IJCRR - 7(11), June, 2015
Pages: 39-43
Print Article
Download XML Download PDF
Understanding the burden of caring people for patients with a stroke in the subacute and chronic phase in
Nepal
Author: Inosha Bimali
Category: Healthcare
Abstract:Purpose: To determine the prevalence of caregiving burden among stroke caregivers in the subacute and chronic phase of stroke in Nepal. Methods: Fifty caregivers of subacute and chronic stroke were included in the study. Participants were asked to complete a caregiver strain index form. Results: Stata /MP 13.0 data analysis and statistical software was used to analyze the data. One sample t-test, two sample ttest and Pearson correlation test were used for the analysis. Level of significance < 0.05 was considered statistically significant with 95% CI. Among the total participants (caregivers) 16% were male and 84% were female. Out of them 72 % were spouse and 28% were daughter-in-law. The mean Caregivers Strain Index score for female caregivers was marginally greater than that for male caregivers. Caregiver burden was found to be significantly high among both subacute (p= 0.0000) and chronic (p= 0.0000) stroke caregivers. Conclusion: Female caregivers were more than male caregivers with overall Caregiver burden found to be significantly high among subacute and chronic stroke caregivers
Keywords: Subacute stroke, Chronic stroke, Caregivers, Caregiver strain index
Full Text:
INTRODUCTION
Stroke is one of the most disabling disorder with the majority of survivors having persistent functional deficits and requiring assistance from professional and informal caregivers.1 The primary caregivers may experience high levels of burden, emotional distress and adverse effects on family relationships.1 Caring for stroke survivors has been burdensome for their informal caregivers.1 A Caregiver is defined as “a person who lives with the patient and is most closely involved in taking care of him/her at home”.2 Caregiving can also be defined as “an unpaid person who helps with the physical care or coping with the disease”.3 The Caregiver is vulnerable to stress and strain as a result of nursing/attending to a patient over a prolonged period of time. Caregiver burden described by Zarit et al “the state resulting from necessary caring tasks or restrictions that cause discomfort for the Caregivers”.4 Caregivers can experience the burden in terms of sleep disturbance, physical strain, financial strain, emotional and behavior instability, etc. In a study of ischemic stroke survivors aged 65 and older, approximately 50% had hemiparesis, 30% needed assistance with walking, 20% were dependent in their ADLs, one-third had depressive symptoms and 26% were placed in nursing homes.5 The degree to which the caregiver’s work is perceived as a burden may differ among societies and cultures. It also depends on various characteristics of the patient as well as the caregiver.2,3 Although there is extensive literature evaluating caregiver burden and benefit in stroke patients in developed countries, there have been few studies conducted in developing countries and none in Nepal. All the studies showed a high level of caregiver strain. A similar situa tion is expected in Nepal because of limited professional and social support. As we cannot rely on assumptions, a study to document caregiver burden in Nepal is needed to estimate the size of the burden and compare it to developed nations and also it could be useful to design prevention strategies in reducing the level of Strain among stroke caregivers in Nepal.
Materials and Methods
The subjects were randomly selected from different hospitals in Kathmandu and Dhulikhel, Nepal from 2013- 2014. Subjects were also included through outpatient’s clinic home visits. Among the 65 participated for screening, 50 fulfilled the inclusion criteria and were included in the study. A written informed consent was obtained from the participants after explaining the study procedure. Ethical approval was obtained from institutional review committee of Kathmandu university school of medical sciences (KUSMS) with the approval number 55/12. The subjects were recruited in the study based on following inclusion and exclusion criteria:

Flow diagram: Subject’s selection and Study methodology
Twenty-five carers who care for patients with a stroke in subacute stage (~6-12 weeks of caregiving) and twenty-five carers who care for patient with a stroke in the chronic stage (~24 weeks of caregiving) were included in the study. The following measures were then obtained: Demographic data like age and gender of the patient and caregivers, relation (patient-caregiver), duration of caregiving. A Self-administered Caregivers Strain Index was then given to the caregivers .14 Caregivers Strain Index is a brief and easily administered screening instrument for the identification of strain. The 13-item Caregivers Strain Index measures common stressors experienced by caregivers. Items are scored yes (1) or no (0) and are summed, with higher scores indicating greater strain. A Caregivers Strain Index score ≥ 7 was considered an indicator of considerable strain.
Data analysis
Stata/MP 13.0 data analysis and statistical software was used to analyze the data. The level of significance <0.05 was considered to be statistically significant with 95% confidence interval. One sample and two sample t-test were used to analyze the caregivers strain among the two groups. Pearson correlation test was used to see the relation between the Caregivers Strain Index score and duration of caregiving and Caregivers Strain Index score and age of the caregivers.
Results
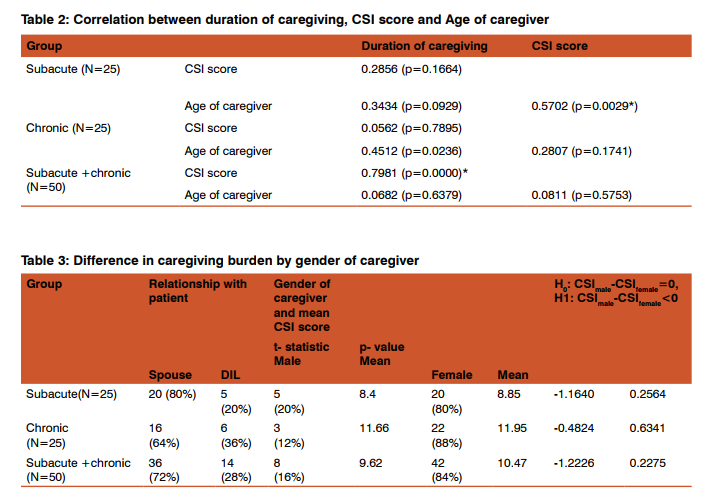
Table 1 gives the mean age of caregiver, mean Caregivers Strain Index score and difference in Caregivers Strain Index score between the caregivers of subacute and chronic stroke patients. The mean age of the caregivers of subacute and chronic stroke patients was 59.84 +7.50 and 57.84+9.28 respectively. The mean Caregivers Strain Index score of caregivers of subacute and chronic stroke patients was 8.76 +0.77 and 11.92 +0.95 respectively. One sample t-test was done to find whether the Caregivers Strain Index score among the subacute, chronic and all caregivers were significantly greater than 7, the cutoff limit of Caregivers Strain Index. Analysis found that the mean Caregivers Strain Index burden for caregivers is high among the caregivers for both types of stroke patients (p=0.0000). Using a two-sample t-test of equality of means, it is also found that the mean Caregivers Strain Index score of chronic caregivers is significantly higher than that of subacute caregivers. In table 2 Pearson’s correlation test was done to identify the correlation between duration of caregiving, Caregivers Strain Index score and the age of caregivers. While there is statistically significant, moderately strong positive correlation (coefficient of 0.5702, p=0.0029) between Caregivers Strain Index score and age of caregiver for the subacute group, the association is statistically insignificant for the chronic group. Moreover, the correlation disappears when the two groups are combined. There is positive but statistically insignificant correlation between duration and age of caregiver for the subacute group, while there is a moderate, positive and statistically significant correlation between duration and age of caregiver for the chronic group. However, for the combined sample the association between duration and age of caregiver is insignificant. Looking at the relationship between duration and Caregivers Strain Index score, it is found to be statistically insignificant for both groups, but for the combined sample the correlation is strong, positive and statistically significant (coefficient of 0.7981, p=0.0000). Table 3 first shows the distribution of caregivers by gender and their relationship with the patient, for each group (subacute and chronic) as well for the combined sample. It also tests the difference in burden by gender of caregivers. Among the total participants (caregivers) 16% were male and 84% were female. Out of them 72 % were spouse and 28% were daughter-in-law. The mean Caregivers Strain Index score for female caregivers is marginally greater than that for male caregivers in both subacute and chronic groups as well as for the combined sample. A two sample t-test shows that the difference is not statistically significant.
Discussion
This study highlights the common and persistent strain experienced by caregivers of stroke subjects. The findings of current study suggest higher caregiving burden among stroke caregivers. A similar finding was shown on a systematic review of caregiver burden among stroke caregivers with 25-54% prevalence of burden and the burden was found to remain elevated for an indefinite period following stroke.17On a study done by Rigby H, Gubitz G and Phillips S suggested that factors contributing to caregiver burden in the poststroke period may depend on patient characteristics, social support factors, caregiver’s mental health, the amount of time and effort required for the caregiver.17 Another finding shows moderate positive association between duration and age of the caregiver among the chronic group. A high number of hours of care of a stroke patient per day have been suggested to be related to the burden perceived by caregivers.17 In this study caregivers did not mention specific hours but claimed of looking after the patients most of the time. It has been assumed that partners who provide more care will experience a higher amount of burden.18, 19 A study conducted by Scholte WJ M et.al. Showed that partners of stroke patients perceived most caregiving burden in terms of feelings of heavy responsibility, uncertainty about patients’ care needs, constant worries, restraints in social life, and feelings that patients rely on only their care as the duration of caregiving increases.20 Female caregivers (84%) were more than male caregivers (16%) in this study. Out of them, 72 % were spouse and 28% were daughter-in-law. Similar findings was seen with 41% to 61% of caregivers being spouse in a study conducted by Das S. et.al in Kolkata.13 Another study done on stroke caregivers in Mumbai suggested that men in India are the bread winners and head of the family and women generally look after the family wellbeing at home.2 Also in India, Joint family system ensures that every member of the family helps in caregiving, e.g. spouse, in-laws in physical management, men in organizing medication and finances, children in improving the environment and even neighbours and relatives help in looking after chores.2 This is in contrast to the western culture. Nepal being a neighbouring country of India sharing same culture, a similar situation is also expected in Nepal which may be the major reason for having more female caregivers than male. Caregiving burden and strain plays a major role in the recovery of stroke survivors in the community. A better understanding of how these concepts affect caregivers is a fundamental for developing physiotherapy interventions for rehabilitation programs for successful reintegration of stroke survivors back in the community. Educational background and occupation of the caregivers was not included in the study. Caregiver strain is associated with the functional and emotional status of stroke subjects, recurrent stroke, and depression symptoms in caregivers, which was not considered in this study.
Conclusion
Female caregivers were more than male caregivers with overall Caregiver burden found to be significantly high among subacute and chronic stroke caregivers. Based on the study findings, conducting more intensive study including the type of stroke, quality of life of patient and caregivers both is recommended.
Acknowledgement
Author would also like to acknowledge all the subjects who voluntarily participated in this study. Author ac-knowledges the immense help received from the scholars whose articles are cited and included in references of this manuscript and is also grateful to the authors /editors /publishers of all the articles, journals and books from where the literature for this article has been reviewed and discussed.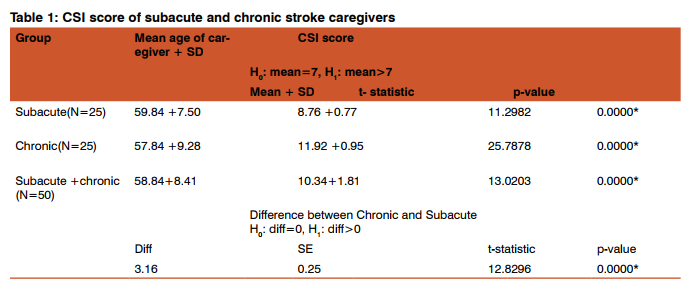
References:
1. Reimer WJM, Haan RJ, Rijnders, Limburg M, Bos GAM. The Burden of Caregiving in Partners of Long-Term Stroke Survivors. Stroke 1998; 29:1605-11.
2. Bhattacharjee M, Vairale J, Gawali K, Dalal PM. Factors affecting burden on caregivers of stroke survivors: Population-based study in Mumbai (India). Ann Indian AcadNeurol 2012;15:113-9.
3. Hileman JW, Lackey NR, Hassanein RS. Identifying the needs of home caregivers of patients with cancer. OncolNurs Forum 1992;19:771-7.
4. Zarit SH, Reever KE, Bach -Peterson J. Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist 1980;20:649-55.
5. Kelly-Hayes M, Beiser A, Kase CS, Scaramucci A, D’Agostino RB, Wolf PA. The influence of gender and age on disability following ischemic stroke: the Framingham study. J Stroke Cerebrovasc Dis. 2003;12:119-26.
6. Wilkinson PR, Wolfe CD, Warburton FG, Rudd AG, Howard RS, Ross-Russell RW, Beech R. Longer term quality of life and outcome in stroke patients: is the Barthel index alone an adequate measure of outcome? Qual Health Care. 1997;6:125-30.
7. Dennis M, O’Rourke S, Lewis S, Sharpe M, Warlow C. A quantitative study of the emotional outcome of people caring for stroke survivors. Stroke 1998;29:1867-72.
8. Thommessen B, Wyller TB, Bautz-Holter E, Laake K. Acute phase predictors of subsequent psychosocial burden incarers of elderly stroke patients. Cerebrovasc Dis. 2001;11:201-6.
9. Blake H, Lincoln NB, Clarke DD. Caregiver strain in spouses of stroke patients. ClinRehabil 2003;17:312-17.
10. Bugge CRN, Alexander H, Hagen S. Stroke patients’ informal caregivers: patient, caregiver, and service factors that affect caregiver strain. Stroke 1999;30:1517-23.
11. Wilkinson PR, Charles DA, Wolfe, Fiona G. Warburton, Anthony G, et al. A long-term follow-up of stroke patients. Stroke 1997;28:507-12.
12. Visser-Meily A, Post M, van de Port I. Psychosocial functioning of spouses in the chronic phase after stroke:Improvement or deterioration between 1 and 3 years after stroke? Patient Education and Counseling 2008;73:153-8.
13. Das S, Hazra A, Ray BK, Ghosal M, Banerjee TK, Roy T, et al. Burden among stroke caregivers-results of a community based study from Kolkata, India. Stroke 2010;41:2965-8.
14. Robinson BC. Validation of a Caregiver Strain Index. J Gerontol 1983;38:344-8.
15. Dozois, David JA, Dobson, Keith S, Jamie L. A psychometric evaluation of the Beck Depression Inventory–II. Psychological Assessment 1998;10:83-9.
16. Wade DT, and Collin C. The Barthel ADL Index: A standard measure of physical disability? Disability and Rehabilitation. 1988;10:64-7. 17. Rigby H, Gubitz G, Phillips S. A systematic review of caregiver burden following stroke.Int J Stroke. 2009;4:285- 92.
18. Poulshock SW, Deimling GT. Families caring for elders in residence: issues in the measurement of burden. J Gerontol. 1984;39:230–239.
19. Seltzer MM, Wailing Li L. The transitions of caregiving: subjective and objective definitions. Gerontologist. 1996;36:614–626.
20. Scholte WJ M et.al. The Burden of Caregiving in Partners of Long-Term Stroke Survivors. Stroke.1998; 29: 1605-11.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





