IJCRR - 7(12), June, 2015
Pages: 19-23
Print Article
Download XML Download PDF
A CASE REPORT OF FACIAL NERVE SCHWANNOMA CO-EXISTING WITH AN EXTERNAL AUDITORY CANAL OSTEOMA: PRESENTATION OF UNILATERAL FACIAL ASYMMETRY WITH CONDUCTIVE HEARING LOSS
Author: Kriti Bhujel
Category: Healthcare
Abstract:Aim: We present here a case of facial schwannoma co-existent with an external auditory canal osteoma which presented with a history of unilateral facial asymmetry with conductive hearing loss. Case Report: A 50 year old female presented with progressive unilateral facial asymmetry of the left side since 5 years, with gradually progressive hearing loss in the left ear since 2 months. Examination revealed left-sided unilateral lower motor neuron facial palsy and a whitish bony hard mass in the left external auditory canal. CECT and CEMR scan of temporal bone showed a neoplasm arising from the vertical segment of left facial nerve. Modified radical mastoidectomy was done to trace the facial nerve lesion along the vertical segment of the facial nerve in the temporal bone and the exploration was extended along its extratemporal segment. The neoplasm was excised and histopathology examination revealed facial nerve schwannoma. The bony mass in the external auditory canal was excised and histopathological examination confirmed it to be an osteoma. Conclusion: The gradually progressive unilateral facial asymmetry was due to the facial nerve schwannoma, while the unilateral conductive hearing loss was explained by the presence of the osteoma in the external auditory canal. The patient was cleared of the disease and physiotherapy was started. The asymmetry of the face improved from House-Brackmann grade 5 to 4 within a month. The hearing threshold improved to within the normal hearing range. The patient has been followed up for 6 months and there is no recurrence of symptoms.
Keywords: Facial asymmetry, Conductive hearing loss, Facial nerve schwannoma, Osteoma, House-Brackmann staging
Full Text:
INTRODUCTION
A facial nerve schwannoma is a slow-growing tumor and may involve any part of the nerve. The posterior fossa and/or cerebellopontine angle is involved in about 50 percent of cases. Symptoms most often include dysfunction of the seventh or eighth cranial nerves. On CT and MRI, the mass appears identical to a vestibular schwannoma and the key to diagnosis is the neuroanatomic location of the tumour.1-4 Features include widening of the Fallopian canal in the temporal bone.3,4 For patients with mild or no facial dysfunction, a conservative attitude with observation and, if necessary, only debulking surgery is appropriate, sparing facial nerve function. The surgical approach depends upon tumor extension and location. Re-routing of the nerve is preferred when possible, but cable grafting is often necessary.1,3,4 Malignant tumors have been reported and may occur as part of the Neurofibromatosis type 2 (NF2) syndrome.4 Histologically, they are composed of cellular Antoni A areas with Verocay bodies and hypocellular myxoid Antoni B areas. Tumor cells are strongly and diffusely immunoreactive for S-100 protein. An osteoma of the external auditory canal is a benign growth of periosteal bone, which forms a solitary, dicrete, pedunculated, hemispherical swelling in the lateral part of the meatus, around the tympanomeatal junction, adjacent to the tympanic membrane. They are usually single. They are usually found as an incidental finding during the examination of an asymptomatic patient. No treatment is required in most asymptomatic cases. Canalplasty is indicated for refractory cases of recurrent otitis externa and frequent cerumen obstruction.
CASE REPORT
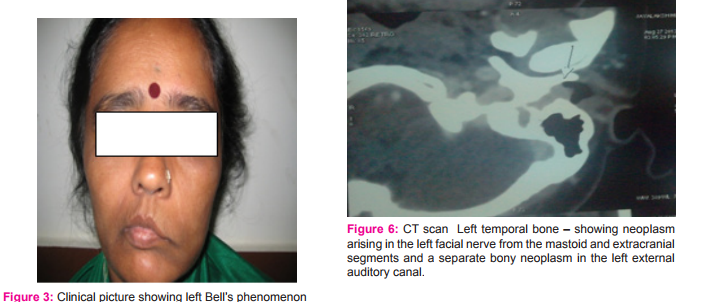
A 50 year old female presented with complaints of gradually progressive left sided facial asymmetry since 5 yrs and gradually progressive unilateral hearing loss in the left ear since 2 months. The patient noticed deviation of the angle of mouth towards the right side 5 years back, which started as a slight deviation which was noticed only when the patient smiled and slowly progressed to be present even at rest. (Fig.1) The facial asymmetry then progressed, with associated drooling of saliva and food and water from the left angle of the mouth and the patient was not able to close her left eye properly. She gave a history of watering and itching of the left eye as well. She also complained of reduced hearing in the left ear since 2 months, which was insidious in onset and gradually progressive. It was associated with intermittent fullness in the left ear. On examination of the ears after removal of cerumen, a whitish pedunculated growth was seen in the left external auditory canal, arising from the posterior wall, about 2 mm medial to the costochondral junction and encircling about 1/3 rd of the canal. On probing, it was hard in consistency, non-tender and did not bleed on touch. The tympanic membrane could not be visualized. Tuning fork tests revealed conductive hearing loss in the left ear. The right ear was grossly normal on examination. Facial nerve examination showed absence of wrinkling of the forehead on the left side (Fig. 2), left-sided Bell’s phenomenon was present (Fig. 3), deviation of the angle of mouth to the right when clenching teeth (Fig.4), and inability to blow out left cheek or to whistle (Fig.5). Taste over the anterior two-thirds of the tongue was normal and Schirmer’s test showed normal values bilaterally. CECT and CEMR scan of the temporal bones showed a heterogeneous iso-to-hypodense lesion noted in the left paraspinal component of the perivertebral space, extending into the stylomastoid foramen. A hyperdense lesion was also seen in the left external auditory canal, involving the bony posterior wall of the external auditory canal. The lesion was seen to cause scalloping of the anterior wall of the left external auditory canal. It was also seen to be pushing the left tympanic membrane medially. The segment of the left facial nerve 8mm proximal to the posterior genu was seen to be thickened. The facial nerve distal to the posterior genu was not seen separately from the above described lesion. The lesion was seen to abut the left styloid process. Ossicles and inner ear structures were found to be normal. These findings were suggestive of a neoplasm arising in the left facial nerve from the mastoid and extracranial segments and a separate bony neoplasm in the left external auditory canal. (Fig. 6, 7) The patient subsequently underwent Modified radical mastoidectomy under general anesthesia. Intraoperatively, a tumor involving the vertical segment and extratemporal segment of the left facial nerve was noted and the same was excised. Left canalplasty was done. The ossicles were found to be intact. Inlay greater auricular nerve grafting was done. The graft was placed in position and meatoplasty was done. (Fig. 8,9) Histopathological examination of the excised tumors revealed features suggestive of schwannoma of the facial nerve and a benign growth of bone from periosteum giving rise to the onion skin histologic appearance of lamellar bone suggestive of osteoma.
DISCUSSION
Facial schwannomas are benign, slow-growing tumors that arise from Schwann cells within the nerve sheath, and are often diagnosed late. Two types of tissue are distinguishable; the compact interwoven bundles of Antoni A, and the looser, more disordered cellular arrangement of Antoni B. The histological appearance cannot differentiate facial schwannomas from vestibular schwannomas and have no clinical, surgical or prognostic significance.5 Facial schwannomas are encapsulated tumors attached to the nerve. They are usually intimately adherent to the nerve trunk, often compressing the nerve against other structures. The tumor is usually slow-growing and can involve multiple segments of the nerve. A proportion of schwannomas are found within the body of the nerve, the nerve fibers either running through the tumor or splayed around its capsule.6 The geniculate ganglion (68.2 %) and labyrinthine portion (52.3 %) are the most commonly affected segments. Multiple segment tumors are almost twice as common (63.6 %) as single segment tumors (36.4 %).7 Facial nerve schwannomas grow in the direction of least resistance.8 Facial nerve schwannomas may be asymptomatic or can present with a wide variety of symptoms. There can be progressive or acute facial nerve palsy. Associated otological symptoms such as conductive and/or sensorineural hearing loss can occur. Mass effect on adjacent nerves may well cause sensorineural hearing loss (SNHL) or even conductive hearing loss if growth into the middle ear impairs the normal function of the ossicles. In a minority of cases (~10%) the tumor is extra-cranial, where it presents as an asymptomatic parotid mass.9 Surgery is the only treatment for facial nerve schwannoma and therefore patients are left with permanent facial dysfunction after treatment because tumor removal almost always requires total nerve resection. Osteomas of the external auditory canal are discrete, pedunculated bone lesions arising along the tympanosquamous suture. The most common location of osteomas in the temporal bone is the external auditory meatus, followed by the mastoid and temporal squame with other sites being exceptional. 10,11 They can present with recurrent otitis externa because the self cleansing mechanism of external canal has been compromised. When the external auditory canal aperture becomes reduced to 3 mm, high frequency hearing loss occurs, and further reduction in size could lead to lower frequency losses.12 It is managed surgically only when the patient suffers from recurrent episodes of otitis externa or conductive hearing loss, and surgery is usually done via the transmeatal route.
CONCLUSION
The patient presented with symptoms of gradual unilateral facial palsy and conductive hearing loss. After clinical and diagnostic investigations it was concluded that the patient had left facial nerve schwannoma along with a co-existing external auditory osteoma. At postoperative 1 year follow up, there is no recurrence of the schwannoma or osteoma. The facial palsy has improved from House- Brackmann 5 to 4. The patient’s hearing is in the normal range at present.
ACKNOWLEDGEMENT
The author acknowledges the immense help received from the scholars whose articles are cited and included in the references of this manuscript. The author is also grateful to the authors, editors and publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. The author wishes to thank the Head of the department of ENT, Central Referral Hospital, Sikkim Manipal Institute of Medical Sciences, Dr. Suvamoy Chakraborty for his constant support and expert guidance. The author would also like to thank her fellow colleagues and post graduate students for their help, and the departments of Radiology and Pathology for their expert inference on the case. A special thanks to my dear friend Dr. Davis Thomas for always being there to help me.


References:
1. Moffat DA, Ballagh RH. Rare tumors of the cerebellopontine angle. Clinical Oncology (Royal College of Radiologists (Great Britain). 1995; 7: 28-41.
2. Bonneville F, Sarrazin JL, Marsot-Dupuch K, Iffenecker C, Cordoliani YS, Doyon W et al. Unusual lesions of the cerebellopontine angle: A segmental approach. Radiographics. 2001; 21: 419-38.
3. Lalwani AK. Meningiomas, epidermoids, and other nonacoustic tumors of the cerebellopontine angle. Otolaryngologic Clinics of North America. 1992; 25: 707-28.
4. Bartels U, Arrington JR. Rare Tumors of the cerebellopontine angle. In: Jackler RK, Brackmann D (eds). Neurotology. St Louis: Mosby, 1994: 835-61.
5. Maran AGD. Benign diseases of the neck. In: Kerr AG (ed.). Scott-Brown’s otolaryngology, 6th edn. London: Butterworth Heinemann, 1997: 5/16/8-10.
6. Hajjaj M, Linthicum FH. Facial nerve schwannoma: Nerve fibre dissemination. Journal of Laryngology and Otology. 1996; 110: 632-3.
7. Kertesz TR, Shelton C, Wiggins RH, Salzman KL,Glastonbury CM, Harnsberger R. Intratemporal facial nerve neuroma: Anatomical location and radiological features. Laryngoscope. 2001; 111: 1250-6.
8. King TI, Morrison AW. Primary facial nerve tumors within the skull. Journal of Neurosurgery. 1990; 72: 1-8.
9. Marzo, Sam J; Zender, Chad A; Leonetti, John P. Facial nerve schwannoma. Current opinion in otolaryngology and Head and Neck Surgery.2009 ;17: 5:346-50
10. Denia A, Perez F, Canalis RR, Graham MD. Extracanalicular osteomas of the temporal bone. Arch Otolaryngol Head Neck Surg 1979; 105: 706-9.
11. Camacho RR, Vicente J, Cajal SR. Imaging quiz case 2. Arch Otolaryngol Head Neck Surg 1999: 125: 349, 351-52.
12. Sheehy JL. Diffuse exostoses and osteomata of the external auditory canal: A report of 100 operations. Otolaryngology, Head and Neck Surgery. 1982; 90: 337-42.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





