IJCRR - 7(12), June, 2015
Pages: 15-18
Print Article
Download XML Download PDF
SOCIO-DEMOGRAPHIC PROFILE OF CEREBRAL PALSY AFFECTED PATIENTS: AN INDIAN SCENARIO
Author: Varidmala Jain, Gyanendra Singh, Jitendra Kumar Jain, Arvind Dayal, Neena Gupta, Tapas Pal
Category: Healthcare
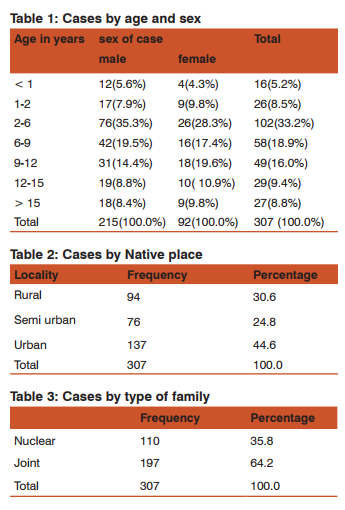
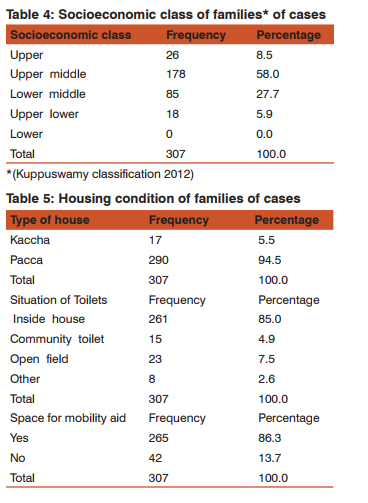
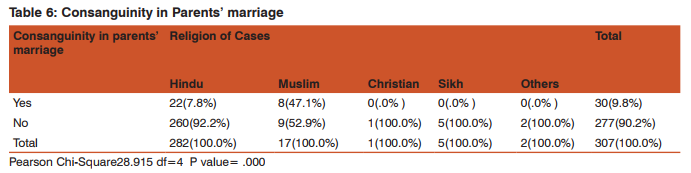
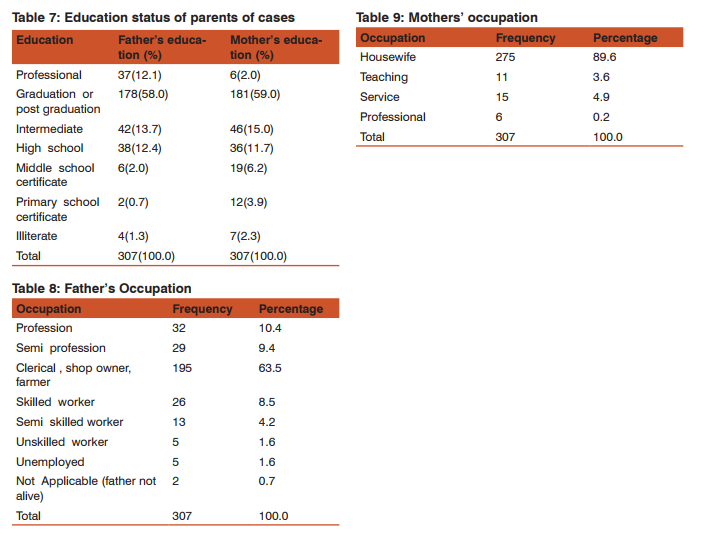
Abstract:Objective: This study was conducted with the aim of describing existing demographic profile of patients and their families coming to the rehab center for treatment. Method: Parents of total 307 patients were respondents. Result: Out of total 307 children only 30% (92) were females. Most common age of presentation was 2-9 years. 64.2% (197) patients belonged to joint families and maximum 58 % (178) belonged to upper middle class. Only 85% (261) families had toilets inside their houses. It was found that consanguineous marriages was found in both Muslims 47.1% (8) and Hindus 7.8% (22). 10.4% (32) fathers were professionals. Maximum mothers 89.6% (275) were housewives despite of high level of education (graduation or above) in 61% (187). Conclusion: Social issues like gender biasness, family support system and socioeconomic profile affect to a great extent the treatment seeking of these families.
Keywords: Cerebral palsy, Socioeconomic status, Consanguinity, Housing condition
Full Text:
INTRODUCTION
Bax1 (1964) has defined cerebral palsy as a ‘disorder of movement and posture due to a defect or lesion of the immature brain.’ According to another study2 ,‘cerebral palsy is an Umbrella term covering a group of non progressive but often changing motor impairment syndromes secondary to lesions or anomalies of brain arising in the early stages of development.’ According to Stanley3 (2000) Cerebral palsy (CP) is the most common congenital neurological disorder. The world wide prevalence of cerebral palsy is 2-2.5/1000 live births. Although in developed world lot of literature on various aspects of cerebral palsy are available, in developing world specially Asia and India literature is scarce. This study was done to describe the socio-demographic profile of families belonging to cerebral palsy affected patients.
METHOD
A descriptive study was done on 307 patients, who came for treatment at Samvedna Trust, Allahabad, India during one year duration. Study was conducted to describe the socio-demographic profile of cases with cerebral palsy and their families. Parents of cases or any guardian, mostly mothers were the respondents. Ethical approval was obtained from Institutional Ethics Committee, Sam Higginbottom Institute of Agriculture Technology and Sciences, Allahabad, India before collection of data. Informed consent was obtained from the respondents.
RESULT
Out of total 307 children only 30% (92) were females. Most common age of presentation was 2-9 years because that is the time when the developmental anomalies and delay in milestones become very obvious. Although trend of Nuclear families is on increase but in the present study it was found that 64.2% (197) patients belonged to joint families and maximum 58 % (178) belonged to upper middle class. In spite of this only 85% (261) families had toilets inside their houses and other 15% were forced to go outside for this daily biological need. Although 47.1% (8) Muslims had history of consanguinity. Contrary to normal belief 7.8% (22) Hindus out of 282 also had consanguineous marriages. Maximum fathers 63.5% (195) were having clerical or other kinds of jobs; business or some of them were also farmers. 10.4% (32) fathers were also professionals. Maximum mothers 89.6% (275) were housewives despite of high level of education (graduation or above) in 61% (187).
DISCUSSION
Gender difference was apparent in our study, since ratio of males was more as compared to females 7:3. This difference is much more significant compared to other studies from most parts of the world. The prevalence in United States was found slightly higher in boys than in girls (male/female ratio, 1.4:1)4. Many studies analyze reason for it. According to a study5 it was stated that sex may have some influence on pathogenesis of developmental brain injuries. It was stated in the study that sex differences in the immature brain appeared to be strongly influenced by intrinsic differences between male and female cells due to their distinct chromosomal complements. In our study the difference is much higher than this which may be because of some gender biasness in health seeking for female child in developing countries. Locality, family type and socioeconomic class may be independent factor but in this study these all seems to have an effect on accessibility of treatment as it was seen that more people from urban and semi urban area approached for treatment and also more from middle socioeconomic status, none of the families belonged to lowest socioeconomic class. Solaski M.6 included twelve studies in the systematic review. Of these, eight found low SES to be a risk factor for increased CP prevalence. The probable reason of discrepancy in this study was that in the far rural and lower income families’ awareness regarding availability of treatment and affordability for seeking long term treatment are very low. In spite of an increasing trend in nuclear family system, majority of patients belonged to joint families because joint family persons could manage to stay out of their families for long duration of treatment because they had a support back at their homes who could look after other siblings of the child and also other parent mostly fathers. Consanguinity is considered as one of the risk factors for cerebral palsy. According to a Turkish study, conducted by Erkin G et.al,7 23.8 % parents had consanguineous marriages. In our study it was observed that 7.8% Hindu parents were also having consanguineous marriage which is not considered a common practice among north Indian Hindus. If we analyze the housing condition, not having toilets inside their houses put affected child and their caregiver to an extremely difficult situation who are already very much compromised for their ambulation. Also many families did not have walking space for the mobility aid. These circumstances put a very serious threat for functioning ability of these children in future also. In an era when we are looking for facilities at the community level for their uninterrupted mobility, children in developing country are still struggling at the basic level for these. Education level of both the parents was quite good; majority of them having education graduation or above. This was the reason why they were sensitive and aware enough to find appropriate treatment for their children to the best of their capability. Maximum mothers were housewives in spite of good education. Many of them had compromised their jobs and carriers to take care of their child leaving their husbands as the sole earners. Same time their education helped them to understand and deal the problem of their child in a better way
CONCLUSION
Social issues like gender biasness, family support system and socioeconomic profile etc affect to a great extent to treatment seeking specially in case of long term treatment. Considering large number of cerebral palsy affected children in our society there is need to increase awareness for this condition and removal of the myth that nothing can be done for them. The families need constant motivation to help bring these children to mainstream of the society and also there is need to increase both quantity and quality of facilities providing treatment to them.
ACKNOWLEDGEMENTS
We acknowledge physiotherapists of Samvedna Trust for helping in data collection. The study was self financed by the corresponding author. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Bax MCO. Terminology and classification of cerebral palsy Dev Med Child Neuro. 1964; 6:295–307.
2. Mutch L, Alberman E, Hagberg B, Kodama K, Perat MV. Cerebral palsy epidemiology: where are we now and where are we going? Dev Med Child Neurol. 1992; 34: 547–551
3. Stanley F, Blair E, Alberman, E. Cerebral Palsies: Epidemiology and Causal Pathways. Clinics in Dev Med. 2000; No. 151. London: Mac Keith Press. 19.
4. Arneson C, Durkin M, Benedict RE, Kirby RS, Yeargin -Allsopp M, Van Naarden Braun K, Doernberg N. Brief Report: Prevalence of Cerebral Palsy: Autism and Developmental Disabilities Monitoring Network, Three Sites, United States, 2004. Disability and Health 2008;2:45-48.
5. Johnston M V, Hagberg H. Sex and the pathogenesis of cerebral palsy. Dev Med Child Neurol. 2007, 49: 74–78
6. Solaski M, Majnemer A, Oskoui M. Contribution of socioeconomic status on the prevalence of cerebral palsy: a systematic search and review. Dev Med and Child Neurol. 2014; 56: 1043–1051
7. Erkin, G., Delialioglu, S. U., Ozel, S., Culha, C. and Sirzai, H. Risk factors and clinical profiles in Turkish children with cerebral palsy: Analysis of 635 cases. Int J Rehab Res. 2008; 31(1), 98-91.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





