IJCRR - 7(12), June, 2015
Pages: 31-35
Print Article
Download XML Download PDF
CARTILAGE GROWTH DISORDERS: A REVIEW
Author: G. Ramkumar, Navin Balasubramanian, Vivek Narayan
Category: Healthcare
Abstract:The normal development and growth of various structures in human body gives distinct appearance to the body with proper functions. Growth of individuals mainly depends upon the growth of long bones. Cartilage in epiphyseal end of long bones proliferates to form matrix which gets converted into bone by ossification and calcification. Continuous formation of matrix, conversion of bone helps the longitudinal growth of bone. Various factors disturb the endochondral ossification in various places including the long bones and the growth of bone is disturbed causing stunted growth with deformities in the individual. Thorough study of
the facts and truths of disturbances of cartilage growth of long bones and other parts of bone would help in research to find out the possible remedies to solve the problem in cartilage dysfunction. Hence the present article is prepared to review the various aspects of cartilage, cartilage growth disturbances in endochondral ossification, stunted growth and deformities.
Keywords: Cartilage, Basicranium, Mandibular condyle, Epiphyseal cartilage
Full Text:
INTRODUCTION
Skeletal growth and growth in longitudinal direction of an individual depends upon proper cartilage function as cartilage plays a vital role in multiple growth centers of the body. 10Mesenchyme of embryonic germinal layer gives rise to formation of cartilage by producing cartilaginous matrix in which fibers are embedded to form homogenous cartilage. 10Depending upon the amount and type of fibers, the cartilage is called as hyaline cartilage, elastic cartilage and fibroelastic cartilage. Cartilage exists in pinna of the ear, nose, nasal septum, respiratory tract, ribs and articular surfaces of joints. In cartilage growth center cartilage proliferates and elaborates a matrix which is slowly replaced by ossification and calcification to form bone through endochondral ossification9 . This normal physiological function of cartilage turning into bone is affected by known and unknown causes. The development and growth of bone particularly the long bones are affected causing stunted growth and deformities. These disorders are being described and discussed in this article.
CARTILAGE GROWTH CENTERS
Cartilage growth centers exist in many places of the body but the following places are important for the growth of structure6, 7, 12.
1. Basicranium
2. Condyle of mandible
3. Epiphyseal end of long bones
CARTILAGE IN BASICRANIUM
Cartilage growth center exist in the base of the skull in the form of synchondrosis12. Cartilage synchondrosis is bipolar cartilage cells on either side with a central zone of persistent cartilage cells8,12. Spheno-occipital synchondrosis, 12 mid-sphenoidal synchondrosis and sphenoethmoidal synchondrosis are present in the base of skull. Persistent cartilage cells proliferate on either side and elaborate a matrix. This matrix further undergoes ossification and calcification to form bone through endochondral ossification12. Spheno-occipital synchondrosis exists in basicranium12. In the anterior part of spheno-occipital synchondrosis, cartilage cells proliferate to form a matrix which gets ossified and calcified to form sphenoid bone. The posterior part of cartilage cells proliferates to form matrix which gets ossified and calcified to form occipital bone. Thus the spheno-occipital synchondrosis is converted into spheno-occipital bone of the skull12. The sphenoid bone in the anterior part is attached with pterygoid plates which in turn join the maxillary bone. Growth of sphenoid bone in basicranium pushes the petrygoid plates which in turn push to maxilla to form mid dle part of face. Any disturbances in the development of sphenoid bone in the anterior part of spheno-occipital synchondrosis causes arrested growth of sphenoid bone. Failure of forward growth of maxilla occurs due to the arrested growth in the base of the sphenoid bone [figure 1] and this causes the deformity of retruded maxilla in the midface.
CLINICAL CHANGES DUE TO DISTURBANCE OF SPHENOID BONE FORMATION IN THE CRANIAL BASE
In the craniofacial development, midface hypoplasia in cleidocranial dysostosis occurs and this is due to inadequate ossification of the cranial base12. As a result of the disturbance in formation of sphenoid bone in cranial base the forward movement of maxilla is not possible. In Crouzon5, 9, 12 syndrome [figures 4, 5 and 6] due to genetic disturbance, early closure of spheno-occipital synchondrosis occur due to failure in the development of the anterior part of sphenoid bone and posterior part of occipital bone. This results in short base of skull and midface hypoplasia[figures 4, 5 and 6]. 12Midface malformation due to cranial base disturbances also occurs in Apert syndrome5 and Turner’s syndrome12. Midface hypoplasia occurs in achondroplasia due to the disturbances of cartilage growth in spheno-occipital synchondrosis3 .
CARTILAGE IN CONDYLE OF MANDIBLE
The head of mandibular condyle articulates within the glenoid fossa to form temporomandibular joint6 . Mandible on either side develops separately and joins in the midline. During development, the anterior part of mandible develops from differentiation of fibrous tissue around the Meckel’s cartilage through intramembranous ossification. The posterior part of mandible is formed by endochondral ossification of condyle of mandible [figure 2]. Condyle of the mandible is a growth center and consists of hyaline cartilage. Cartilage cells in condyle proliferate and elaborate a matrix downwards. The matrix gets calcified and bone is formed. Further proliferation of cartilage cells and further matrix formation pushes the bone downwards. 11Formation of cartilage matrix, conversion of matrix into bone continuously help to form the bone which helps in the forward growth of mandible. While the anteroposterior growth of mandible is formed by endochondral ossification of condyle, the horizontal growth of mandibular body is formed by surface apposition of bone in the preformed intramembranous ossification. Any disturbances to condylar cartilage growth center affect the development and growth of posterior part of mandible resulting in arrested growth of mandible. The following conditions are due to the disturbance of condylar growth center.
1. Agenesis of condyle
Agenesis of condyle is congenital absence of condyle due to failure of formation of condyle on one side. It is associated with hemifacial microsomia, where unilateral absence of condyle occurs. Clinically the individual has depression in the preauricular region with absence of auricle and external auditory meatus. The mandible in the affected side has arrested growth with deviation of mandible from unaffected side causing a shift in the midline. Palpation will reveal total absence of condyle and condylar movement in the affected side. Facial deformity with microstomia is a characteristic feature. Prenatal growth disturbance of condyle is the cause of agenesis of condyle.
2. Aplasia of condyle
Aplasia of condyle is an attempted formation of miniature condyle where the growth of condyle and endochondral ossification is affected. It may be unilateral or bilateral. In unilateral aplasia of condyle, the mandible will be small due to arrested growth in that side. On palpation the condyle will be small in size but the movement is not affected. On the unaffected side the growth of mandible is normal causing deviation of mandible and shift of midline towards the affected side. Bilateral aplasia of condyle causes arrested growth of mandible on both sides causing mandibular micrognathism.
3. Hypoplasia of condyle
Hypoplasia of condyle [figures 7, 8 and 9] is reduced size of condyle due to developmental disturbance6 . This may occur unilaterally or bilaterally. As the condyle is hypoplastic and there is disturbance in endochondral ossification on one side, it causes arrested growth of mandible on one side and results in facial deformity [figures 7, 8 and 9]. The unaffected side of mandible grows normally but is deviated to affected side shifting the midline. If hypoplasia occurs on both sides, arrested growth occurs resulting in micrognathism. Due to arrested growth of mandible there is a depression at the junction of ramus and body called antegonial notch. Thus when cartilage growth center in condyle of mandible is affected, arrested growth of mandible occurs causing deformity. The exact cause of prenatal disturbance of cartilage growth center is not fully understood but may be due to certain developmental disturbances.
4. Unilateral condylar hyperplasia
Disturbances in cartilage growth in many places occur as a deficiency or absence of growth of cartilage. But in condylar growth centers, cartilage overgrowth occurs resulting in condylar hyperplasia4 where cartilage produce excessive matrix and bone resulting in a large mandible with excessive anteroposterior growth. In unilateral condylar hyperplasia there is bending of the lower border of mandible with deranged occlusion of teeth. The unaffected side is normal.
CARTILAGE IN EPIPHYSEAL END OF LONG BONES
The growth of long bone in vertical direction is purely due to the presence of cartilage in the epiphyseal end of long bones7 [figure 3]. The cartilage proliferates and forms a matrix which gets calcified to form bone. Continuous proliferation of cartilage to form matrix and the matrix ossifying into bone causes growth in the length of bone. The growth of diaphysis in horizontal direction is by intramembranous ossification. If the endochondral ossification in epiphyseal end is disturbed, different deformities occurs with a common sign of stunted growth/dwarfism9 . Achondroplasia is a condition in which absence of cartilage growth occurs. Absence of cartilage growth in spheno-occipital synchondrosis causes midface hypoplasia and shortening of base of skull. Absence of cartilage growth in epiphyseal end in achondroplasia results in stunted growth of long bones in extremities with short stature of the individual [figures 10, 11 and 12]. Deficient ossification of cartilage matrix in epiphyseal end causes stunted growth with flattened vertebral body in Morquio Brailsford disease. Abnormal ossification of epiphyses causes stunted growth in dysplasia epiphyseal multiplex10. Osteopetrosis is a genetic disorder in which failure of bone resorption causes excess bone formation which obliterates the blood vessels and the viability of bone in that area is lost1 . Osteomyelitis can develop in the affected bone due to a compromised blood supply. In osteopetrosis continuous bone formation occurs and failure of bone resorption causes unresorbed cartilage. This causes widening of bone with club shaped appearance of metaphysis of long bones. Thus the persistent cartilage causes defects in bone10. The cartilage matrix formed in the epiphyseal end fails to calcify and more amount of cartilage accumulates in the metaphysis affecting the longitudinal growth of long bone in Ollier’s disease10. Shortness of affected extremities due to chondrodystrophic calcification congenita and stippled epiphyses is a rare congenital disease with discrete spots of calcification affecting cartilaginous structure. A single limb may be affected10. Cartilage growth disturbances occurs in epiphyseal end of long bones due to genetic disturbances resulting in stunted growth of extremities with a clinical appearance of a long trunk and short extremities, polydactyly with cardiac changes in Ellis-van Creveld syndrome2 . Growth of any organ depends upon the metabolic activities of growth hormones, pituitary hormone and thyroid hormone. Epiphyseal cartilage growth is also suppressed when there is a deficiency of these hormones and cause stunted growth in hypopituitarism and hypothyroidism9 . Stunted growth occurs in Gargoylism due to chondroosteodystrophy10 and is associated with mental retardation, cloudy cornea and enlargement of liver and spleen.
DISCUSSION
It is true that proper growth of an individual depends upon the proper growth of cartilage in the cartilage growth centers, since midface deformity is due to the disturbance in growth of spheno-occipital synchondrosis12. Arrested growth of mandible is due to defective condylar growth and stunted growth is due to failure of cartilage growth center in epiphyseal end of long bones11. Craniofacial deformities are due to disturbances in growth centers of cranial base. Cartilage growth disturbance in spheno-occipital synchondrosis may be only a local disturbance without involving other growth centers as we find that in Crouzon’s disease only face is affected. But in achondroplasia, cartilage growth disturbances occur both in spheno-occipital synchondrosis and in the epiphyseal cartilage growth center resulting in midface deformity and stunted growth of long bones. Anterior cranial base is affected more than posterior cranial base and the skull base is shortened in the cartilage growth disturbances of the cranial base. Since cranial base growth disturbance is due to mutation of genes, a thorough research study may be helpful to solve this problem. Arrested growth of mandible due to disturbances in cartilage growth center of condyle appears to be an independent disorder without involving other cartilage growth centers. Arrested growth of mandible is not associated with other skeletal deformities like midface hypoplasia or stunted growth. This appears to be more of prenatal disturbances rather than genetic involvement. Cartilage growth disturbances in condyle cause aplasia and hypoplasia of condyle resulting in arrested growth of mandible. But condylar hyperplasia also occurs with the formation of large body of mandible for which the reason in not known. The major cause of individual stunted growth/dwarfism is mainly due to disturbed growth of epiphyseal cartilage of long bones. This may be a physiological alteration due to pituitary and thyroid deficiency or due to genetic disturbances. There is no absence of cartilage in epiphyseal growth center but the existing cartilage does not grow or grows abnormally. In the abnormal cartilage, there is failure of ossification and calcification. The reason behind failure of growth, ossification and calcification of cartilage is not fully understood but genetic changes have been proposed. Cartilage growth in the epiphyseal end without ossification and calcification may occur as masses in the long bone. Single long bone may also be affected. In certain conditions, epiphyseal cartilage growth is affected in association with ectodermal dysplasia and cardiac manifestations in Ellis-van Creveld syndrome and mental retardation, cloudy cornea, spleen and liver enlargement are seen in Gargoylism. The systemic symptoms do not have any relevance in the failure of cartilage growth. Disturbances in epiphyseal cartilage growth are not associated with condylar cartilage growth but is seen in cranial base disorders as in achondroplasia.
CONCLUSION
Disturbances in cartilage growth centers causing stunted growth and deformity have been explained. Stunted growth of long bones, arrested growth of mandible and sphenoid bone are the features of cartilage growth disturbances. Disturbances are not uniform and may vary for every growth center. Continuous and constant research in genetics and prenatal disturbances pertaining to the cartilage growth disturbances may be carried out and this research may reveal some newer concepts which may help to prevent the cartilage growth disorders. This review article would act as a basis for further evaluation and research of cartilage growth disturbances.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
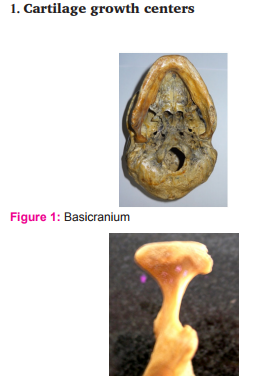
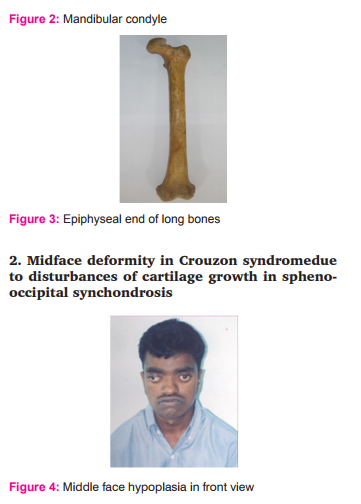
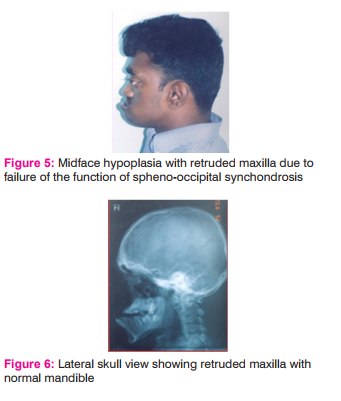
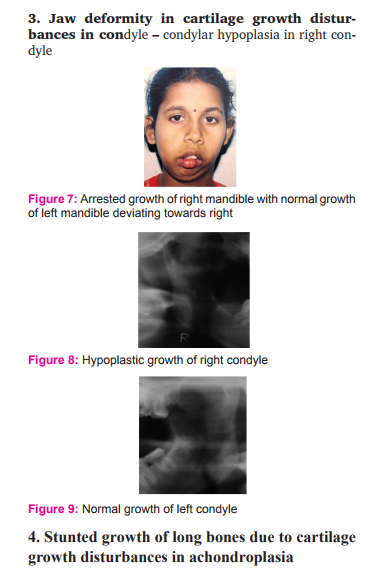

Figure 12: Stunted growth of lower extremities
References:
1. Bollerslev J. (1987) Osteopetrosis: a genetic and epidemiological study. Clin Genet 31:86–90.
2. Baujat G, Le Merrer M. Ellis-van Creveld syndrome. Orphanet J Rare Dis 2007;2:27.
3. Baujat Geneviève et al.AchondroplasiaBest Practice and Research Clinical Rheumatology, March 2008 Volume 22, Issue 1, 3–18.
4. Jonck LM. Facial asymmetry and condylar hyperplasia. Oral Surg Oral Med Oral Pathol 1975;40:567-573.
5. Kreiborg S,Cohen M.M, et al. Is craniofacial morphology in Apert and Crouzon syndromes the same? – Acta odonto scand. 1998 vol 56, no 6: 339–341.
6. Kreutziger, KL, Mahan, PE. Temporomandibular degenerative joint disease. Part I. Anatomy, pathophysiology, and clinical description. Oral Surg Oral Med Oral Pathol. 1975; 40:165–182.
7. Karlen AG, Cameron JA. Dysplasia epiphysialis punctata; report of a case with discussion. J Bone Joint Surg Br. 1957 May; 39-B (2):293–301.
8. Mølsted K, Kjaer I, Dahl ESpheno-occipital synchondrosis in three-month-old children with clefts of the lip and palate: a radiographic study. Cleft Palate–Craniofacial Journal 1993; 30:569–573.
9. Robert B Duthie, George Bentley, Mercer’s orthopedic surgery volume I ninth edition.
10. Samuel.L.Turek, Orthopedics: principles their application 4th edition.
11. Sicher, H. Functional Anatomy of the Temporomandibular Joint. in: B. Sarnat (Ed.) The Temporomandibular Joint. Charles C Thomas, Publisher, Springfield, Ill; 1951.
12. Nie X. Cranial base in craniofacial development: developmentalfeatures, influence on facial growth, anomaly, and molecular basis.Acta Odonto Scand 2005; 63: 127–35.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





