IJCRR - 7(11), June, 2015
Pages: 50-52
Print Article
Download XML Download PDF
BONE MARROW STUDY IN PANCYTOPENIA
Author: GOVINDARAJ T., RATHNA S., VENKATRAMAN J.
Category: Healthcare
Abstract:Background: Pancytopenia is defined by reduction of all the three formed elements of blood below the normal reference. 1It represents wide variety of disorders affecting the marrow components. Materials and Methods: The present Bone marrow study was carried out over a period of eight months from June 2013 to Jan 2014. A total of fifty cases with a hematological diagnosis of pancytopenia on peripheral smear were included for the study. Results: Out of 50 cases, 34 were males and 16 were females. Most of the patients were in the age group of 41-60 years (54%). The commonest cause of pancytopenia was megaloblastic anaemia (44%) followed by mixed nutritional anemia(20%), hypersplenism(12%), aplastic anemia(10%), Acute Leukaemia(6%), myelodysplastic syndrome(2%) and uncommon causes like Dengue fever(4%) and Hemolytic anemia(2%). Conclusion: Pancyopenia is a commotn entity and it reflects the underlying pathology. Bone marrow study is an important tool in the diagnosis of cause of pancytopenia to implement appropriate management and therapy
Keywords: Bone marrow aspiration, Pancytopenia, Megaloblastic anemia
Full Text:
INTRODUCTION
Pancytopenia is defined by reduction of all the three formed elements of blood below the normal reference.1 It is a manifestation of wide variety of disorders, which primarily or secondarily affect the bone marrow. The presenting symptoms are often attributable to anemia or thrombocytopenia. Leucopenia is an uncommon initial presentation but poses serious threat to life.2 The mechanisms contributing to pancytopenia include, decrease in haematopoietic cell production, marrow replacement by abnormal cells, suppression of marrow growth and differentiation, ineffective hematopoiesis with cell death, defective cell formation, antibody mediated sequestration or destruction of cells in a hypertrophied and overactive reticuloendothelial system.3 Pancytopenia is a serious hematological problem, the underlying cause of which is diagnosed by bone marrow study. Bone marrow examination is extremely helpful in the evaluation of pancytopenia.4 Since the underlying pathology of pancytopenia determines the management and prognosis of the patient, there is a definite need to study about pancytopenia.
MATERIALS AND METHODS
The present study was carried out over a period of eight months from June 2013 to Jan 2014. During this period a total of fifty patients with pancytopenia were studied. A criterion for pancytopenia is : haemoglobin less than 10 gms/dl, total WBC count less than 4000/cumm, platelet count less than 100000/cumm. Bone marrow aspiration was performed using Salah and Jamshidi needle from the posterior iliac crest.
RESULTS
50 cases of pancytopenia were studied. Out of 50 cases, 34 were males and 16 were females. The male to female ratio was 2.1:1. Most of the patients were in the age group of 41-60 years (54%). Majority (50%) of the patients had hemoglobin ranging from 5.1-7 g%. The total leukocytic count was in the range of 500-4000 cells/ cumm. The range of platelet count varied from 4000- 1,50,000 cells/cumm. The reticulocyte count varied from 0.1-20%. Bone marrow aspirate in the present study of pancytopenia showed the following types of cellularity:
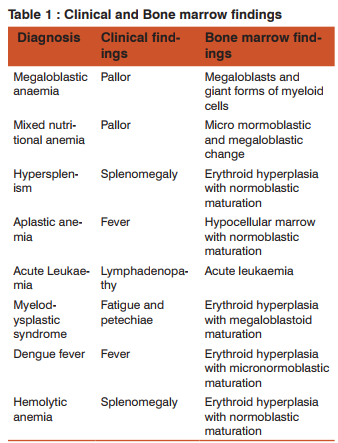
Hypocellularity – 10%, Hypercellularity – 76%, Normocellular – 14%. The commonest cause of pancytopenia was megaloblastic anaemia (44%) followed by combined nutritional anemia(20%), hypersplenism(12%), aplastic anemia(10%), Acute Leukaemia(6%), myelodysplastic syndrome(2%) and uncommon causes like Dengue fever(4%) and Hemolytic anemia(2%) were also encountered.
DISCUSSION
In the present study, megaloblastic anemia(44%) was the commonest cause of pancytopenia followed by combined nutritional deficiency anemia and hypersplenism, in sharp contrast to the present study Hossain MA et al3 observed aplastic anemia was the commonest followed by chronic malaria and kalaazar. Osama5 found megaloblastic anemia (39%) as the commonest cause of pancytopenia followed by hypersplenism (19%) in concurrence to the present study. Megaloblastic anemia is common in india.this seems to reflect the higher prevalence of nutritional anemia .In the study of pancytopenia by Jha et al6 , the age range was 10-79 years(31 years)There was a male preponderance and male to female ratio was 1.5:1.In the present study, age ranged from 18-70 years.There was a male preponderance and the male to female ratio was2.4:1. Aplastic anemia is another frequent cause of pancytopenia. In the study by Jha et al6 , age ranged from 1.5-70 years with male to female ratio of 1.3:1in contrast to the present study where the age ranged from 31-60 years with male to female ratio was 1.5:1. Hypersplenism is known cause of pancytopenia.Kumar et al7 study, age ranged from 41-70 years with male to female ratio being 2:1.In the present study age ranged from 41-70 years with male to female ratio being 2:1. Jha et al6 study revealed leukemia associated with pancytopenia accounted for 19.59% of total cases of pancytopenia and age ranged from 2-75 years with male to female ratio of 1.9:1.In the present study leukemia accounted for 6% of pancytopenia cases and age varied from 21-40 years with male to female ratio being 2:1. Pancytopenia is known to occur in MDS. In a study of 31 patients by Kini J et al8 the patients were in the age group of 4-7 years.In the present study, one case presented with pancytopenia in a female patient aged 55 years. Naeem Khan et al.9 studied 30 cases of pancytopenia and found 1 case of dengue fever. In the present study, 2 cases in 18 years (male) and 22 years (female) with dengue fever presented with pancytopenia. Osama et al.5 in their study found two cases of pancytopenia with hemolytic anemia. In the present study, one patient of hemolytic anemia presented with pancytopenia.
CONCLUSION
Pancytopenia is a common entity. However, it has received inadequate attention in the Indian subcontinent. A study of pancytopenia using easily available diagnostic techniques is therefore important. Age and sex distribution of patients with pancytopenia in this study was consistent with the findings in other studies. Megaloblastic anemia was the commonest cause of pancytopenia in the present study. Most other studies have reported aplastic anemia as the commonest cause. This seems to reflect higher prevalence of nutritional anaemia in the Indian subjects. Uncommon etiological factors like dengue fever and hemolytic anemia were identified in this study. A comprehensive clinical and bone marrow study usually helps in identification of the underlying cause. Pancytopenia poses a challenge for the haematologists in searching the accurate diagnosis. Bone marrow examination is extremely helpful in evaluation of pancytopenia.4 The spectrum of disorders primarily or secondarily affecting the bone marrow may manifest with peripheral pancytopenia.10,11,12 Underlying pathology determines the management and prognosis of patients. Hence there is a need to study.
ACKNOWLEDGEMENT
Authors sincerely thank Dr A L Hemalatha, Former Prof and Head, Dept of Pathology, Mysore Medical College, Mysore for her constant support. Authors also acknowledge the immense help received from the scholars who articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Williams DM. Pancytopenia, Aplastic anemia and PureRed cell aplasia In: Wintrobe’s Clinical Hematology, 10th ed. Baltimore: William and Willkins; 1993.1449-1484.
2. Firkin F, Chesterman C, Penington D, Rush B. deGruchy’s Clinical haematology in Medical Practice.5th ed. London: Blackwell Scientific Publications; 1989.119-136, 346-358.
3. Hossain MA,Akond AK,Chowdhary MK.PancytopeniaA study of 50 cases. Bangladesh Journal of Pathology 1992;1:9-12.
4. Khodke K, Marwah S, Buxi G, Yadav RB, Chaturvedi NK. Bone Marrow Examination in Cases of Pancytopenia. JIACM 2001; 2:55-59.
5. Osama I, Baqai Hz, Anwar F, Hussain N. Patterns of pancytopenia in a general medical ward and a proposed diagnostic approach. JAMC 2002;16(1):8-13.
6. Jha A, Sayami G, Adhikari RC, Panta AD, Jha R. Bone Marrow Examination in Cases of Pancytopenia. JNMA 2008 Jan-Mar;47(169):12-7.
7. Kumar R, Kalra SP, Kumar H, Anand AC, Madan H. Pancytopenia – A six year Study. JAPI 2001;49:1078-81.
8. Kini J, Khandilkar UN, Dayal JP. A study of the haematologic spectrum of Myelodysplastic syndrome. India J Pathol Microbiol 2001;44 (1):9-12
9. Naeem Khan M, Ayyub M, Nawaz KH, Naeem Naqi, Hussain T, Shujaat H, et al. Pancytopenia: Clinico-pathological study of 30 cases at Military Hospital, Rawalpindi. Pak J Pathol 2001 Apr-Jun;12 (2):37-41. 1
0. Dodhy MA, Bokhari N, Hayat A. Aetiology of Pancytopenia, A five- year experience. Ann Pak Inst Med Sci 2005 AprJun;1 (2): 92-5.
11. Wintrobe MM Clinical Haematology. 8th ed. Philadiphia; Lea and Febiger 1981: 699-915.
12. Verma N, Dash. Repraissal of underlying pathology in adult patients presenting with pancytopenia. Trop Geog Med 1992; 44: 322-7.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





