IJCRR - 7(13), July, 2015
Pages: 25-28
Print Article
Download XML Download PDF
UTERORECTAL FISTULA MANIFESTING DURING SECOND TRIMESTER OF PREGNANCY AS MASSIVE LOWER GASTROINTESTINAL BLEEDING: IS IT A MENACE OF MTP?
Author: Papa Dasari
Category: Healthcare
Abstract:A 27-year-old G2 A1 post IVF conception, DADC twins was hospitalized at 11 weeks with a diagnosis of threatened abortion.. History documented included that she conceived soon after marriage 5 years ago and underwent MTP by surgical method (D&E) at 8 weeks of pregnancy following which she suffered from secondary infertility. Laparoscopy for evaluation of secondary infertility a year ago revealed bilateral tubal block and she was treated with ATT for 6 months elsewhere. She conceived following second attempt of IVF. At admission, she had mild bleeding and USG confirmed DADC twins with good cardiac activity and the
placenta of the first twin was posterior encroaching Os and that of second twin was also posterior wall but near fundus of the uterus .She was managed conservatively with bed rest, progesterone support and psychological support. She expelled the first fetus at 16 weeks following 18 days of leaking. Conservative management was continued. At 20 weeks she developed leaking from the second sac and developed severe pain abdomen and acute gush of bleeding per rectum. USG revealed empty uterus and the fetus outside the uterus. Emergency laparotomy with a provisional diagnosis of spontaneous rupture uterus revealed a large rent on the posterior surface of uterus and anterior rectal wall and the fetus which was in the rectosigmoid was extracted by squeezing. There was a mucus fistula between the uterus and rectum. Uterine rent was closed and colostomy was done. She was discharged home with advice to opt for surrogacy or adoption.
Keywords: Medical termination of pregnancy, Secondary infertility, Bilateral tubal block, IVF, Acute gastrointestinal haemorrhage, Uterorectal fistula
Full Text:
INTRODUCTION
Enterouterine fistulae are very rare and around 58 cases were reported over 200 years prior to 19551 . In the later years 24 cases of colouterine fistulae were reported in English and French literature and these were due to diverticulitis in the non-pregnant state2 . Colouterine fistula presenting during pregnancy is so rare only 2 case reports are available. The following case is unique because of its clinical presentation as massive gastrointestinal bleeding during second trimester of twin pregnancy following IVF.
CASE REPORT
A 27 year old G2 A1 attended our emergency Obstetric services at 11+1 weeks of gestation with history of bleeding per vaginum of two weeks duration. Bleeding was moderate in amount and bright red in color and was not associated with pain abdomen. This pregnancy was achieved after the second attempt of IVF performed for bilateral tubal block at a private ART centre. She was on micronized progesterone support since then and it was a dichonionic and diamniotic pregnancy. Her past history revealed 5 years of secondary infertility following first trimester medical termination of pregnancy (MTP) by dilatation and evacuation (D&E) at a private hospital soon after marriage. She was investigated for secondary infertility after 4 years of MTP at another private hospital and was diagnosed to have bilateral tubal block after laparoscopy and was given ATT (Anti-Tubercular Treatment) empirically for six months.
On examination, she had no palor and was normotensive. Systemic examination was normal. Abdominal examination revealed 16 week size pregnant uterus. Per speculum examination showed minimal bleeding through os and on per vaginal examination cervix was 2 cms and os was closed. USG confirmed dichorionic diamniotic twins with good cardiac activity. CRL of twin A was 57.5 mm and twin B was 53.5 mms and the NTs were within normal limits. The placenta of twin A was posterior and was low in the cavity encroaching the OS. There was a small subchorionic hematoma. Twin B placenta was also in the posterior wall and up towards the fundus. She was hospitalised with a provisional diagnosis of threatened abortion and was managed conservatively with continued progesterone support and bed rest. Her initial investigations soon after admission were normal. Hb 11gm%; WBC 6,400 /cmm; urine culture and cervical swab culture were sterile. GTT and TFT were normal. She continued to have mild bleeding per vaginum with occasional pain abdomen and bouts of excessive bleeding and constipation on and off. She was given psychological support and required sedatives on and off. She developed leaking per vaginum 2 weeks after admission i.e., at 13+6 weeks of gestation. The first sac had no liquor and the fetus was alive but compressed. The patient was reassured and explained the possibility of spontaneous abortion/absorption of the first twin and conservative management was continued. Cervical swab culture and urine culture at this time revaled growth of E.Coli and she was treated with the sensitive antibiotic, injection Amikacin for 10 days. After 18 days of leaking pervaginum, the cord of the first fetus prolapsed and after 3 days she spontaneously expelled the placenta and the fetus. Conservative management was continued and she was receiving injection Proluton 500mg im weekly. Repeat Cervical swab culture did not grow any organisms. The follow up USG at 19 weeks revealed less liquor in the sac of the existing live fetus and after 2 days she complained of leaking per vaginum. At 19+6 weeks of gestation she had persistent pain abdomen not releived by sedatives and complained of fresh bleeding per vaginum in the midnight. She had tachycardia which progressively increased and her BP was maintained and after 4 hours she complained of sensation of passing stools and there was a gush of fresh blood on the bed. On perspeculum examination, there was minimal bleeding through cervix and Os was closed. At the end of examination, large fresh blood clot was expelled through the anus. After securing the iv access and starting intravenous fluids a gentle per rectal examination was performed which revealed a tear in the anterior rectal mucosa. Emergency surgical opinion was sought. Clinically they deferred regarding the rent in anterior rectal wall and performed anal packing with adrenaline soaked gauze. Immediate USG performed revealed empty uterine cavity and fetus lying transversely to the left of uterus. A provisional diagnosis of spontaneous rupture uterus was made and she was taken up for emergency laparotomy with General Surgeon back up after taking consent for hysterectomy and necessary procedure. At laparotomy there was 300 ml of haemoperitoneum, dense adhesions between bowel, omentum and fundus of uterus. There was a large 12x12 cm irregular rent in the posterior wall of uterus. Placenta was partially extruding through the rent and morbidly adherent to the edges. Fetus was contained wholly inside the rectum. (Fig. 1)
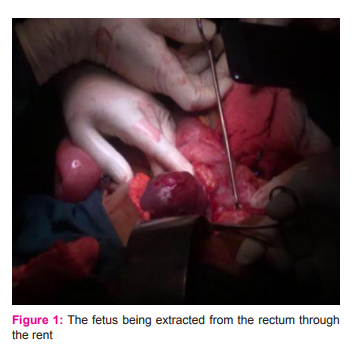
There was a large rent 6x6cm with irregular margins involving more than 3/4th of the luminal circumference of the lower sigmoid and rectum. There was a mucus fistula approximately 10 cm. There was a solid mass of 4x4 cm in the right ovary which was adherent to the right cornu of uterus. Right tube agglutinated and was adherent to the right lateral pelvic wall. Left fallopian tube and ovary agglutinated and fixed to left broad ligament. The fetus was extracted enmass by gentle traction and squeezing of the rectosigmoid. (Fig. 2). The uterine rent was closed in two layers with inturupted sutures using chromic catgut. Defunctioning Colostomy was performed by the Surgeons and the rent in the rectum was closed transversely with interrupted 2-0 vicryl sutures. Omentum was interposed between the rectal suture line and uterus. The mass in the right ovary was excised and the cut section revealed sebacious material with hair. Saline wash was given. Intraperitoneal drain was kept. Abdomen was closed enmass with continuous No.1 PDS. She received 4 units of packed cells and 4 FFPs. Postoperatively she was on intravenous fluids and nil per oral for 72 hours and was on intravenous antibiotics and the drain was removed after 5 days. She had febrile spikes for 10 days and workup for sepsis revealed again colonization of E. coli in cervical swab. Wound swab culture and blood culture were sterile. She was treated with injection Meropenum. Sutures were removed on day 15 and she was discharged after explaining the risks of contemplating pregnancy again and with advice to follow up in Surgery OPD for colostomy care and closure. She was counseled for adoption / surrogacy and advised against conception under any circumstances.

DISCUSSION
The common causes of bleeding per rectum during pregnancy include hemorrhoids, fissure in ano and rectal polyps.. Rare causes are arteriovenous malformations, intussusceptions, enteric fever, tuberculosis etc. A rare case of acute lower gastrointestinal hemorrhage due to ectopic pregnancy eroding the colon was misdiagnosed preoperatively as choriocarcinoma and enema prior to colonoscopy to rule out colonic causes induced massive hemorrhage and the women died of sepsis after laparotomy3 . Uterorectal fistula can also present with bleeding during menstruation (menochezia)4 in the non-pregnant state and with chorioamnionitis and post-abortal bleeding during pregnancy5 . The present case did not have history suggestive of menochezia. Massive gastrointestinal bleeding leading to shock due to uterorectal fistula during pregnancy is not found in literature search. The common causes of uterorectal fistula are diverticulitis and malignancies and rarely endometriosis. The other rare causes are radiation injury, perforation involving uterus and bowel during dilataion and curettage, pelvic surgery and polypectomy2 etc., Obstetric injury leading to enterouterine fistula was reported as the most common etiology prior to 19551 Of the causes injury due to curette was responsible for the fistulae in good number of cases and the clinical manifestations occur after few days to few months. In the present case there was history of curettage in her first pregnancy when she underwent surgical abortion and however there was no history suggestive of menochezia following this. Colouterine fistula due to endometriosis involving caecum presented during pregnancy with sepsis and biochemical DIC at 16 weeks of gestation. She needed subtotal hysterectomy and resection and anastamosis of bowel to save life because of severe uterine sepsis.5 A case of enterouterine fistula presented with recurrent early pregnancy and chorioamnionitis. She had spontaneous abortion and suffered from malena on the second post abortal day of her third pregnancy. Later she underwent laparotomy and an ileouterine fistula was found along with a piece of cartilage. The authors concluded that this fistula was due to the cartilage which she swallowed as there was no history of instrumentation of uterus in her previous pregnancy losses. In both the above cases and the present case of ours intermittent pain abdomen was present and sepsis was evident. In the present case sepsis was due to colouterine fistula and not ascending infection as her cervico- vaginal swab was sterile on admission and later after rupture of the first sac Escherichia coli was grown.
CONCLUSION
Uterorectal fistula due to uterine perforation that occurred long ago can manifest during subsequent pregnancy and the symptoms mimick those of threatened abortion. One of the acute manifestations can be sudden episode of bleeding per rectum. Closure of uterine perforation at the time of its occurrence should be undertaken to prevent fistula.
ACKNOWLEDGEMENT
I would like to acknowledge the help rendered by Dr. Manikandan, Associate Professor, Dept of Obstetrics and Gynaecology, Dr. Nandakishore, Associate professor, Department of general Surgey for the emergency laparotomy I also acknowledge all the authors of the references which I mentioned as the learning resources. They are of immense help to me to understand and write this case report.
References:
1. Martin DH, Hixson CH and Wilson EC. Enterouterine fistula. Obstet Gynecol. 1956; 7:466-469.
2. Uzan J,Koskas M, Fournier P, Marguiles AL, Luton D,Yazbeck C. Colouterine fistula after polymyomectomy: a Case report. Journal of Medical Case Reports. 2014, 8:199-202.
3. Ekwaro L,Kizza PM, Nassali G,Lubega J. Ectopic pregnancy: Unusual cause of lower GIT bleeding. A Case report East and Central African Journal of Surgery, 2004; 9: 5-7
4. P Pinto, L Sharma, P.Kini Chronic uterorectal fistula with menochezia and amenorrhea. IJGO.1990;
5. Siganeshan V, Willis IH, Zarate LA,Howard L,Robinson MJ. Colouterine fistula secondary to endometriosis with associated chorioamnionitis. Obstet Gynecol 2006; 107:451–3
6. Shaw FM, Renius JF, Leiken EL, Tejani N. Recurrent chorioamnionitis and second trimester abortion because of an enterouterine fistula. Obstet Gynecol.1995;86:639-641.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





