IJCRR - 7(10), May, 2015
Pages: 20-24
Print Article
Download XML Download PDF
CADAVERIC STUDY OF THE EXIT OF SCIATIC NERVE
Author: Shaheen Rizvi, Sharadkumar Pralhad Sawant
Category: General Sciences
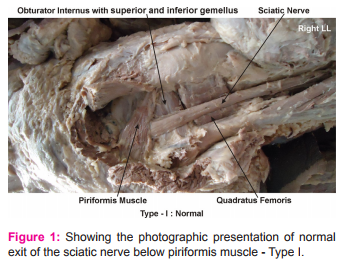
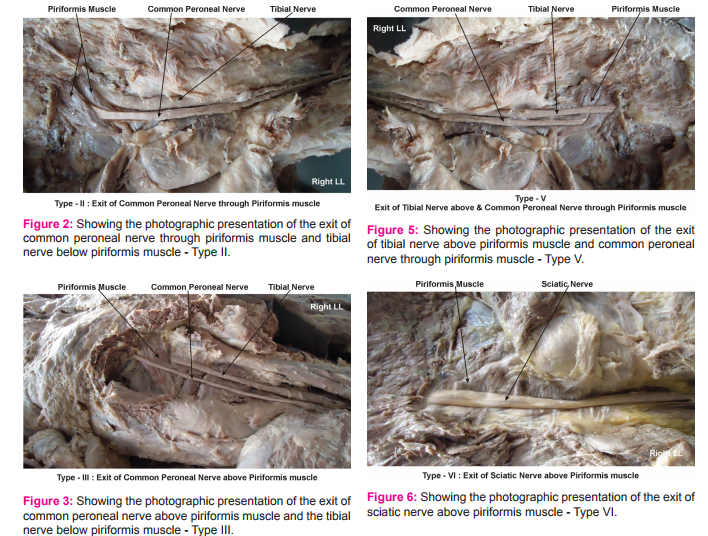
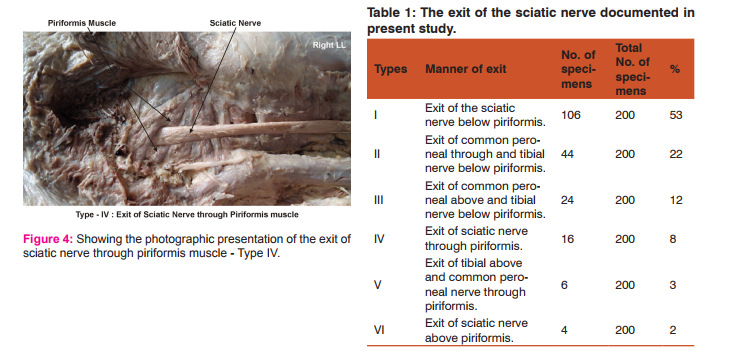
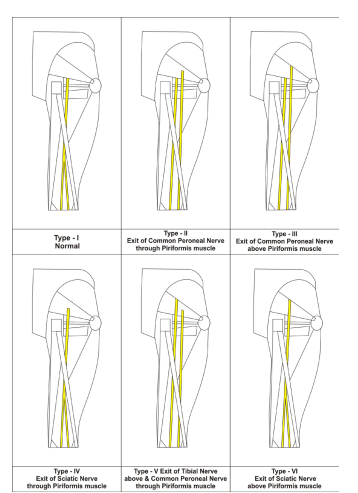
Abstract:Aims: To study the exit of sciatic nerve in 100 cadavers. Materials and Methods: In the department of Anatomy of K.J.Somaiya Medical College, Sion, Mumbai, India, the study on exit of sciatic nerve was performed on 100 (200 specimens of Inferior Extremities) embalmed donated cadavers (80 males and 20 females). The specimens were classified into six groups. Observations: In Type I, 106 (103 males and 3 female) of the 200 (53%) specimens, the exit of the sciatic nerve below piriformis muscle. In Type II, 44 (all males) out of 200 (22%) specimens, the exit of common peroneal nerve through piriformis muscle and the tibial nerve below piriformis muscle. In Type III, 24 (22 males and 2 female) out of 200 (12%) specimens, the exit of common peroneal nerve above piriformis muscle and the tibial nerve below piriformis muscle. In Type IV, 16 (all males) out of 200 (8%) specimens, the exit of sciatic nerve through piriformis muscle. In Type V, 6 (4 males and 2 females) out of 200 (3%) specimens, the exit of tibial nerve above piriformis muscle and common peroneal nerve through piriformis muscle. In Type VI, 4 (all males) out of 200 (2%) specimens, the exit of sciatic nerve above piriformis muscle.
Conclusion: Sciatic nerve division into the tibial and common peroneal components at a higher level can result in the involvement of only one out of the two divisions in sciatic neuropathy. It can also result in a failure of the sciatic nerve block while performing popliteal block anaesthesia. These anatomical variations may contribute to clinical conditions such as piriformis syndrome, sciatica and coccygodynia.
Keywords: Sciatic nerve, Gluteal region, Piriformis, Sciatic nerve block, Piriformis syndrome, Sciatica
Full Text:
INTRODUCTION
The sciatic nerve also known as the ischiadic nerve and the ischiatic nerve is 2 cm wide at its origin and is the thickest nerve in the body. It leaves the pelvis via the greater sciatic foramen below piriformis and descends between the greater trochanter and ischial tuberosity, along the back of the thigh, dividing into the tibial and common peroneal nerves at a varying level proximal to the knee. Superiorly it lies deep to the gluteus maximus, resting first on the posterior ischial surface with the nerve to quadratus femoris between them. It then crosses posterior to obturator internus, the gemelli and quadratus femoris, separated by the latter from obturator externus and the hip joint. It is accompanied medially by the posterior femoral cutaneous nerve and the inferior gluteal artery. More distally it lies behind the adductor magnus and is crossed posteriorly by the long head of the biceps femoris. It corresponds to a line drawn from just medial to the midpoint between the ischial tuberosity and greater trochanter to the apex of the popliteal fossa. Articular branches arise proximally to supply the hip joint through its posterior capsule, these are sometimes derived directly from the sacral plexus. Muscular branches are distributed to biceps femoris, semitendinosus, semimembranosus and the ischial part of adductor magnus. The point of division of the sciatic nerve into its major components (tibial and common peroneal) is very variable. The common site is at the junction of the middle and lower thirds of the thigh, near the apex of the popliteal fossa. The division may occur at any level above this, though rarely below it. It is not uncommon for the major components to leave the sacral plexus separately, in which case the common peroneal component usually passes through piriformis at the greater sciatic notch while the tibial component passes below the muscle (1). The sciatic nerve supplies the knee flexors and all the muscles below the knee, so that a complete palsy of the sciatic nerve results in a flail foot and severe difficulty in walking. This is rare and usually related to trauma. The nerve is vulnerable in the posterior dislocation of the hip. As it leaves the pelvis it passes either behind piriformis or sometimes through the muscle and at that point it may become entrapped (the piriformis syndrome; this is a common anatomical variant but an extremely rare entrapment neuropathy). External compression over the buttock (e.g. in patients who lie immobile on a hard surface for a considerable length of time) can injure the nerve. The commonest cause of serious sciatic nerve injury is iatrogenic. It may be damaged in misplaced therapeutic injections into gluteus maximus. The safe zone for deep intramuscular injections here is the upper outer quadrant of the buttock. Perhaps safer still is to inject into the quadriceps, though this can produce problems of its own, e.g. haemorrhage, leading to contracture of the muscle, which limits knee movement. Sciatic nerve palsy occurs after total hip replacements or similar sureries in 1% of cases. This can be due to sharp injury, burning from bone cement, traction from instruments, manipulation of the hip, inadvertent lengthening of the femur, or haematoma surrounding the nerve or within its soft tissue coverings. Haematoma is characterised by the development of severe pain in the immediate post operative period. Early surgical exploration and evacuation of haematoma can reverse the nerve lesion. Unfortunately the other causes may not be reversed. The majority are temporary. Complete sciatic nerve palsy is very rare. For some reason, possibly anatomical, the common peroneal part is more usually affected. The patient has a foot drop and a high stepping gait (1). The sciatic nerve bifurcates into two major divisions (tibial and common peroneal), most commonly at the lower part of the posterior compartment of the thigh (1, 2, 3, 4, 5). Several authors have reported variations in its division into the tibial and common peroneal nerve from the sacral plexus to the lower part of the popliteal space (3, 4, 5, 6, 7, 8, 9). These anatomical variations may contribute to piriformis syndrome, sciatica, coccygodynia and muscle atrophy (10). This should be taken into account by clinicians who are planning interventions around the sciatic nerve and its division in the lower extremity (11).
MATERIALS AND METHODS
This study on division of sciatic nerve was performed on 100 (200 specimens of Inferior Extremities) embalmed donated cadavers (80 males and 20 females) in the department of Anatomy of K. J. Somaiya Medical College, Sion, Mumbai, India. To study the exit of the sciatic nerve 200 specimens were classified into six groups. Group A, the exit of the sciatic nerve below piriformis muscle. Group B, the exit of common peroneal nerve through piriformis muscle and the tibial nerve below piriformis muscle. Group C, the exit of common peroneal nerve above piriformis muscle and the tibial nerve below piriformis muscle. Group D, the exit of sciatic nerve through piriformis muscle. Group E, the exit of tibial nerve above piriformis muscle and common peroneal nerve through piriformis muscle and in Group F, the exit of sciatic nerve above piriformis muscle. The photographs were taken for proper documentation.
Observations:
In Type I, 106 (103 males and 3 female) of the 200 (53%) specimens, the exit of the sciatic nerve below piriformis muscle.
In Type II, 44 (all males) out of 200 (22%) specimens, the exit of common peroneal nerve through piriformis muscle and the tibial nerve below piriformis muscle
. In Type III, 24 (22 males and 2 female) out of 200 (12%) specimens, the exit of common peroneal nerve above piriformis muscle and the tibial nerve below piriformis muscle.
In Type IV, 16 (all males) out of 200 (8%) specimens, the exit of sciatic nerve through piriformis muscle.
In Type V, 6 (4 males and 2 females) out of 200 (3%) specimens, the exit of tibial nerve above piriformis muscle and common peroneal nerve through piriformis muscle.
In Type VI, 4 (all males) out of 200 (2%) specimens, the exit of sciatic nerve above piriformis muscle.
DISCUSSION
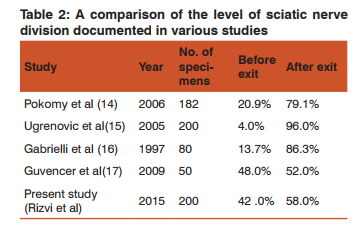
During embryological development at the base of the limb bud, the nerves contributing to the lower limb forms two plexuses lumbar and sacral (12). Later, as the elements from each of these plexuses grow out into the limb, they are subdivided into the dorsal and ventral components, for the dorsal and ventral musculatures (13). The sciatic nerve is formed when the large dorsal component of the sacral plexus, common fibular nerve and the ventral component, tibial nerve move downward close together (13). Hence, based on their previously mentioned developmental formation, it is possible that the common fibular and the tibial divisions of the sciatic nerve separate from each other at different levels from their origins; in the gluteal region, the posterior compartment of the thigh or the popliteal fossa, as observed in this study. Various studies have reported on the level of sciatic nerve division into tibial and common peroneal nerves (Table 2). The incidence of sciatic nerve division before its exit in the gluteal region in our study was 42%, which was higher than that found in a study conducted by Pokorny et al (20.9%), Ugrenovic et al (4.0%) and Gabrielli et al (13.7%) (14, 15, 16). Guvençer et al (17) examined 50 gluteal regions in 25 cadavers and observed that in 52% of the cases, the sciatic nerve exited the pelvis as a whole nerve without any division, whereas in 48% of the cases, a high division of sciatic nerve was recorded (Table 2).
Saleh et al studied the level of division of the sciatic nerve into the tibial nerve and common peroneal nerve above the knee in 30 cadavers, and reported that the sciatic nerve divided at a distance of 50–180 mm above the popliteal fossa crease (13). Suresh et al recorded the measurements from the magnetic resonance images of 59 patients and proposed a formula for determining the point of bifurcation of the sciatic nerve in the posterior thigh using a linear regression model (18). Acute sciatic neuropathies commonly result from hip arthroplasty, hip fracture or dislocation. On the other hand, causes such as coma, which result in prolonged compression, are relatively rare (2).
The extent of involvement and neurological deficits vary depending on the level of division of the sciatic nerve. A high division of the sciatic nerve into the tibial and common peroneal nerves can result in the escape of either the tibial or the common peroneal nerve from one of the aforementioned causes, which would finally result in a decrease in neurological deficits as compared to the low division of the sciatic nerve. One important consequence of the high division of the sciatic nerve that has been reported by various authors is that it may lead to failure of popliteal block anaesthesia (19, 20).
Clinical significance
A high division of the sciatic nerve into the tibial and common peroneal nerves can result in the escape of either the tibial or the common peroneal nerve, which would finally result in a decrease in neurological deficits as compared to the low division of the sciatic nerve. One important consequence of the high division of the Sciatic Nerve is that it may lead to the failure of popliteal block anaesthesia.
CONCLUSION
The awareness of the variant exit of the sciatic nerve is clinically important for surgeons dealing with entrapment or compressive neuropathies, orthopaedicians operating on the fractures of femur, anaesthetist performing pain management therapies on the lower limb and physiotherapist doing electromyography for evaluating and recording the electrical activity produced by skeletal muscles. A lack of knowledge of such type of variations might complicate surgical repair.
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
SR drafted the manuscript, performed the literature review and SPS assisted with writing the paper.
ACKNOWLEDGEMENT
Authors are thankful to Dean Dr. Geeta Niyogi Madam for her support and encouragement. Authors are also thankful to Mr. M. Murugan for his help. Authors also acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Standring S. Gray’s Anatomy: the Anatomical Basis of Clinical Practice. 39th ed. London: Churchill Livingstone, 2005, pp 1364-1458.
2. Yuen E.C., So Y.T., Sciatic neuropathy, Neurological Clinic 1999, Vol. 17, pp 617-631.
3. Paval J., Nayak S., A case of bilateral high division of sciatic nerve with a variant inferior gluteal nerve, Neuroanatomy, 2006, Vol. 5, pp 33-4.
4. Rosse C., Gaddum-Rosse P., Hollinshead W. H., Hollinshead’s Textbook of Anatomy, 5th ed. Philadelphia: Lippincott-Raven Publishers, 1997, pp 324-651.
5. Moore K. L., Dalley A. F., Clinically Oriented Anatomy, 4th ed. Philadelphia: Lippincott Williams and Wilkins, 1999, pp 347-560.
6. Ndiaye A., Sakho Y., Fall F., Dia A., Sow M.L., Sciatic nerve in gluteal portion: application of sciatic nerve post injection lesion, Morphologie 2004, Vol. 88, pp 135-138.
7. Arifoglu Y., Surucu H.S., Sargon M.F., Tanyeli E., Yazar F., Double superior gemellus together with double piriformis and high division of the sciatic nerve, Surgical Radiological Anatomy, 1997, Vol. 19, pp 407-8.
8. Valade N., Ripart J., Nouvellon E. et al., Does sciatic parasacral injection spread to the obturator nerve? An anatomic study. Anesth. Analg. 2008, Vol. 106, pp 664-7.
9. Benzon H. T., Katz J. A., Benzon H. A., Iqbal M. S., Piriformis syndrome: anatomic considerations, a new injection technique, and a review of the literature, Anaesthesiology 2003, Vol. 98, pp 1442-8.
10. Schwemmer U., Markus C.K., Greim C.A. et al., Sonographic imaging of the sciatic nerve and its division in the popliteal fossa in children. Paediatric Anaesthesiology 2004, Vol. 14, pp 1005-1008.
11. Babinski M. A, Machado F. A., Costa W. S., A rare variation in the high division of the sciatic nerve surrounding the superior gemellus muscle. Europian Journal of Morphology 2003, Vol. 41, pp 41-2.
12. Demiryurek D., Bayramoglu A., Erbil M., Aldur M. M., Mustafa E. S., Bilateral divided piriformis muscle together with the high division of the sciatic nerve. Gazi Medical Journal 2002, Vol. 13, pp 41-4.
13. Saleh H. A., El-fark M. M., Abdel-Hamid G. A., Anatomical variation of sciatic nerve division in the popliteal fossa and its implication in popliteal nerve block, Folia Morphol (Warsz) 2009, Vol. 68, pp 256-259.
14. Pokorny D., Jahoda D., Veigl D., Pinskerova V., Sosna A., Topographic variations of the relationship of the sciatic nerve and the piriformis muscle and its relevance to palsy after total hip arthroplasty, Surgical Radiological Anatomy 2006, Vol. 28, pp 88-91.
15. Ugrenovic S., Jovanovic I., Krstic V. et al., The level of the sciatic nerve division and its relations to the piriform muscle. Vojnosanit Pregl 2005, Vol. 62, pp 45-49.
16. Gabrielli C., Olave E., Mandiola E. et al., Inferior gluteal nerve course associated to the high division of the sciatic nerve. Rev. Chil. Anat. 1997, Vol. 15, pp 79-83.
17. Güvençer M., Iyem C., Akyer P., Tetik S., Naderi S., Variations in the high division of the sciatic nerve and relationship between the sciatic nerve and the piriformis, Turk Neurosurgery 2009, Vol. 19, pp 139-44.
18. Suresh S., Simion C., Wyers M. et al. Anatomical location of the bifurcation of the sciatic nerve in the posterior thigh in infants and children: a formula derived from MRI imaging for nerve localization, Reg. Anesth. Pain Med 2007, Vol. 32, pp 351-353.
19. Vloka J. D., Hadzic A., April E., Thys D. M., The division of the sciatic nerve in the popliteal fossa: anatomical implications for popliteal nerve blockade. Anesth Analg 2001, Vol. 92, pp 215-7.
20. Nayak S., An unusual case of trifurcation of the sciatic nerve, Neuroanatomy 2008, Vol. 5, pp 6-7.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





