuroda et al had reported 22.8% patient with carotid atherosclerosis had renal atherosclerosis. [11] Aggarwal et al reported advanced lesion like fibrous plaque was rarely observed before fifth decade. [19] When atherosclerosis presents in renal artery all (100%) the cases also had carotid atherosclerosis. It had been seen that 45%-100% of patient with renal atherosclerosis had co-morbid carotid artery atherosclerosis. [11] Studies had shown that severe carotid atherosclerosis associated with renal atherosclerosis and also the chronic kidney disease. [20] The wide difference in atherosclerotic lesions between the present study and other studies might be due to the fact that they have used the earlier AHA classification which considered even grade I and II lesions as atherosclerosis. In the present study since we have used the modified AHA classification of atherosclerosis, the earliest lesions like intimal thickening and intimal xanthoma were not considered as atherosclerotic lesions, partly explaining the difference in the prevelance of atherosclerosis. From above discussion we conclude that if carotid atherosclerosis is present, patient will be having coronary, aortic atherosclerosis but patient might have renal atherosclerosis. If carotid atherosclerosis is absent it doesn’t mean that patient won’t be having atherosclerosis in any other vessels.
CONCLUSION
From above study we conclude that carotid atherosclerosis is the indicator of generalized atherosclerosis. Assessing the carotid atherosclerosis using non-invasive technique can be used as screening tool for cardiovascular, cereberovascular and kidney disease due to renal artery atherosclerosis. The use anti-atherogenic preventive measures may be implemented as soon as carotid atherosclerosis is detected. So as to prevent premature death caused by cardiovascular, cereberovascular and kidney disease, burdening the national economy.
ACKNOWLEDGEMENT
The authors would like to thank Mr Ravishankar for statistical analysis and lab technicians from Histopathology division for processing the samples for this study. Authors acknowledge the immense help received from scholars whose article are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publisher of all those articles, journals and books from where the literature for the article has been reviewed and discussed.
References:
1. Shah PK. Screening asymptomatic subjects for subclinical atherosclerosis: can we, does it matter, and should we? J Am Coll Cardiol. 2010;56:98–105.
2. Fausto N. Atherosclerosis in young people. Am J Pathol 1998;153:4.
3. Zoccali C, Mallamaci F, Finocchiaro P. Atherosclerotic renal artery stenosis: epidemiology, cardiovascular outcomes, and clinical prediction rules. J Am Soc Nephrol2002; 13: S179–83.
4. Naher S, Naushaba H, Muktadir G, Rahman MA, Khatun S, Begum M. Percentage area of intimal surface of the abdominal aorta affected by atherosclerosis: A postmortem study. J Med Sci Res 2007; 9 (1):26-30.
5. Virmani R, Kolodgie FD, Burke AP, Farb A, Schwartz SM. Lessons From Sudden Coronary Death: A Comprehensive Morphological Classification Scheme for Atherosclerotic Lesions. Arterioscler Thromb Vasc Biol 2000;20:1262- 1275.
6. Prince MR. Is there replacement for percentage stenosis in characterizing occlusive vascular disease? Radiology. 2007;245(3):617-8
7. McGill HC Jr, McManhan CA, Herderick EE, Tracy RE, Malcom GT, Zieske AW, et al. Effects of coronary heart disease risk factors on atherosclerosis of selected regions of the aorta and right coronary artery. PDAY Research Group. Pathobiological Determinants of Atherosclerosis in Youth. Arterioscler Thromb Vasc Biol. 2000;20:836–45.
8. Faxon DP, Creager MA, Smith SC, Jr, et al. Atherosclerotic Vascular Disease Conference: Executive summary: Atherosclerotic Vascular Disease Conference proceeding for healthcare professionals from a special writing group of the American Heart Association. Circulation. 2004;109:2595– 2604.
9. Bots ML, Hoes AW, Koudstaal PJ, Hofman A, Grobbee DE. Common carotid intima-media thickness and risk of stroke and myocardial infarction: the Rotterdam Study. Circulation. 1997;5(5):1432–1437.
10. Mattace-Raso F, van Popele NM, Schalekamp MA, van der Cammen TJ. Intima-media thickness of the common carotid arteries is related to coronary atherosclerosis and left ventricular hypertrophy in older adults. Angiology. 2002;53(5):569–74
11. Kuroda S, Nishida N, Uzu T, Takeji M, Nishimura M, Fujii T et al. Prevalence of renal artery stenosis in autopsy patients with stroke. Stroke. 2000;31:61–65
12. Finn AV, Kolodgie FD, Virmani R. Correlation between carotid intimal/medial thickness and atherosclerosis: a point of view from pathology. Arterioscler Thromb Vasc Biol. 2010;30:177–181
13. Singh H, Oberoi SS, Gorea RK, Bal MS. Atherosclerosis in coronaries in Malwa region of Punjab. J Indian Acad Forencis Med. 2005;27(4):236-239
14. Nezarat N, Sadeghi M, Rabiel K, Afshar Moghadam N , Satareh M, Ezadinezhad M, et al The effect of body fat distribution on coronary and carotid atherosclerosis: an autopsy study. J Res Med Sci. 2012;17(Spec 1):S125-S130.
15. Keche AS, Tirpude BH, Bobade HJ. Progressive atherosclerosis in central India – A modern epidemic. Al Ameen J Med Sci. 2013;6(4):342-349.
16. Prati P, Vanuzzo D, Casaroli M, Di Chiara A, De Biasi F, Feruglio GA, Touboul PJ. Prevalence and determinants of carotid atherosclerosis in a general population. Stroke. 1992;23:1705–1711.
17. Ahmed S, Prabhu MH, begum A. Atherosclerosis of aortaan autopsy study. J Biomed Pharm Res. 2013;2(5):52-58.
18. Kallikazaros IE, Tsioufis CP, Stefanadis CI, Pitsavos CE, Toutouzas PK. Closed relation between carotid and ascending aortic atherosclerosis in cardiac patients. Circulation.2 000;102:III263–268
19. Aggarwal A, Kapoor K, Singh B. Prevalence and severity of atherosclerosis in renal artery in Northwest Indian population: an autopsy study. Surg Rad Anat. 2009;31(5):349- 346.
20. Iwakiri T, Sato Y, Matsuura Y, Hatakeyama K, Marutsuka K, Yasashit A, et al. Association between renal vasculature changes and generalized atherosclerosis: An autopsy survey. J Atheroscler Thromb. 2014;21(2):99-107
Abbreviations:
LAD - Left anterior descending artery
RCA – Right coronary artery
LCA – Left circumflex coronary artery
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





