IJCRR - 7(10), May, 2015
Pages: 01-05
Print Article
Download XML Download PDF
AMELOBLASTIC FIBRO SARCOMA OF THE MANDIBLE IN A YOUNG MALE
Author: Balasubramanian A., N. S. Kannan
Category: General Sciences
Abstract:Aim: Aim of this study is to report a rare case of Ameloblastic Fibro Sarcoma (AFS) of mandible arising as a denovo malignancy and to review the literature with reference to so far reported cases, nomenclature, classification, differential diagnosis and management. Case report: A 14 year old male patient presented with complaints of a painless swelling of left side of the face since 1 year. Based on clinical presentation and investigation reports it was diagnosed as a case of AFS in left side of mandible arising as a denovo malignancy. He underwent left hemimandibulectomy 'en bloc' with part of the adjacent masseter and pterygoid muscles under general anaesthesia. Discussion: Ameloblastic Fibro Sarcoma (AFS) is one of the rare histopathology variety of odontogenic tumours. The first case of AFS was reported in 1887 by Heath. Since then only 91 cases have so far been reported. This number includes both denovo and sarcomatous transformation from pre-existing ameloblastic fibroma, occurring in different sites. The most common site affected is mandible [78%]. The mean age of patients with tumours arising denovo is 22.9 years. Ours is a case of AFS arising as a denovo malignancy in left side of mandible. Conclusion: We are presenting our case due to rarity and the limited information that exists regarding histopathology characteristics of AFS, lack of defined criteria for grading and biologic behaviour of these tumours, making the diagnosis eluding, treatment decision challenging and assessment of prognosis difficult.
Keywords: Odontogenic tumours, Denovo malignancy, Orthopantomogram, Hemimandibulectomy ‘en bloc’
Full Text:
INTRODUCTION
Ameloblastic Fibro Sarcoma (AFS) is one of the rare histopathology variety of odontogenic tumours. The first case of Ameloblastic Fibro Sarcoma (AFS) was reported in 1887 by Heath. Since then only 91 cases have so far been reported in literature. This number includes both denovo and sarcomatous transformation from pre existing ameloblastic fibroma, occurring in different sites. The most common site affected is mandible [78%]. The mean age of patients with tumours arising denovo is 22.9 years. Biopsy is required for preoperative diagnosis. The management of AFS should be wide surgical excision with surrounding soft tissue especially if there is cortical disruption as in our case, due to its propensity for high local recurrence. We report a rare case of Ameloblastic Fibro Sarcoma (AFS) in left side of mandible in a 14 year male, arising as a denovo malignancy and the literature is reviewed with reference to so far reported cases, nomenclature, classification, differential diagnosis and management.
CASE DETAILS
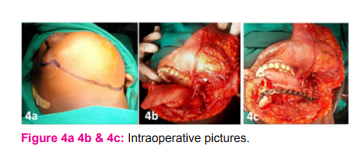
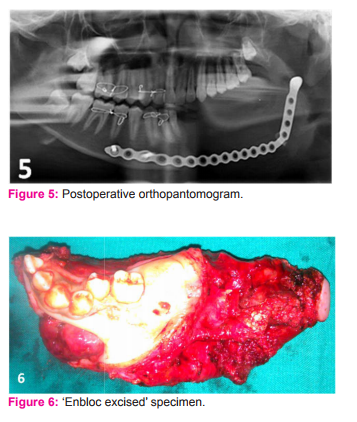
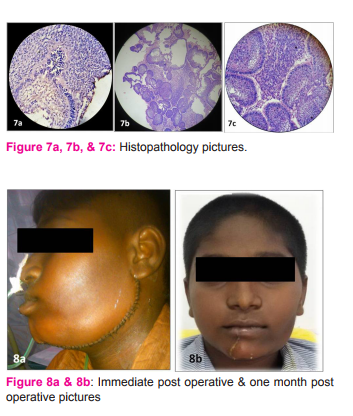
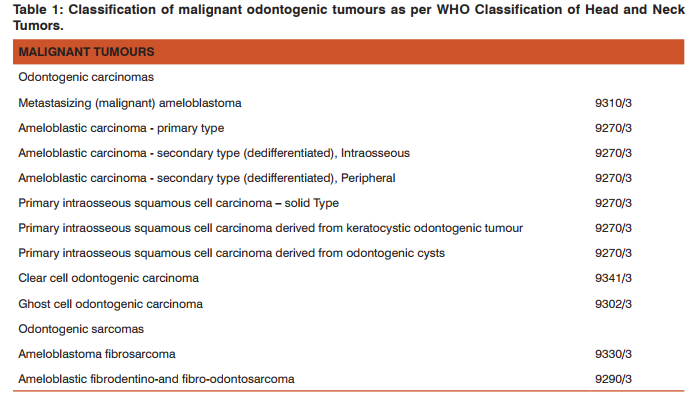
A 14 year old male patient presented in outpatient department with complaints of a painless swelling of left side of the face since 1 year (Figure 1a and 1b). Clinical examination revealed a swelling of 12 x 10cm involving the left side of the mandible with firm to hard consistency. Overlying skin appeared normal. On intraoral examination, the swelling was extending from the region of left lower canine tooth to the retro molar region and with lingual version of canine and premolars, medially displaced second premolar, loosening of first molar and missing left lower second molar tooth. There was no cervical lymphadenopathy. Orthopantomogram (Figure 2) showed expansile lytic lesion involving the left side of the mandible extending from the area beneath the root of the left lower canine, posteriorly up to the condyle with resorption of roots of both the premolars, fracture of the 1st molar tooth, missing of second molar tooth and grossly displaced unerupted third molar tooth. Contrast Enhanced Computerised Tomography (CECT) of head and neck showed circumferential cortical expansion with thinning of the cortex and areas of cortical disruption involving the horizontal ramus, coronoid process and ascending ramus up to the condyle on the left side of the mandible (Figure 3a 3b and 3c). Other routine investigations were within normal limits. Incision biopsy revealed features of Ameloblastic Fibro Sarcoma. The case was posted for surgery and under general anaesthesia, left hemimandibulectomy ‘en bloc’ with part of the adjacent masseter and pterygoid muscles was done (Figure 4a 4b and 4c). Left lower jaw reconstruction was done with titanium plate. Post operative orthopantomogram is shown in (Figure 5). Postoperative period was uneventful and specimen (Table/Fig 6) sent for histopathology (Figure 7a, 7b and 7c) was reported as Ameloblastic Fibro Sarcoma with negative resection margins. Immunohistochemistry for Vimentin marker was positive. Immediate post operative picture is shown in (Figure 8a). Picture at one month follow up was aesthetically satisfying (Figure 8b). On one year follow up, the patient was hale and healthy and no recurrence so far. He is still under continuous follow up.
DISCUSSION
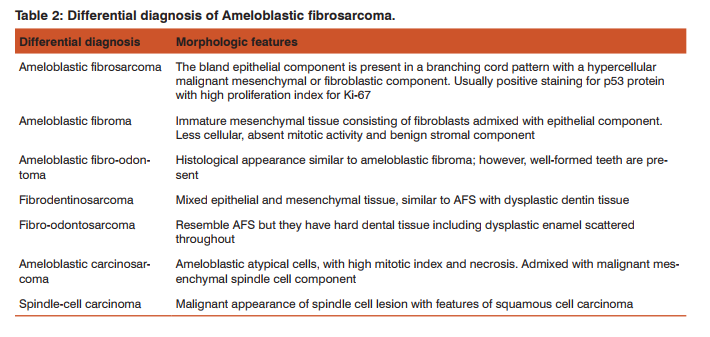
The first case of Ameloblastic Fibro Sarcoma (AFS) was reported in 1887 by Heath1 . So far, only 91 cases have been reported in the literature2-4. AFS is a rare mixed malignant odontogenic tumour composed of benign epithelial component and malignant ectomesenchymal component5 .Classification of malignant odontogenic sarcomas includes other odontogenic sarcomas, specifically two closely related entities that have similar histological features as AFS, ameloblastic fibrodentinosarcoma and fibro-odontosarcoma; These sarcomas have similar morphologic features of AFS; however, in addition they either have dysplastic dentin (fibro-dentinosarcoma) and/ or enamel and dentin (fibro-odontosarcoma) a feature not seen in AFS6,7. These tumours can arise either denovo8 constituting two thirds or as sarcomatous transformation of pre-existing ameloblastic fibroma forming remaining one third9 . They commonly occur in young adults, usually in third decade with a wide age range from 4 months to 89 years reported in the literature and have male predilection4,6-9. The mean age of patients with tumours arising denovo is 22.9 years and is 33 years for those derived from ameloblastic fibroma10. The age of our patient is below the mean age i.e. 14 years. The most common sites affected include mandible [78%], followed by maxilla [20%] and rarely skull base. Moreover, tumours affecting maxilla and mandible tend to occur more in the posterior aspect11. Using the term odontome for any tumour arising from the dental formative tissues, Broca12 suggested a classification of odontogenic tumours (OTs) in 1869. Since then it has undergone many modifications until 1966, when WHO established a Collaborating Centre for the Histological Classification of Odontogenic Tumours and Allied Lesions (including jaw cysts) headed by Dr Jens Pindborg13. In 1971, the first authoritative WHO guide to the classification of OTs and cysts appeared, followed in 1992 by a second edition. In 2002, Philipsen and Reichart produced a revision of the 1992-edition and in 2003, the editors of the WHO Blue Book series: ‘WHO Classification of Tumours’ decided to produce a volume on the Head and Neck Tumours including a chapter on Odontogenic Tumours and Bone Related Lesions. In July of 2005, this volume was published by International Agency for Research on Cancer (IARC), Lyon. Mosqueda-Taylor, in his article have concluded: ‘The lack of uniform criteria employed for their proper identification, as well as the histomorphologic similitude found among some of them which behaves in different way, and the scantiness of proper methods to determine their precise origin makes necessary to recognize that at present, in spite of having more or less strict diagnostic criteria which have been internationally accepted, there is a need to continue developing research in the epidemiological, clinico-pathological, morpho-physiological and therapeutical fields in this area of the maxillofacial pathology’14. Still many new findings and controversies are on the offing regarding odontogenic tumours and their classification14. Classification of malignant odontogenic tumours as per WHO Classification of Head and Neck Tumours is reproduced here for ready reference (Table 1)6 . Differential diagnosis of Ameloblastic fibro sarcoma. (Reproduced from WHO Classification of Head and Neck Tumours) is shown in (Table 2)6 . The natural history of these tumours is characterised by only local aggressiveness contributing to high rate of local recurrence with little propensity for regional and distant metastases. So far, in the literature, only one case had been reported to have metastases to mediastinum and liver. It is because of this behaviour these tumours are categorised as low to intermediate grade malignancy. The gross appearance of these tumours is fleshy with white to yellowish cut surface. Microscopically epithelial component resembles follicular ameloblastoma where the cells have palisading arrangement. These epithelial islands are separated by ectomesenchymal stroma, which forms the bulk of the tumour. Stroma is hyper cellular with polygonal to fusiform cells revealing cellular atypia and increased mitosis8,10. The common clinical features include swelling and pain. They can also present with mucosal ulceration, loosening of teeth and paraesthesia. Radiologically these tumours present as expansile radiolucent lesion with indistinct margins. Biopsy is required for preoperative diagnosis and it is often difficult to diagnose these tumours in preexisting ameloblastic fibromas wherein focal area of malignant degeneration is often missed in biopsies. In such instances, serial sectioning of the surgical specimen is mandatory to establish appropriate diagnosis. The management of AFS should be wide surgical excision with surrounding soft tissue especially if there is cortical disruption as in our case, due to its propensity for high local recurrence rate14. In mandibular AFS, it often results in segmental or hemimandibulectomy. The reconstructive options for resulting defects include mandibular reconstruction with plates or osteocutaneous free flaps. Some authors have recommended adjuvant chemotherapy and radiotherapy but their role is uncertain due to paucity of data in the literature. Radiotherapy may be of use in margin positive resections to decrease the local recurrence rate.
CONCLUSION
To conclude AFS are rare tumours and a high index of suspicion is needed before proceeding to dental extraction since these patients often present with dental pain. So far, only 91 cases have been reported in the literature. This number includes both denovo and sarcomatous transformation from pre existing ameloblastic fibroma, occurring in different sites. AFS of mandible as denovo malignancy below mean age group so far reported, continues to be a rare entity. All patients with ameloblastic fibroma treated by local excision/conservatively should be kept under close surveillance for detecting recurrence/malignant transformation, which may turn out to be AFS. These cases require to be treated by wide surgical resection en bloc with removal of surrounding tissue if tumour has perforated cortical plates. The rarity of AFS and the limited information that exists regarding histopathology characteristics, lack of defined criteria for grading and biologic behaviour of these tumours makes not only the diagnosis challenging and the treatment decision and assessment of prognosis difficult. Presentation of our case report may add up for further research.
ACKNOWLEDGMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
Source of funding: Nil
Conflict of interest: Authors declare that they do not have any conflict of interest.

References:
1. Heath C. Lectures on certain disease of the jaws. Br Med J. 1887;2:5–13.
2. Hu YY, Deng MH, Yuan LL, Niu YM. Ameloblastic fibrosarcoma of the mandible: A case report and mini review. Exp Ther Med. 2014;8(5): 1463–6.
3. Pontes HA, Pontes FS, Silva BS, Cury SE, Fonseca FP, Salim RA, et al. Immunoexpression of Ki67, proliferative cell nuclear antigen, and Bcl-2 proteins in a case of ameloblastic fibrosarcoma. Ann Diagn Pathol. 2010;14(6):447–52.
4. Demoor-Goldschmidt C, Minard-Colin V, Cassagneau E, Supiot S, Oberlin O, D’hautuille C, et al. Ameloblastic fibrosarcoma of the mandible: report of 2 chemosensitive pediatric cases. J Pediatr Hematol Oncol. 2012;34(2):e72–6.
5. Dallera P, Bertoni F, Marchetti C, Bacchini P, Campobassi A. Ameloblastic fibrosarcoma of the jaw: report of five cases. J Craniomaxillofac Surg. 1994;22(6):349–54.
6. Barnes, L.; Eveson, J.; Reichart, P.; Sidransky, D. WHO Classification of Head and Neck Tumors Pathology and Genetics of Head and Neck Tumours; IARC Press: Lyon, France, 2005; pp. 283-328.
7. Gilani S M, Raza A, Al-Khafaji B M. Ameloblastic fibrosarcoma: A rare malignant odontogenic tumor European Annals of Otorhinolaryngology, Head and Neck Diseases. 2014;131(1):53–56.
8. Zabolinejad N, Hiradfar M, Anvari K, Razavi AS. Ameloblastic fibrosarcoma of the maxillary sinus in an infant: a case report with long-term follow-up. J Pediatr Surg. 2008;43:e5–e8.
9. Kobayashi K, Murakami R, Fujii T, Hirano A. Malignant transformation of ameloblastic fibroma to ameloblastic fibrosarcoma: case report and review of the literature. J Craniomaxillofac Surg. 2005;33(5):352–55.
10. Bregni RC, Taylor AM, García AM. Ameloblastic fibrosarcoma of the mandible: report of two cases and review of the literature. J Oral Pathol Med. 2001;30(5):316– 20.
11. Khalili M, Shakib P A. Ameloblastic fibrosarcoma of the upper jaw: Report of a rare case with long-term follow-up. Dent Res J (Isfahan).2013;10(1):112–5.
12. Broca P. Recherches sur un nuveau grupe des tumeurs désignées sousle nom d’odontomes. Gaz Hebd Sci Med. 1868;5:70-84 (Research on a new group of tumors designated under the name odontomas by Mr. Paul Broca, ... [1867 Edition]).
13. Pindborg JJ, Kramer IRH. Histological Typing of Odontogenic Tumours, Jaw Cysts and Allied Lesions. 11th ed. Geneva: World Health Organization; 1971.
14. Mosqueda-Taylor A. New findings and controversies in odontogenic tumors. Med Oral Pathol Oral Cir Bucal. 2008;13(9):E555-8.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





