IJCRR - 7(10), May, 2015
Pages: 25-34
Print Article
Download XML Download PDF
RETROSPECTIVE ANALYSIS OF REASONS FOR PRE DONATION DEFERRAL - A SUCCESSFUL KEY TO MODIFY BLOOD DONOR RECRUITMENT STRATEGIES
Author: Sonam Kumari
Category: General Sciences
Abstract:Background: To make blood collection, processing and transfusion safe for the patients as well as the donors and blood bank staff, many safety measures are undertaken, and the most important of which is the selection of suitable blood donors. Moreover, the knowledge of rate and causes of donor deferral can guide the recruitment strategy for whole blood donation. Objectives: To analyse the incidence and reasons for deferrals and to apply relevant findings to modify recruitment strategy for blood donors. Materials and Methods: Data for whole blood donorspresenting for donation in our blood centre and outdoor blood donation camps over three years were analyzed retrospectively. National guidelines were used for selection and deferral of whole blood donors. Results: 895 (5.61%) donors were deferred. Among them 790 (4.95%) were voluntary donors and 105 (0.65%) were replacement donors. Majority 534 (59.7%) of the donors deferred were between 18 \? 30 years. Temporary deferrals were 791(88.37%) and permanent deferrals were 104 (11.6%). Among temporary deferrals, themost common causes were medical (400 i.e 44.7%) causes followed by anemia (163 i.e. 18.2%). Among permanentdeferrals, the most common cause was Jaundice (34 i.e. 3.8%). Conclusion: Donor counselling to improve the return rate of temporary deferrals and strict donor selection criteria should be implemented with more proactive measures to make blood donation a safe and pleasurable experience.
Keywords: Donor deferral, Temporary, Permanent, Anemia, Underweight, High risk donors
Full Text:
INTRODUCTION
A huge number of blood donors are not able todonate blood successfully for several reasons, either temporarily or permanently. The donors are deferred/ rejected for several reasons related to the safety of the donor and the potential threat to the recipient and the blood bank staff. Donor (Blood Donor) is a person who, after complete medical examination by the doctor, is declared fit for donation of blood. Individualsdisqualified from donating blood are known as ‘deferred’ donors.[1] Deferring prospective donors often leaves them with negative feelings about themselves as well as the blood donation process. Additionally these donors are less likely to return for blood donation in future. Criteria for these deferrals and their implementation strongly influence the quality of blood supply. Thus, every blood transfusion centre has to balance the fulcrum between acceptable quality and desired quantity.[2] A few studies from India in the past have provided different common reasons for deferralof whole blood donation highlighting differing demographic profile in different parts of thecountry.[3]Most of the efforts at government, community (various organizations like religious, political or societies) and individual levels are focused at recruiting more and more new donors while ignoring the retention and re-entry of those recruited but deferred due to various temporary causes. Retention and re-entry of these temporarily deferred donors can be achieved by analyzing the reasons of their deferrals and ameliorating the causes wherever possible.
AIM
The present study was undertaken to analyze the deferral incidence and pattern among blood donors and to apply relevant findings to modify recruitment strategy for blood donors.
MATERIALS AND METHODS
The study was conducted at Department of Transfusion Medicine, Gian Sagar Medical College and Hospital, Patiala, India during the period from January 2012 to December 2014.The study involved donors who had donated blood at outdoor voluntary blood donation camps and at the blood bank. Donors were selected by Medical officer. Information regarding the donor deferral was recorded. Each donor was examined by MedicalOfficer based on detailed medical history and brief physical examination as per the criteria laiddown by the Drugs and Cosmetic Act 1940 (and rules there under) supplemented by the Technical Manual (Directorate General of Health Services, Ministry of Health and Family Welfare, Govt. of India) and the Departmental Standard Operating Procedures. [4]Detailed informationof the deferred donors including the age, sex, cause of deferral whether temporary or permanentwere recorded. The quantity of blood collected was 350ml from donors who weighed> 45 kg and450 ml from donors who weighed >60 kg. All the donors were screened clinically for anemia and those found anemic or borderline anemic were tested for haemoglobin estimation (Hb%) by DIASPECT Hemoglobinometer and the cut-off value was 12.5g/dl. Pulse rate between 60 – 100/ minute with adequate volume and without any irregularity was accepted. Donors with systolic blood pressure (BP) between 100 and 160 mm of Hg and diastolic BP between 60-100 mm of Hg were accepted for blood donation.An average of three measurements were taken for those not falling within this range of systolic or diastolic BP. Detailed information on the donor deferral including the cause of deferral were recorded in the donor questionnaire cum consent form and the donor record register. Temporarily deferred donors during that period were counselled regarding the importance of blood donation, and they were informed that they could be recruited for blood donation after removal of the cause. Deferral reasons were analysed amongst replacementvoluntary, male-female, occupation and various age group categories. Donors were categorized into five conventional age group categories for analysis.
STATISTICAL ANALYSIS
Computer Software SPSS programme was used to analyse the data. All the datawere compiled, tabulated and analysed
RESULTS
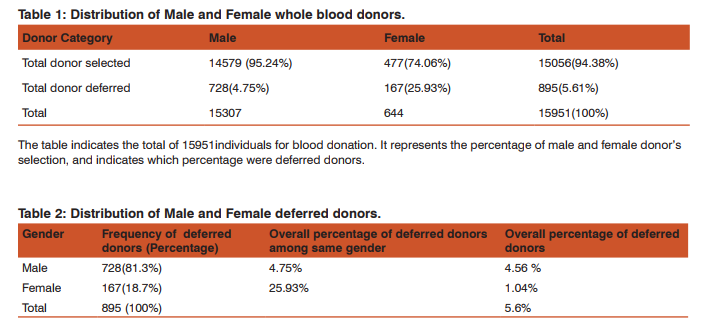
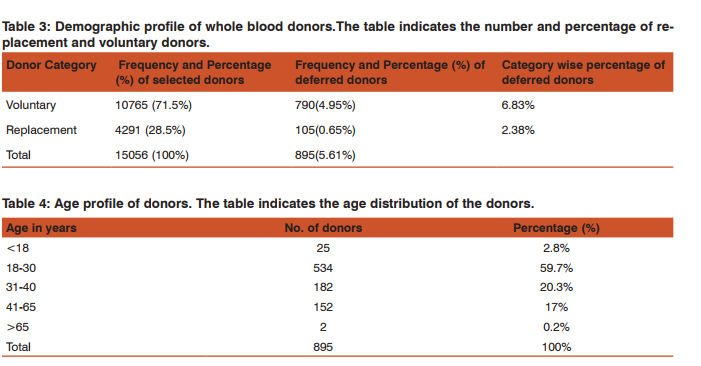
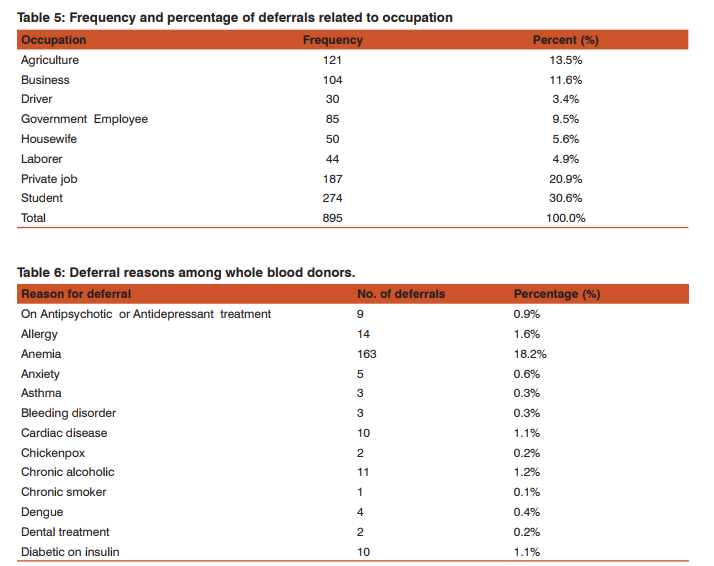
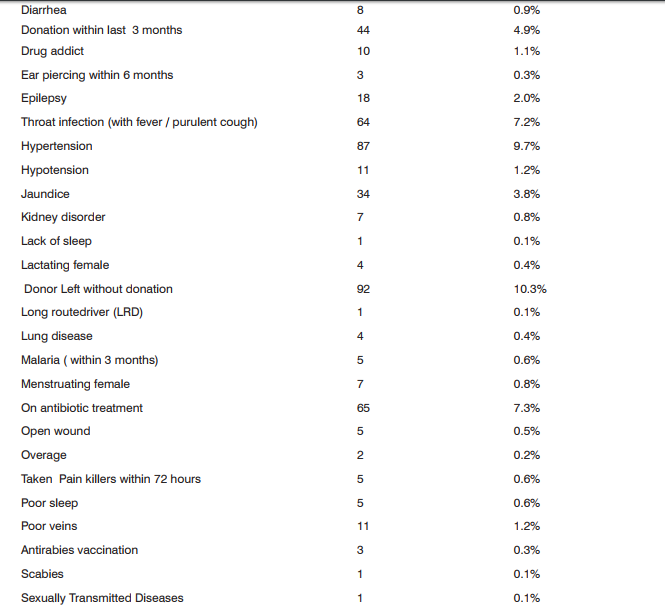
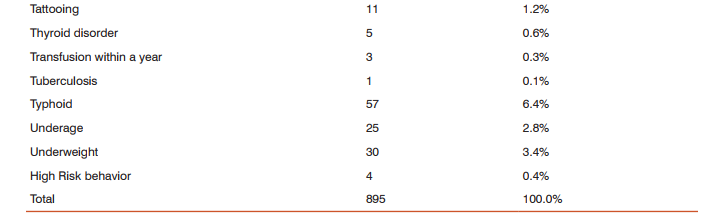
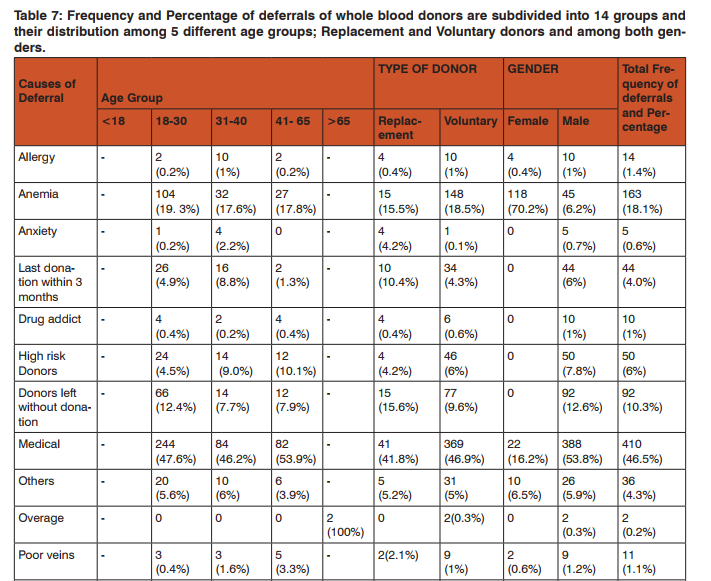
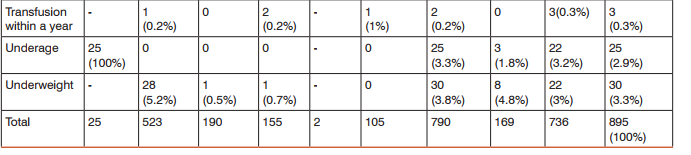
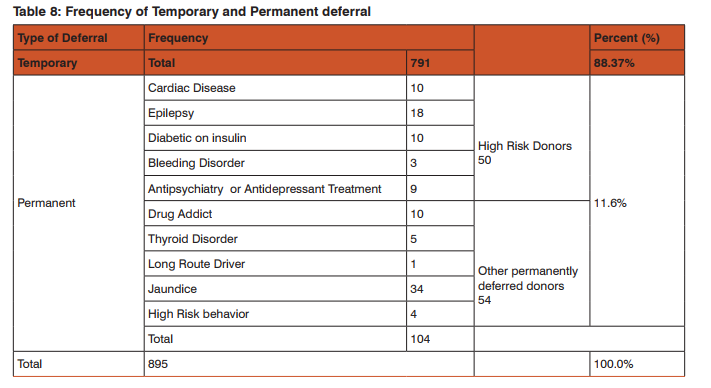
During the study period total 15,951 donors were screened out of which 15056 (94.38%)were accepted both in the outdoor voluntary blood donation camps and at the blood bank. Of the total donors who were willing for blood donation, 895 (5.61%) donors were deferred.Total Male donors screened were15307 (95.9%) and female were 644 (4.03%) out of which 728(4.75%) males and 167(25.93%) females were deferred [Table 1]. Among the total 895(5.61%) deferred donors, 728(81.3%) were male and 167(18.7%) were female while gender wise 4.75% males25.93% females were deferred [Table 2]. Out of total 11,555 voluntary donors (VD), 790 (6.83%) were deferred and out of 4396 replacement donors (RD), 105 (2.38%) were deferred. Out of 5.61% deferred donors, 4.95% were voluntary and 0.65% were replacement donors[Table 3]. Age category was divided into 5 groups i.e. 65 years. Majorityi.e. 534 (59.7%) of the donors deferred were between 18 – 30 years of age followed by 182 (20.3%) in 30 – 40 years age group. 27 donors were not eligible for blood donation i.e. 25 of them were underage 65 years of age [Table 4]. Donor Population were divided into 8 groups on the basis of occupation as shown in [Table 5] and the most common group of deferred donors was of students 274 (30.6%) followed by those doing private job 187 (20.9%). One of these 8 groups was of drivers (local and long route drivers) 30(3.4%). Most common cause of deferral among drivers was medical (17) including hypertension (8) followed by Chronic alcoholic or some drug abuse (like opium addiction) (10). Precise detail of causes of deferrals among blood donors was shown in [Table 6] with total number and percentage of each while for convenience and statistical analysis, these causes were divided into 14 groups shown in [Table 7]. Most common causes of deferral were Medical 410 (45.8%) causes followed by anemia 163 (18.2%), donors who left without donation 92 (10.3%) and High risk donors 50 (5.8%). Medical causes of deferral included hypertension, Jaundice, fever, cough, typhoid, malaria, antibiotics or medication intake, dental treatment, diarrhoea, ,chickenpox, surgery, open wound, kidney disease, lung disease, hypotension, dengue, thyroid disorder and allergy. High risk group included those donors with high risk of donation related adverse events and it consists of cardiac disease, epilepsy, diabetic on insulin, antidepressant or antipsychiatry treatment and bleeding disorders. ‘Others’ category of deferral included chronic alcoholic, chronic smoker, ear piercing or tattooing, menstruating or lactating woman, lack of sleep, antirabies vaccination and transfusion within a year. Medical causes were the most common causes of deferral among 18 – 30, 31 – 40, 41 -65 years age group i.e. 244(47.6%), 84(46.2%) and 82(53.9%) respectively followed by anemia i.e. 104(19. 3%), 32(17.6%) and 27(17.8%) respectively. Donors left without blood donation were more among the younger population of 18 – 30 years age group i.e. 66 (12.4%). [Table 7]. Medical causes are the most common causes of deferral among both voluntaryand replacement donors. All the reasons of deferral are more common among voluntary donors except for anxiety which is more common among replacement donors i.e. 4 out of 5[Table 7]. Donor deferrals were tabulated into temporary and permanent as shown in [Table8].Causes of Permanent deferral included high risk group, drug addicts, jaundice, thyroid disorder, long route driver and high risk behaviour. Temporary deferrals were 791(88.37%) and permanent deferrals were 104 (11.6%). Among males, the mostcommon causes of temporary deferral were medical causes i.e. 388 (53.8%) followed by donors who left without donation 92(12.6%)and anemia 45(6.2%). In females, anemia118 (70.2%) was the most common cause fortemporary deferral followed by medical causes 22(16.2%)[Table 7]. Among Medical causes, the most common causes for deferral were hypertension 87 (9.7%), on antibiotic treatment 65(7.3%), throat infection 64 (7.2%) and typhoid within 1 year 57 (6.4%). The most common cause of permanent deferral among males wasJaundice 34 (3.8%). All the donors falling in High risk group 50(7.8%) were also deferred permanently. In females, thyroid disorder (4 out of 5 donors) was the common cause for permanent deferral.
DISCUSSION
Deferring unfit donors is the preliminary step towards safety of the blood donor and the recipient. There are definitive advantages of eliminating donors with possible risk of transfusion transmissible disease because, despite the availability of sensitive screening tests to detect these infections, blood donors can be infected, but tests are negative if they donated in the window period.[5] The rate and reasons of deferral differs from region to region and from one centre to other. Donor deferral rates in regional blood centres vary from 5 to 24 per cent and a less restrictive criteria can be used for donor selection without compromising donor safety.[6,7] Knowledge of deferral incidence and causes in a particular region helps in deciding the magnitude and direction of blood donor recruitment efforts. This knowledge also helps in calculating the eligible and potential blood donor pool. The eligible donor pool may drastically vary from the potential donor pool which is usually calculated on the basis of age alone. This fact was highlighted by William Riley and colleagues in their study where they showed that the conventional method of determining eligible donors, using age alone as the criteria, overestimated eligible donor prevalence by approximately 59 percent![8] In our study, we segregated donor deferrals on the basis of medical interview and general physical examination. Most of the donors were males 15307 (95.9%) and women accounted for only 644 (4.03%) of the donors. In studies from other countries,following deferral rates were reported 12.8% by Zou et al(2008), 14.4% by Lim et al (1993) and 13.6% by Custer et al (2004).[7,9,10] From Indian Literature, deferral rate were observed as Sundar et al. (6%), Chaudhary etal. (16.4%), Bahaduret al. (9%) and Sharma et al. (5.1%).[3,11,12,13] Deferral incidence varies among donor population, which reflects the regional diversity and variation in whole blood donor eligibility criteria internationally. In present study donor deferral rate was5.61% which was similar to that of Sundar et al and Sharma et al. The donor deferral rate can be reduced by educating the donors and providing information about the selection criteria which will result in better acceptability and there by less negative feeling about rejection and it will further enhance the future donor return rate. The most common cause of temporary deferrals in females wasanemia118 (70.2%). Among males, the most common cause of deferral was medical cause i.e. 388 (53.8%). A number of other studies showed anemia as the most common cause like Agnihothri N, 56%, Arslan et al 20.7%, Halperin et al 46%[2,14,15]. Similarly, in present study anemia was the most common cause of deferral 163 (18.2%) when all the causes of deferral were considered independently followed by medical causes like hypertension 87 (9.7%), antibiotic treatment 65(7.3%) and typhoid within 1 year 57 (6.4%). In anotherIndian study by Chaudhary et al. low weight (32.3%) and low haemoglobin (18.6%) were the twomost common reasons for deferral.[11]The relationship between haematocrit deferral rates and temperature is strongest in areas of the country with greater temperature variability, with the lowest values occurring in the summer. The effect of seasonality on Hematocrit deferrals should be taken into account for donor counselling, recruitment, and retention efforts.[20]In a study from Trinidad and Tobago, a history of high-risk sexual activity was the most common cause of deferral [16]while in present study history of high risk behaviour could be elicited only in 4 donors (0.4%) which could be due to the tendency of people to hide such information (as high risk sexual activity is considered a social taboo in Indian society). Analysis of the deferrals showed that the top ten defined causes were Anemia 163(18.2%), Donors who left with-out donation 92 (10.3%), Hypertension 87 (9.7%), Antibiotic treatment within 72 hours 65 (7.3%), Throat infection 64 (7.2%), Typhoid 57 (6.4%), Donation within last 3 months 44 (4.9%), History of Jaundice 34 (3.8%), Underweight 30 (3.4%) and Surgery within 6 months 22 (2.5%) which accounts for 73.7% of the total deferrals. A large number of deferrals due to pulse irregularities or histories suggestive of potential cardiovascular problems were reported by Blumberg et al, [19] whereas in our study 10 (1.1%) donors had known cardiac disease or symptoms suggestive of cardiovascular problems and were deferred permanently. Incidence of donors with poor veins with minimal possibility of successful phlebotomy was 11 (1.2%). These donors were deferred as trials of phlebotomy in such donors results in incomplete collections, multiple punctures, painful and unpleasant experience resulting in negative impact on such donors as well as the colleague donors.Rate of unsuccessful phlebotomy due to poor vein, double puncture, collecting less quantity were reported as 0.5% by Farrales and 0.006% by Sunder. [17,3 ] Loss of blood units due to miscollection (underweight or overweight) or poor phlebotomy are common. Such losses can be avoided by implicating trained and vigilant blood bank staff and this would further supplement the blood supply. In addition to deferral, age, sex, race, and education were associated with return of deferred donors.[21]Silvergleid et al donor attitude survey indicated 90% donor approval of direct questioning, and analysis of donor deferral patterns indicated almost a five-fold increase in the number of donors deferred for participation in high-risk activities indicating that such questioning could have a positive impact on blood safety.[22,16]Given that Human Immuno deficiency Virus (HIV) antibody screening cannot detect HIV-seronegative (but infectious) “windowperiod” donations, the deferral of at-risk donors may offer some additional protection to the blood supply.[23]In present study, 30(3.4%) of deferred donors were drivers (local and long route drivers). Since drivers were considered to be comparatively more indulged in high risk activities, causes of deferral among drivers were analysed and most common of them were medical (17) including hypertension (8) followed by chronic alcoholic or some drug abuse (like opium addiction) (10). It strengthens the fact that occupation should also be considered while analysing donor deferral patterns.The most common group of deferred donors was of students 274 (30.6%) which forms the major chunk of the eligible and potential donors. It further supports the need for donor retention and counselling as they are the most receptive part of the society and can be easily retained. Of these deferred students, 25 (2.8%) were underage; they can be made aware of their eligibility period so that they can return for donation. In our study 104 (11.6%) of donors were deferred for permanent reasons which was similar to Custer et al (2004) and Arslan (2007) who reported a permanent deferral rate of 10.6% and 10% respectively. [10,14] Two Indian studies from Chandigarh and Lucknow reported that history of jaundice was the most common cause of deferral[18,11] whereas in present study jaundice was the most common cause of permanent deferral. In females, thyroid disorder (4 out of 5 donors) was the common cause for permanent deferral. Permanently deferred donors were segregated into High risk group (50) and others (54). This high risk group consisted of donors with (high risk of donation related adverse events) cardiac disease, epilepsy, diabetic on insulin, antidepressant or antipsychiatry treatment and bleeding disorders. In the study done by Charles et al, in Trinidad and Tobago, the difference in rate of deferral amongst voluntary and replacement donors was not significant[16]while in present study, out of 5.61% deferred donors, 4.95% were voluntary and 0.65% were replacement donors which was quite significant. It is due to the fact that we had recruited more and more voluntary donors in our blood donation programmes. The incidence of all kind of deferrals was more common among voluntary donors except for deferral due to anxiety (4 out of 5) which might be due to the fact that replacement donors were forced for donation, they were not mentally prepared for donation. Donors who had donated blood within last three months comprised of 44 (4.9%) of the total deferrals. These were the donors who need not to be motivated; they should be properly guided for their eligible period so that they can return for donation regularly. According toRios JA et al, deferral of donors with low Estimated blood volume who are less than 23 years old may offer a rational approach to protecting donors at greater risk of reactions without jeopardizing the adequacy of the blood supply while Halperin D et al study showed that selective deferral of donors with low blood volume have a very negative impact on blood donor return rates and subsequent blood donations. [24,15]So, it is very important to counsel the donors who are selectively deferred for reasons like low estimated blood volume. Pindick et al concluded that it is both clinically feasible and efficient to recruit healthy prior donors older than the age of 65 years for blood donation.[25] 2 donors in present study were deferred due to age >65 years who were willing to donate and otherwise normal clinically but were not accepted. It indicates the need for formulation of a strategy to recruit such donors to improve the donor pool. The objective during donor selection should be blood collection as well as donor safety. Safety of donors is important as it helps in gaining confidence and winning the trust of future donors as well.[26]Information Education and Communication (IEC) material providing information and education on causes and duration of deferral may “prime” prospective donors about possibility of deferral. Any such sensitization beforehand results in better acceptability of “rejection” and thereby less “negative” feeling about blood donation and more chances of future return. In addition, medical examination (Hemoglobin, blood pressure, pulse rate) serves as an incentive for future repeat donations. The category of temporary deferral influences the likelihood of future return, but the demographic and donation factors associated with return are largely consistent.[27] Sawanpanyalert et al proposed adonor deferral system providing a more flexible, sensitive, and predictive tool for averting donation by those who, though HIV antibody-negative, are at a higher risk of being infected with HIV.[5] Donor self-deferral is valid for reducing the risk of HIV transmission through blood transfusions, and its implementation should be encouraged, when recruiting blood donors. [28,29] In present study, a special category of deferral was of donors who got enrolled themselves but left the donation area without donating blood which constituted 92 (10.3%) of the total deferrals. The probable reasons of such self- deferral might be the peer - pressure, long waiting periods, fear or anxiety or lack of confidence or indulgence in high risk behavioural activity. This kind of selfdeferralfurther needs to be investigated to improve the donor pool. Wherever varying staff in the deferral process - doctors, nurses and clerks - were involved, analysis and audits should be undertaken for medical donor deferrals.[30,19] Education, motivation, and treatment of these deferred donors due to anemia or other temporary deferrals are important aspects in blood banking and hence that these donors can be recruited again.[31] The entire blood bank staff, especially medical officers, should share the responsibility of winning the confidence of donors and making blood donation a safe and pleasurable experience which will eventually increase voluntary blood donation, giving a permanent remedy to the shortage of blood in the country.[26]
CONCLUSION
Analysis of rejection patterns may help medical personnel to be more focused in donor screening. Temporary donor deferrals need to be actively and aggressively managed especially medical causes (fever, throat infections, and typhoid), anemia, underage, underweight and donors who enrol themselves but don’t donate blood. This will not only help in maintaining a healthy donor pool but will also help in improving donor and recipient safety in the long run, provided the potential donors are appropriately counselled.[12]By developing strategies to identify and rationalize donor selection criteria, the blood transfusion services would be able to decrease the unnecessary deferrals.[11]
ACKNOWLEDGEMENT
The author acknowledges the immense help received from the scholars whose articles are cited and included in the references of this manuscript. The author is also grateful to the authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of Funding No funding from any source received for this work.
Conflict of Interest No conflict of interest involved in this study.
References:
1. Kulkarni N. Analysis of donor deferral in blood donors. Journal of Evolution of Medical and Dental Sciences 2012; 1: 1076-1082.
2. Agnihotri N. Whole blood donor deferral analysis at a center in Western India. Asian J Transfus Sci.2010; 4(2):116- 122.
3. Sundar P, Sangeetha SK, Seema DM, Marimuthu P, Shivanna N. Pre-donation deferral of blood donors in South Indian set-up: An analysis. Asian J Transfus Sci.2010; 4(2):112- 115.
4. Department of AIDS Control Ministry of Health and Family Welfare Government of India.Annualreport:2008-2009. Availablefrom: http://nacoonline.org/upload/Publication/ Annual Report NACO 2008-09.PDF.
5. Sawanpanyalert P, Uthaivoravit W, Yanai H, Limpakarnjanarat K, Mastro TD and Nelson KE. Donation deferral criteria for human immunodeficiency virus positivity among blood donors in northern Thailand. Transfusion 1996; 36: 242-249.
6. Tomasulo PA, Anderson AJ, Paluso MB, Gutschenritter MA andAster RH. A study of criteria for blood donor deferral. Transfusion 1980; 20(5):511-8.
7. Zou S, Musavi F,Notari EP, Rios JA, Trend JT and Fang CT.Donor deferral and resulting donor loss at the American Red Cross Blood Services, 2001 through 2006. Transfusion 2008; 48: 2531-2539.
8. Riley W, Schwei M. and McCullough J. The United States’ potential blood donor pool: estimating the prevalence of donor-exclusion factors on the pool of potential donors. Transfusion 2007; 47: 1180-1188.
9. Lim JC, Tien SL, and Ong YW. Main causes of pre-donation deferral of prospective blood donors in the Singapore Blood Transfusion Service. Annals of the Academy of Medicine, Singapore 1993; 22(3):326-331
10. Custer B., Johnson E S, Sullivan SD, Hazlet T K, Ramsey SD, Hirschler NV, Murphy EL and Busch MP. Quantifyinglosses to the donated blood supply due to donor deferral and miscollection. Transfusion 2004; 44: 1417–1426.
11. Chaudhary RK, Gupta D and Gupta RK. Analysis of donordeferral pattern in a voluntary blood donor population. Transfus Med. 1995; 5: 209-12.
12. Bahadur S, JainS, Goel RK, Pahuja S and Jain M. Analysis of blood donor deferral characteristics in Delhi, India. Southeast Asian J Trop Med Public Health2009; 40(5).
13. Sharma T, Singh B, and BhattGC. Profile of deferral of blood donors in regional blood transfusion enter in North India. Asian J Transfus Sci. 2013; 7(2): 163-164.
14. Arslan O. Whole blood donor deferral rate and characteristics of the Turkish population. Transfus Med 2007; 17:379- 83.
15. Halperin D, Baetens J, Newman B. The effect of short term temporary deferral on future blood donation. Transfusion. 1998; 38:181-183.
16. Charles KS, Hughes P, Gadd R, Bodkyn C J and Rodriguez M. Evaluation of blood donor deferral causes in the Trinidad and Tobago National Blood Transfusion Service. Transfusion Medicine 2010; 20: 11-14.
17. Farrales FB, Stevenson AR and Bayer WL. Causes of disqualification in a volunteer blood donor population. Transfusion. 1997; 17:598-601.
18. Kaur R,Basu S, Marwaha N. A Reappraisal of underlying causes in donor deferral. Ann Natl Acad Med Sci. 2002;38:93-9.
19. Blumberg N, Shah I, Hoagland J, Shirer L and Katz AJ. Evaluation of Individuals Deferred from Blood Donation for Medical Reasons. VoxSanguinis 1982; 42(1): 1-7.
20. Sebok MA, Notari EP, Chambers LA, Benjamin RJ and Eder AF. Seasonal temperature variation and the rate of donor deferral for low hematocrit in the American Red Cross. Transfusion 2007; 47: 890-894.
21. Custer B, Chinn A, Hirschler NV, Busch MP and Murphy EL. The consequences of temporary deferral on future whole blood donation. Transfusion 2007; 47: 1514-1523.
22. Silvergleid AJ, Leparc GF and Schmidt PJ. Impact of explicit questions about high-risk activities on donor attitudes and donor deferral patterns. Results in two community blood centers. Transfusion 1989; 29: 362-364.
23. Johnson ES, Doll LS, Satten GA, Lenes B, Shafer AW, Kamel H, Casanova RJ and Petersen LR. Direct oral questions to blood donors: the impact on screening for human immunodeficiency virus. Transfusion 1994; 34: 769-774.
24. Rios JA, Fang J, Tu Y, Wright D J, Spencer B, Hillyer C D, Hillyer KL, Eder A. F. and Benjamin, R. J. The potential impact of selective donor deferrals based on estimated blood volume on vasovagal reactions and donor deferral rates. Transfusion 2010; 50: 1265-1275.
25. Pindyck J, Avorn J, Kuriyan M, May Reed, Iqbal MJ, Levine SJ. Blood Donation by the Elderly Clinical and Policy Considerations. JAMA. 1987;257(9):1186-1188.
26. Sareen R, Gupta GN, Dutt A.Donor awareness: key to successful voluntary blood donation. F1000Research 2012, 1:29.
27. Custer B, Schlumpf KS, Wright D, Simon TL, Wilkinson S and Ness. Donor return after temporary deferral. Transfusion 2011; 51: 1188-1196.
28. Urwijitaroon Y, Barusrux S, Romphruk A, Puapairoj C and Pakote L. Reducing the risk of HIV transmission through blood transfusion by donor self-deferral. Southeast Asian J Trop Med Public Health 1996;27:452-6.
29. Anderson SA, Yang H, Gallagher LM, O’Callaghan S, Forshee RA, Busch MP, McKenna MT, Williams I, Williams A, Kuehnert MJ, Stramer S, Kleinman S, Epstein J. and Dayton AI. Quantitative estimate of the risks and benefits of possible alternative blood donor deferral strategies for men who have had sex with men. Transfusion 2009; 49: 1102- 1114.
30. Galea G, GillonJ and Urbaniak SJ.Study on medical donor deferrals at sessions Transfusion Medicine 1996; 6: 37–43.
31. Alok K, Satyendra P, Sharma SM, Ingole NS and Gangane N. Impact of counselling on temporarily deferred donor in a tertiary care hospital, central India: A prospective study. Int J Med Public Health 2014;4:400-403.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





