IJCRR - 7(13), July, 2015
Pages: 29-34
Print Article
Download XML Download PDF
EVALUATION OF PSYCHIATRIC MORBIDITY IN THE COMMUNITY THROUGH APPLICATION OF
SCHEDULE FOR CLINICAL ASSESSMENT IN NEUROPSYCHIATRY (SCAN)
Author: P. K. Chaudhury, Dhrubajyoti Bhuyan
Category: Healthcare
Abstract:Background: Hospital based reports do not reflect prevalence of psychiatric morbidity in the community. Even the lack of knowledge and stigma associated with mental disorders cause hindrance to avail hospital services. Community based survey in a well defined sample is the right and appropriate approach for proper estimation of prevalence of such illnesses. Aims: To estimate the prevalence of psychiatric illnesses in the community and to study the socio demographic co-relates of the positive cases. Methods: 10% of participants from the pool of three thousand (3,000) respondents recruited for World Mental Health (WMH) Survey were selected, by using systemic random sampling method and psychopathology was tested by using the translated Assamese version of Schedule for Clinical Assessment in Neuropsychiatry (SCAN). Results: The prevalence of psychiatric morbidity in the community was found to be 13.18%, with Alcohol Use Disorder being the most common psychiatric morbidity.
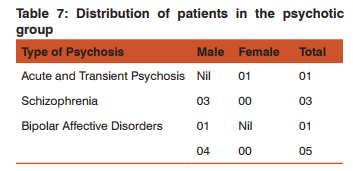
Conclusion: Alcohol Use Disorders are the commonest psychiatric morbidity (4.39%) in the study population followed by Depression (3.38%), Anxiety (1.69%) and Psychosis (1.69%). The figures reflect only the point prevalence of the diseases.
Keywords: Psychiatric morbidity, Clinical assessment, Composite international diagnostic interview
Full Text:
INTRODUCTION
Psychiatric conditions are a growing public health concern, – they are responsible for little more than 1% of deaths and accounts for about 11% of disease burden1 . Though psychiatric conditions are well known to impose a great burden to the sufferer, family and also to the society, mental health is still the most neglected portion of the spectrum of health2 . May be due to lack of awareness and associated social stigma, patients even if they are suffering for a longer period hesitate to present to psychiatrists3 . Therefore, what we see in the clinical setup is probably the tip of the iceberg; the actual problem may be much more greater than one can anticipate. So, proper evaluation of psychiatric morbidity is a necessity for any intervention to be taken. Although there are various instruments designed to study the epidemiology of mental illness in the community, like Diagnostic Interview Schedule (DIS) (1981) and Composite International Diagnostic Interview (CIDI) (1993), which can be used by trained non-mental health professionals, the results obtained by application of such instruments may not also be able to identify the actual magnitude of the illness. However, the diagnosis made by application of another sophisticated instrument called Schedule for Clinical Assessment in Neuropsychiatry (SCAN) adopted by WHO requires trained mental health professionals and is recognized as a valid and reliable instrument. Therefore the current study attempts to estimate the prevalence of psychiatric illnesses in the community through application of this instrument. This instrument was applied in its translated Assamese version to see its applicability and any technical problem in the administration in a small-defined population.
AIMS AND OBJECTIVES
The aims and objectives of the study are
1. To estimate the prevalence of mental disorders in the community.
2. To study the socio-demographic correlates of the positive cases.
METHODOLOGY
Sample Selection: The samples for the study were drawn from a predetermined sample for another study – The World Mental Health (WMH) Survey, conducted by the WHO. The WMH study was completed in the Department of Psychiatry, Assam Medical College and Hospital, Dibrugarh in the month of October 2004. This study has the advantage of having a meticulously worked out sample of 3000 households, which was made on the basis of sample proportion to size. From this pool of 3000 households the sample for our study was drawn by using systematic random sampling method (every 10th sample). The investigators were blind about the diagnostic status of the sample, which has already been evaluated by the WMH – CIDI in the study mentioned above.
Size of the Sample: We have selected a sample of Three hundred respondents by using the method mentioned above.
Inclusion Criteria: 1. Age: 18 years and above 2. Sex: Both sexes.
Exclusion Criteria: 1. Age: Below 18 years. 2. Respondents with chronic debilitating illness.
Instruments Used: Schedule for Clinical Assessment in Neuropsychiatry (SCAN): It is an instrument for assessing, measuring and classifying major psychiatric illnesses, It was developed in the framework of the World Health Organization and the National Institute of Health joint project on Diagnosis and Classification of Mental Disorders, Alcohol and Drug related problems. It consists of four parts:
1. The Tenth Edition of Present State Examination (PSE10)
2. The Glossary of Differential Definitions.
3. The Item Group Checklist (IGC)
4. Clinical History Schedule (CHS)
PSE 10 itself has two parts, Part I covers Somatoform, Dissociative, Anxiety, Depressive and bipolar disorders and problems associated with basic bodily functions and use of Alcohol and other Substance use, while Part II contains Psychotic and Cognitive disorders and observed abnormalities of speech, affect and behaviour. The instrument was translated into Assamese and adopted after testing the inter-rater reliability which was found to be of higher order.
Place of Study: The study was conducted in the rural and urban areas of Dibrugarh District having a total population of 2,08,548 households according to the 2001 census.
Procedure: The Study was undertaken after receiving ethical clearance of Institutional ethical committee of Assam Medical College and Hospital, Dibrugarh For the purpose of the study, a SCAN trainer who had been trained in New Delhi trained five PG students from the Department of Psychiatry, Assam Medical College and Hospital Dibrugarh. Informed consent was obtained from each respondent before evaluation. Those respondents suffering from debilitating systemic illness were excluded from the study. The diagnosis was obtained by using the diagnostic algorithm of SCAN.
RESULTS
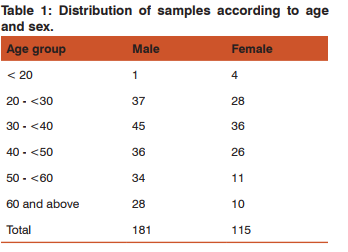
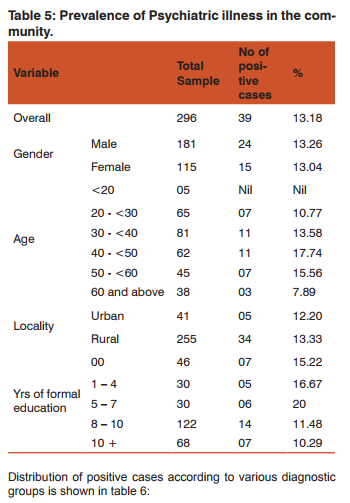
Though our original sample size was 300, 4 respondents were excluded from the study due to their debilitating physical illnesses as per the criteria. Therefore effective sample size reduced to (300 – 4) = 296. 181 male & 115 female respondents participated in the study and their age wise distribution is shown in table 1:
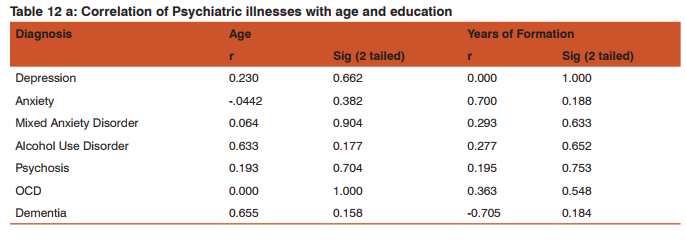
The study was conducted in both urban & rural areas of Dibrugarh District. As many as 255 ( 86.15%) respondents hailed from rural areas and only 41 (13.85%) were from urban area. This is depicted in table 2:
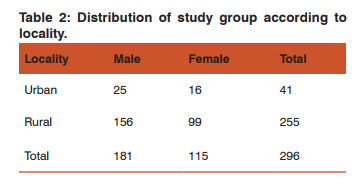
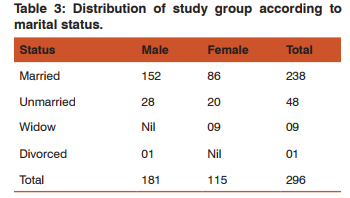
Table 3 shows marital status of the respondents participating in the study:
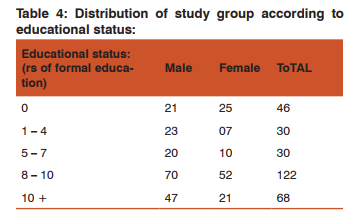
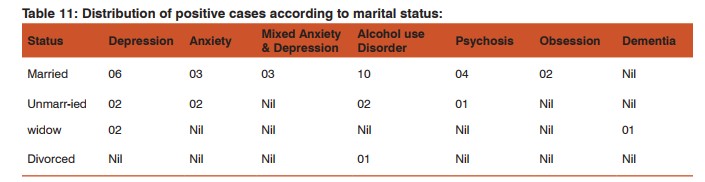
The educational status was measured in terms of years of formal education and the distribution of the samples according to this variable is shown in table 4:
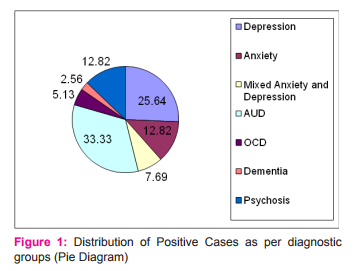
Our study shows 13.18% prevalence on psychiatric illnesses including mental and behavioural disorders due to use of alcohol. Alcohol related mental problems alone have the prevalence on 4.38% and this accounts for about 33.33% of the total psychiatric morbidity.
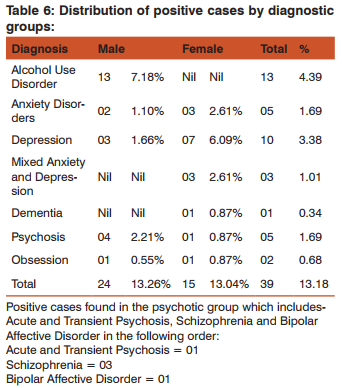
Alcohol related mental and behavioural problems accounts for about 33.33% of all the psychiatric morbidity followed by Depression, which accounts for about 25.64%, Anxiety and Psychosis each contributes to 12.82% of all psychiatric morbidity.
Data analysis:
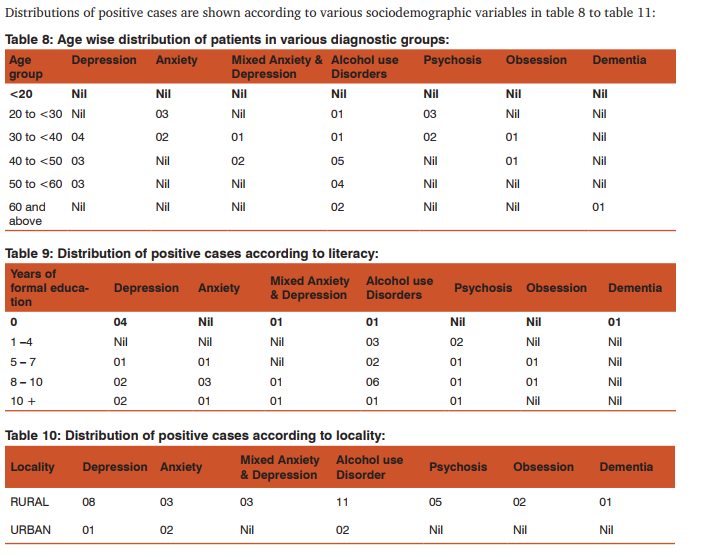
I. Analysis based on age wise distribution According to the statistical analysis based on age wise distribution of the positive cases the following results were obtained –
According to the statistical analysis co- relation between age and depression was found to be 0.230, which indicates that as the age increases the occurrence of Depression also increases and it its percentage of increment is 23%. Such type of positive co-relations were also found with Mixed Anxiety Depression, Alcohol Use Disorder, Psychosis and Dementia:
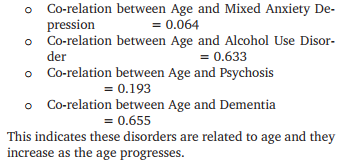
This indicates these disorders are related to age and they increase as the age progresses. However, a negative co-relation (-0.442) was found between Age and Anxiety indicating that as the Age increases prevalence of Anxiety decreases and its percentage of decrease is 44.2%, in other words Anxiety is more common in early adult ages. However, statistical analysis shows no linear co-relation between Age and Obsession. Positive co-relation was found between Years of Formal Education and Anxiety, the co-relation coefficient being 0.700. A negative co-relation of –0.705 was found between Years of Formal Education and Dementia. Obsession, Psychosis, Mixed Anxiety Depression and Alcohol Use Disorder also show a positive co-relation with literacy.
However, no co-relation was shown to occur between Years of Formal Education and Depression.
DISCUSSION
Our study shows point prevalence of 13.18% psychiatric illnesses including Alcohol Use Disorders, which is in keeping with the study- NIMH – Epidemiological Catchment Area (ECA) Programme (1984) conducted in USA, which showed 1-month prevalence of psychiatric illnesses being 15.14%4 . Alcohol Abuse and Dependence were found to be the most common psychiatric condition in this part of the country accounting for about 33.33% of all psychiatric illnesses. This is most common in males and incidentally we have not found any female alcoholic during our study, this was probably because we were handicapped with a small sample size. Depression was the second common psychiatric morbidity in the community and majority of the sufferers were the females. Though the sample size was small the detection of the cases with the help of SCAN was very meticulous and the results were in accordance with the other standard literature5,6,7. Though our study samples were drawn from the pool of respondents recruited for the WMH (World Mental Health) Survey which was done by using another instrument (CIDI) which was completed in the Department of Psychiatry, Assam Medical College, Dibrugarh during 2002 – 2004 with support from WHO and Ministry of Health, Government of India. The two results could not be compared as the data of the WMH Survey are under process of analysis at WHO headquarters, and results are yet to be published. Hopefully the two results may be compared once the WMH results are published.
Limitation:
1. Sample size was too small for a community-based study.
2. Burden of disease was not assessed.
3. Utilization of health services for various mental illnesses was not studied.
4. The study does not reflect the course of illness, as it was a cross-sectional study.
Conclusion
Epidemiological studies involving this type of sophisticated instrument are quite a few in the world and ours is one of its kinds in this part of the country. Although the sample size was small the case detection with the help of SCAN was very meticulous and the results were in accordance with the standard literature. The translated Assamese version of SCAN was found to be very useful and no technical problems during its application was met with. This study is expected to be a guide in the field of Community Based Study and inspire the future generation for a more comprehensive study in the field of Mental Health Disorders.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Murrey C J L and Lopez AD, Summary Global Burden of Disease and Injury Series Global Burden of Disease a comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020 The Harvard School of Public Health on Behalf of The World Health Organization And The World Bank.
2. WORLD HEALTH ORGANIZATION (2005) Mental health: facing the challenges, building solutions Report from the WHO European Ministerial Conference WHO Regional office for Europe Scherfigsvej 8 DK-2100 Copenhagen, Denmark.
3. Stier A and Hinshaw SP, (2007) Explicit and Implicit Stig- Stier A and Hinshaw SP, (2007) Explicit and Implicit Stigma Against Individuals With Mental Illness, Australian Psychologist 42(2), 106-117.
4. Eaton WW, Holzer CE, Von Korff M et al (1984): The Design Of The Epidemiologic Catchment Area Survey; Archives of General Psychiatry: 41: 942-948.
5. Regier DA, Myers JK, Kramer M et al (1984) The NIMH Epidemiologic Catchment Area Program; Archives of General Psychiatry: 41: 934-941.
6. Robbins LN, Helzer JE, Weissman MM et al (1984): Life- Robbins LN, Helzer JE, Weissman MM et al (1984): Lifetime Prevalence of Specific Psychiatric Disorders in Three Sites; Archives of General Psychiatry: 41:949-958.
7. Dr. Kulkarni AP and Dr. Baride J P (2002): Textbook of Community Medicine, 2nd Edition; Vora Medical Publication, Mumbai.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





