IJCRR - 7(13), July, 2015
Pages: 62-68
Print Article
Download XML Download PDF
PREGNANCY OUTCOME IN ISOLATED OLIGOHYDRAMNIOS AT OR BEYOND 34 WEEKS OF GESTATION
Author: Kavitha G.
Category: Healthcare
Abstract:Objectives: A significant reduction in the amount of amniotic fluid co-relates with an increased rate of both perinatal morbidity and mortality. The objectives of the study are to determine the neonatal outcome, and the appropriate route of delivery in isolated oligohydramnios.
Methodology: This was a prospective case-control study conducted over a period of 22 months (November 2006 to August 2008) at department of obstetrics and gynecology, Basaveshwar Teaching and General Hospital and Sangameshwar Hospital, attached to Mahadeveppa Rampure Medical College, Gulbarga. The study consists of analysis of pregnancy outcome in 50 antenatal patients with the ultrasound diagnosis of oligohydramnios (AFI ? 5) at or beyond 34 weeks of gestation. Oligohydramnios was defined as ultrasound diagnosis of amniotic fluid index ?5cm. Inclusion Criteria included singleton pregnancy of any order of parity with gestational age ? 34 weeks and AFI ? 5cm. Multiple gestation, gestational age < 34 weeks and >40 weeks, AFI > 5cm and < 5cm, ruptured membrane, pregnancy induced hypertension and congenital anomalies were excluded from the study. The results were analyzed using parameters like standard deviation, chi square test and 'Z' test. Results: There was statistically significant difference in two groups in non-stress NST, rate of induced labor, cesarean section rate, IUGR, low birth weight, admission to NICU and no difference in meconium stained liquor and Apgar score < 7 at 5 minutes. Conclusion: Pregnancies with isolated oligohydramnios (AFI ? 5) at or beyond 34 weeks is associated with increased rates of non reactive NST, FHR deceleration during labor, development of fetal distress, caesarean delivery and low birth weight.
Keywords: Isolated oligohydramnios, Non stress test, FHR deceleration.
Full Text:
INTRODUCTION
Importance of amniotic fluid volume as an indicator of fetal status was appreciated relatively recently.1 Amniotic fluid has a number of important roles in fetal development. It cushions the fetus against trauma, has antibacterial property and promotes growth and development of gastrointestinal and musculoskeletal system.2 It helps to maintain the fetal body temperature and plays a part in the homeostasis of fluid, and permits fetal movements.2, 3 Amniotic fluid volume maintains amniotic fluid pressure there by reducing the loss of lung fluid - an essential component to pulmonary development. It prevents compression of the umbilical cord.4 Decreased amniotic fluid volume is frequently one of the first clues to an underlying fetal abnormality or maternal disease state.5 Most common quantitative measure for fluid volume used in clinical practice is AFI. It is calculated by dividing the uterus externally into 4 quadrants and using ultrasound to measure vertical diameter of the largest pocket in each quadrant in millimeter, which is then summed to calculate AFI.6. AFI ≤ 5cm is the accepted cut off for the diagnosis of oligohydramnios. Ante partum diagnosis of oligohydramnios by means of AFI accounted for 2.3% of pregnancies undergoing sonography after 34weeks.7 Sonogram – assisted diagnosis of oligohydramnios is associated with increased pregnancy intervention, still birth, fetal heart rate deceleration during labor and increased neonatal morbidity and mortality rates.7 Oligohydramnios can be an idiopathic finding in women who have low risk pregnancies and no medical or fetal complication.8 The present study was designed to study the outcome of pregnancies with AFI ≤ 5cm at or beyond 34weeks of gestation.
MATERIAL AND METHODS
This was a prospective case-control study conducted over a period of 22 months (November 2006 to August 2008) at department of obstetrics and gynecology, Basaveshwar Teaching and General Hospital, and Sangameshwar Hospital attached to Mahadeveppa Rampure Medical College, Gulbarga. The study consists of analysis of pregnancy outcome in 50 antenatal women with the ultrasound diagnosis of oligohydramnios (AFI ≤ 5) at or beyond 34 weeks of gestation compared with 50 controls with normal liquor (AFI > 5 and < 25) matched for other variables like age, parity and gestational age. Method of Collection of data • Women who have had 3 or more antenatal visits were considered as booked cases. • For all cases selected, thorough history was taken and complete examination was done and clinical evidence of oligohydramnios was looked for.
• The previous obstetric records and ultrasound reports were reviewed.
• Gestational age was calculated from their date of last menstrual period or from their first trimester ultrasound report.
• 50 patients with ultrasound diagnosis of oligohydramnios (AFI ≤ 5) were included in the study group. Amniotic fluid index was calculated by four quadrant amniotic fluid volume measurement technique.
• Oligohydramnios was defined as amniotic fluid index ≤5cm. The amniotic fluid volume is considered normal if amniotic fluid index is between 5.1 and 25cm.
• For each case, a control was taken with similar age, gravidity, parity and gestational age with amniotic fluid index of more than 5cm and less than 25cm.
Inclusion Criteria
a. Women with any order of parity
b. Singleton pregnancy
c. Gestational age ≥ 34 weeks d. AFI ≤ 5cm
Exclusion criteria
a. Multiple gestation
b. Gestational age less than 34 weeks and >40 weeks
c. AFI > 5cm
d. Ruptured membrane e. Pregnancy induced hypertension
f. Congenital anomalies
All the pregnant women in the study who went into spontaneous labor were allowed to deliver irrespective of gestational age with continuous fetal heart rate monitoring. Women not in labor with the gestational age between 34–38 weeks were closely monitored with biweekly NST and BPP, until they went into spontaneous labor. If they failed to go into spontaneous labor, they were induced at 38wks with dinoprostone gel or oxytocin drip depending on the Bishop’s score. NST was done for all patients. Variable deceleration was considered significant if it was below 70 bpm persisting for >60 seconds. Those who developed significant variable, repetitive late deceleration or other omnious FHR pattern with or without meconium stained liquor which persisted in spite of corrective measures like change in maternal position, hydration, O2 inhalation and stopping oxytocin were diagnosed as fetal distress and delivered by LSCS or by instrumental vaginal delivery. Amnioinfusion was not done in our study. Women with malpresentation and other obstetric indications were directly taken for cesarean delivery. All newborns were attended by pediatricians and endotracheal intubations and suctioning were done if liquor is meconium stained. Various outcome measures recorded were: induced Vs spontaneous labor, nature of amniotic fluid, FHR tracings, mode of delivery, and indication for cesarean section or instrumental delivery, Apgar score at one minute and five minutes, birth weight, admission to neonatal ward, perinatal morbidity and mortality. Early neonatal death was defined as the death of a fetus whose birth weight was 1000 grams or more, within first seven days of life. Fetal distress was an ill defined term used to express intrauterine fetal jeopardy, resulting from intrauterine fetal hypoxia. Non reassuring fetal heart rate pattern, significant variable and repetitive late deceleration were considered as fetal distress. Apgar score: Five minute apgar score < 7 was considered abnormal. IUGR was defined as a birth weight of less than 10th centile for gestational age. Low birth weight was defined as birth weight less than 2.5 kg at term. Preterm was defined as gestational age <37 completed wks. Term was defined as gestational age more than 37 completed weeks.
RESULTS
The results were recorded and tabulated. The outcomes were statistically analyzed using parameters like standard deviation, chi square test and ‘Z’ test.
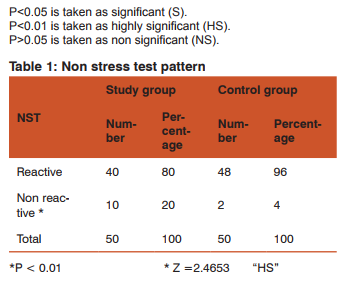
The non stress test was non reactive in 10 (20%) women of study group compared to only 2 (4%) in women of control group. There was highly significant difference between the two groups in occurrence of non reactive pattern. (P <0.01)
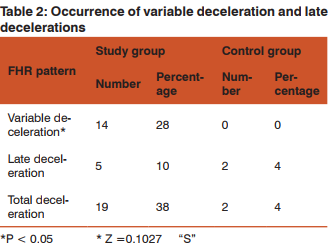
The most common fetal heart rate abnormality was variable deceleration. Variable deceleration was noted in 14 (28%) and late deceleration in 5(10%) of women in study group. In the control group no women developed variable deceleration and 2(4%) of women had late deceleration. There was significant difference in two groups in occurrence of variable deceleration (P < 0.05).
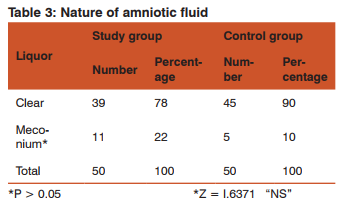
Amniotic fluid was meconium stained in 11 (22%) women in study group. In control group, only 5 (10%) women had meconium stained amniotic fluid. The difference in occurrence of meconium stained amniotic fluid between two groups was not statistically significant.
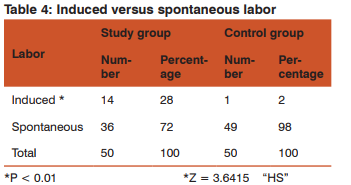
Labor was induced in 14 (28%) women in study group and 1 (2%) women in control group. More women in the study group were induced when compared to control group (P < 0.01).
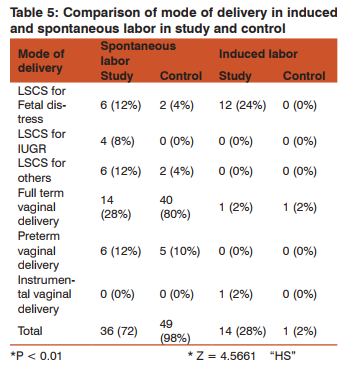
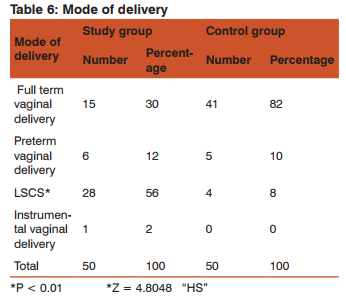
12 (24%) of induced women in study group had LSCS for fetal distress. Induction of labor in the study group resulted in increased incidence of fetal distress leading to cesarean delivery. Out of 14 (28%) induced, 12 (24%) had cesarean delivery and 1 (2%) landed up with vacuum delivery. Out of 28 cesarean delivery in the study group, 18 were done for fetal distress, 4 for IUGR and 2 for breech presentation, 2 for cephalo-pelvic disproportion and 1 for previous two cesarean delivery and 1 for persistent occipito-posterior position.
The mean apgar score for study group was 5.12 at 1min, 8.0 at 5min. The mean Apgar score for women in control group was 6.9 at 1 minute and 8.66 at 5min. 5 min Apgar < 7 was seen in 10% in study group and 4% in control group.
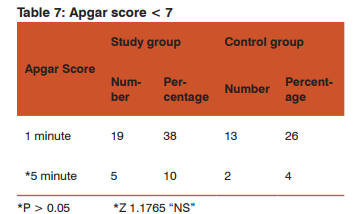
The difference in the occurrence of Apgar score < 7 at 5 min was not statistically significant between both groups.
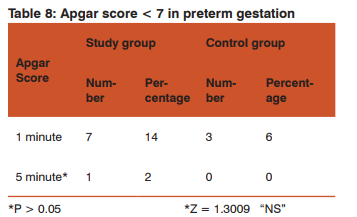
Agar score <7 at 5min was seen in 1 (2%) baby of study group with preterm gestation compared to 0 (0%) in control group which is not statistically significant.
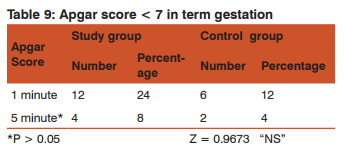
Apgar score < 7 at 5min was seen in 4 (8%) of study group with term gestation. There was no difference in the Apgar score < 7 at 5 minutes both preterm and term gestation
Apgar score < 7 at 5min was seen in 4 (8%) of study group with term gestation. There was no difference in the Apgar score < 7 at 5 minutes both preterm and term gestationtwo groups were statistically significant (P < 0.05).
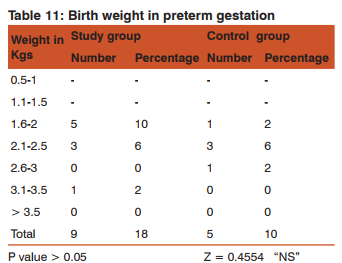
In preterm gestation 8 (16%) babies weighed < 2.5 kg in study group compared to 4 (8%) in the control group.
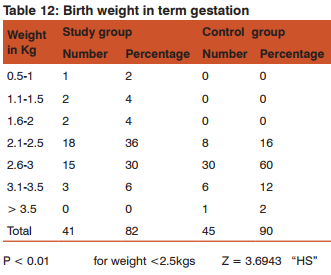
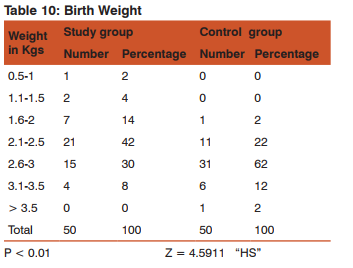
There were 23 (46%) low birth weight babies in study group, compared to 8 (16%) in the control group in term gestation. Difference in birth weight at term gestation between both groups is statistically significantly.
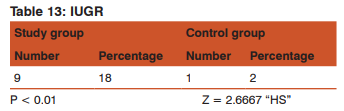
9 (18%) neonates in study group and 1 (2%) in control group were IUGR. The difference is statistically significantly P < 0.01.
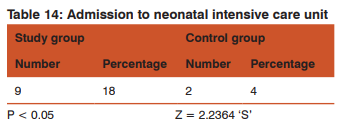
9 (18%) neonates of study group were admitted to neonatal ward for various morbidities like meconium aspiration, IUGR, preterm care, neonatal seizures, and birth asphyxia. Only 2 (4%) of control group were admitted to neonatal ward. The difference in two groups was statistically significant. There was no case of early neonatal death both in study and control group.
DISCUSSION
Amniotic fluid volume is now recognized as an important marker of fetal well being. When oligohydramnios is diagnosed, detailed examination of fetal anatomy, particularly renal tract must be under taken, and fetal growth parameters must be assessed to exclude fetal growth restriction.9 Doppler velocimetry of the umbilical artery must be performed and an increased S/D ratio in cases of oligohydramnios helps to identify fetus at risk, 80% of the fetus had an adverse perinatal outcome when the umbilical artery Doppler was abnormal.10 Infants born to women treated by amnioinfusion were significantly less likely to have meconium below the vocal cords and were less likely to develop meconium aspiration syndrome than infants not given amnioinfusion.11 Intravenous maternal hydration by infusing 2 liters of 5% dextrose water in 2 hours increase the AFV by 4.5cm (mean) in women with oligohydramnios as well as in those with normal AFV and may be beneficial in the management of oligohydramnios.12 Conway DL et al (2000) in a randomized clinical trial including 183 low risk women between 37 and 41 weeks gestation with < = 5cm ( patients with hypertension, rupture membranes, abnormal fetal testing, fetal growth restriction and fetal anomaly were excluded) found no significant difference in perinatal death, neonatal seizures meconium aspiration, fetal growth characteristics, route of delivery between two groups. He concluded that expectant management in otherwise normal pregnancy at term appears to be a reasonable alternative to labor induction.13 Ghosh G et al (2002) studied 333 parturients with oligohydramnios with intact membranes and found no significant difference in perinatal outcome in relationship to the amniotic fluid index, although a 50% increase in emergency operation for fetal distress was noted.14 Voxman EG (2002) studied antepartum testing records of 779 women with oligohydramnios ≤5 cm seen over 12 months period and found that AFI ≤ 5.0cm was significantly associated with an abnormal antepartum fetal heart rate tracing but not with cesarean delivery, meconium stained fluid, Apgar score < 7 or NICU admission.15 Zhang J et al (2004) examined fetal growth and perinatal outcomes in pregnancies with isolated oligohydramnios in 15,151 low risk pregnant women randomly assigned to ultrasound screening group or the control group. Oligohydramnios was diagnosed in 1.5% women with ultrasound screening compared with 0.8% among the controls. Approximately half of the oligohydramnios cases in the screening group were isolated with no clearly associated factors. Pregnancies with isolated oligohydramnios had perinatal out come similar to pregnancies with a normal amniotic fluid index.16 Locatelli A et al (2004), assessed prognostic values of amniotic fluid reduction by serial assessment of amniotic fluid index in uncomplicated term pregnancies in 3050 women and concluded that sonographic diagnosis of oligohydramnios carries an increased risk of adverse perinatal outcome even in low risk pregnancies after 40 weeks.17 Alchalabi HA et al (2006) in a study to determine the impact of the amniotic fluid index on the perinatal outcome of the patients admitted for induction of labor at term in 180 patient at 37-42 weeks gestation with unfavorable cervix and intact membranes found that meconium staining of the amniotic fluid was significantly higher in the group with AFI < 5cm and number of cesarean deliveries due to fetal distress was significantly higher. He concluded that induction of labor at term in patients with oligohydramnios is associated with an increased risk of cesarean delivery due to fetal distress.18 Manzanares S et al (2007) evaluated outcome of active induction of labor for isolated oligohydramnios in 412 singleton term low risk gestation and found that overall rate of cesarean deliveries and cesarean deliveries for non reassuring fetal status were higher in the oligohydramnios group than in control group. There was no difference between groups in neonatal outcome or perinatal morbidity or mortality.19 Danon D et al (2007) in a study evaluated the maternal and neonatal outcomes of 138 pregnancies complicated with isolated oligohydramnios at term managed by induction of labor and found that cesarean section rate was significantly higher in the induced group than the spontaneous labor group. He concluded that pregnancies with isolated oligohydramnios at term apparently are not at higher risk of perinatal complications, but induction of labor is associated with increased rate of cesarean delivery.20
CONCLUSION
Pregnancies with isolated oligohydramnios (AFI ≤ 5) at or beyond 34 weeks are associated with increased rate of non reactive NST, FHR deceleration during labor, development of fetal distress, rate of caesarean delivery and low birth weight. Rate of cesarean for fetal distress is increased because of increased rate of induction of labor in the women with oligohydramnios. Routine induction of labor for isolated oligohydramnios is not recommended. No appropriate route of delivery can be recommended by the study. It is preferable to allow patients to go into spontaneous labor with continuous fetal heart rate monitoring. Termination of pregnancy with oligohydramnios by caesarean delivery or instrumental vaginal delivery should be done at the onset of fetal distress. Antepartum diagnosis of oligohydramnios warrants close fetal surveillance.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from from where the literature for this article has been reviewed and discussed.
References:
1. Chamberlain PF, Manning FA, Morrison I, Harman CR, Lange IR. Ultrasound evaluation of amniotic fluid index. I. The relationship of marginal and decreased amniotic fluid volumes to perinatal outcome. Am J obstet Gynecol. 1984 Oct;150(3): 245-9.
2. Brace RA. Physiology of amniotic fluid volume regulation. Clin obstet Gynecol. 1997 Jun;40(2):280-289.
3. Wallenburg HC. The amniotic fluid I. Water and electrolyte homeostasis. J Perinat Med. 1977;5(5): 193-205.
4. Nicolini U, Fisk NM, Rodeck CH, Talbert DG, Wigglesworth JS. Low amniotic pressure in oligohydramnios-- is the cause of pulmonary hypoplasia? Am J Obstet Gyncol. 1989 Nov;161:1098-101.
5. Hill M. Oligohydramnios: Sonographic diagnosis and clinical implications. Clin obstet Gynecol. 1997 Jun; 40( 2):314-27.
6. Ott WJ. Reevaluation of the relationship between amniotic fluid volume and perinatal outcome. Am J Obstet Gynecol. 2005 Jun;192(6):1803-9.
7. Casey BM, McIntire DD, Bloom SL, Lucas MJ, Santos R, Twicker DM et L. Pregnancy outcome after antepartum di-agnosis of oligohydramnios at or beyond 34 weeks of gestation. Am J Obstet Gynecol. 2000 Apr; 182(4): 902-12.
8. Leeman L, Almond D. Isolated oligohydramnios at term: is induction indicated? J Fam Pract. 2005 Jan;54(1):25-32.
9. Halperin ME, Fong KW, Zalev AH et al. Reliability of amniotic fluid volume estimation from ultrasonogram ; intraobserver and interobserver variation before and after the establishment of criteria. Am J Obstet Gynecol. 1985 Oct;153(3):264-7.
10. Carroll BC, Burner JP. Umbilical artery Doppler Velocimetry in pregnancies complicated by oligohydramnios. J Reprod Med. 2000 Jul; 45(7):562-6.
11. Cunningham FG, Gant Norman F, Leveno KJ et al. Abnormalities of fetal membranes and amniotic fluid. Chapter 31 in William’s Obstetrics 21st edition, Mc Graw Hill 2001; 820-824.
12. Umber A, Chohan MA. Intravenous maternal hydration in third trimester oligohydramnios: effect on amniotic fluid volume. J Coll Physicians Surg Pak. 2007Jun;17(6):336-9.
13. Conway DL, Groth S, Adkins WB, Langer O. Management of isolated oligohydramnios in the term pregnancy: A randomized clinical trial. Am J Obstet Gynecol 2000;182:S21.
14. Ghosh G, Marsal K, Gudmundsson S. Amniotic fluid index in low risk pregnancy as an admission test to the labor ward. Acta Obstet Gynecol Scand. 2002;81(9): 852-5.
15. Voxman EG, Tran S, Wing DA. Low amniotic fluid index as a predictor of adverse perinatal outcome. J Perinatol. 2002 Jun;22(4):282-5.
16. Zhang J, Toendle J, Meikle S, Klebanoff MA, Rayburn WF. Isolated oligohydramnios is not assioated with adverse perinatal outcomes. BJOG. 2004 Mar;111(3);220-5.
17. Locatelli A, Zagarella A, Toso L, Assi F, Ghidini A, Biffi A. Serial assessment of amniotic fluid index in uncomplicated term pregnancies: prognostic value of amniotic fluid reduction. J Matern Fetal Neonatal Med. 2004 Apr;15(4):233-6.
18. Alchalabi HA, Obeidat BR, Jallad MF, Khader YS. Induction of labor and perinatal outcome: the impact of amniotic fluid index. Eur J Obstet Gynecol Reprod Biol. 2006 Dec;129(2):124-7.
19. Manzanares S, Carrillo MP, Gonzalez-Peran E, Puertas A, Montoya F. Isolated oligohydramnios in term pregnancy as an indication for induction of labour. J Matern Fetal Neonatal Med. 2007 Mar;20(3):221-4.
20. Danon D, Ben-Haroush A, Yogev Y, Bar J, Hod M, Pardo J. Prostaglandin E2 induction of labor for isolated oligohydramnios in women with unfavourable cervix at term. Fetal Diagn Ther. 2007;22(1):75-9.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





