IJCRR - 7(13), July, 2015
Pages: 22-24
Print Article
Download XML Download PDF
CHRONIC TELOGEN EFFLUVIUM - A SHORT REVIEW
Author: Shashikant, Veeresh Dyavannanavar, Sidramappa R. Warad
Category: Healthcare
Abstract:Diffuse hair loss is a common complaint which dermatologists can come across in daily clinical practice. Women present more frequently with this complaint. Chronic telogen effluvium is a diffuse, generalized form of hair loss of unknown cause which is common in middle aged women. It often starts abruptly and is alarming to the patient as large number of hair are shed.
Keywords: Hair loss, Chronic telogen effluvium
Full Text:
INTRODUCTION
Chronic telogen effluvium (CTE) was first described by Whiting DA in 1996.1 It is characterized by an abrupt onset of diffuse hair loss of scalp persisting for more than six months. This condition predominantly affects healthy women in their fourth to fifth decade of life.2 It may be primary chronic telogen effluvium or may be secondary to various causes.3
Epidemiology
The exact incidence of CTE is not known. Garcia-Hernandez MJ reported an incidence of 67% in post-menopausal women out of 109 females of CTE.4
Etiopathogenesis
Most cases of CTE are primary or idiopathic. However, it may also occur secondary to various systemic causes. Various causes of secondary CTE areas follows:
- Iron deficiency. - Hypothyroidism and hyperthyroidism.
- Protein energy malnutrition.
- Zinc deficiency.
- Chronic renal failure.
- Liver failure.
- Systemic lupus erythematosus and other connec
- Systemic lupus erythematosus and other connective tissue disorders.
- Drugs (Heparin, colchicine, methotrexate)5,6
- Diabetes mellitus.5
Iron deficiency is the most common cause one can come across as compared to others.6 The exact pathogenesis of chronic telogen effluvium is uncertain, but it may be due to shortening of the anagen phase of the hair cycle without miniaturization of hair follicles, synchronization phenomena of the hair cycle or premature teloptosis.1,3,6 It has been suggested that shedding is not noticeable until the length of anagen phase is reduced by 50%, with a subsequent doubling of telogen hair. The patient should be assured that this type of shedding will not lead to baldness.6,7
Clinical features
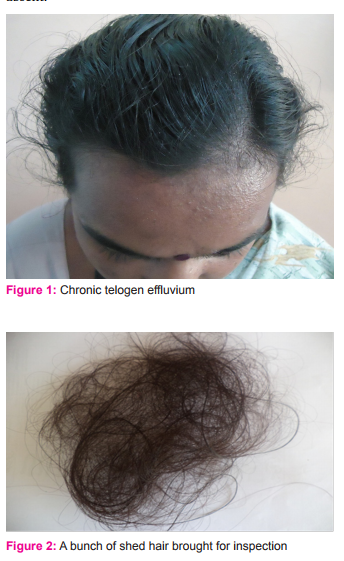
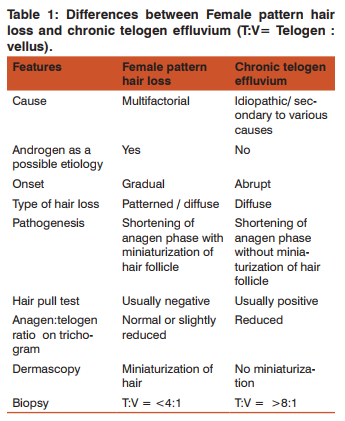
Chronic telogen effluvium may be triggered by an acute telogen effluvium. In primary CTE no specific triggering agent is evident. It predominantly affects women.6 The presentation of this type of hair loss tends to be distinctive.6 The typical patient is an otherwise healthy woman between 30 to 50 years with dense scalp hair (figure 1).1,6,8 It is characterized by abrupt, excessive, alarming, diffuse shedding of hair that runs a fluctuating course over several years.1,6,8 Patient often gives history of long hair during childhood, suggestive of a long anagen phase, and they report a high density of hair prior to the onset of hair loss.8 Patients insist that previously they had more hair and are distressed by the prospect of going bald. Many patients frequently bring large ball of hair for showing to clinician. However, no clinically obvious finding can be established. This condition tends to run a fluctuating course, at times reflecting seasonal periodicity in the growth and shedding of the hair with a maximal proportion of telogen hair at the end of summer and beginning of autumn. In the long run, the disorder appears to be self-limiting. It is of importance to reassure the patients that this condition represents exaggerated shedding rather than actual hair loss.6 Chunks of hair are usually seen in the bathroom, pillow, hair brush and comb. Usually patients will display a hand-full of hair to corroborate the complaint of excessive shedding (figure 2). Thinning of hair is not a feature of CTE, though many women do notice 50% reduction in ponytail thickness. Family history of androgenetic alopecia is usually absent.8
On examination moderate to severe bitemporal recession may be seen.1 There is no widening of the central part, as common in androgenetic alopecia. Hair pull test is usually positive over the vertex and occipital scalp.8 Diagnosis of CTE cannot be excluded by one single negative hair pull test.8 If the insult is prolonged and/or regularly repeated, it results in diagnostic difficulty.3 Investigation Histopathological picture is normal except for a slight increase in the telogen hair follicles.1 To exclude androgenetic alopecia scalp biopsy is usually required.3 The biopsy should be at the level of sebaceous gland.9 Normal terminal to vellus hair ratio is 7:1. A ratio of more than 8:1 is considered as diagnostic of CTE.9 In a study conducted by Sinclair R in 2002, out of 305 women with chronic diffuse hair loss, 54(18%) were diagnosed as CTE, 181(59%) were as FPHL and 70(23%) showed intermediate features on single horizontal biopsy.10 Iron deficiency has been reported in majority of women complaining of diffuse hair loss, but this probably has been overestimated.
Differential diagnosis:
Acute telogen effluvium and female pattern hair loss (FPHL) are important differential diagnosis of CTE. It can be differentiated with acute telogen effluvium by its long and fluctuating course. Differences between CTE and FPHL are mentioned in table 1.
Treatment
If a particular cause for chronic telogen effluvium is identified, such as hypothyroidism or iron deficiency, then suitable treatment should be given. If any drug is under suspicion as the cause of hair loss, then the patient should be advised to stop taking that drug, or that has to be substituted with an alternate drug which has lesser risk of causing hair loss. If the diet is inadequate, then it should be rectified.11 It is said that CTE is a self-limiting process, which may resolve spontaneously in 3-10 years, but there is no evidence to substantiate this assertion.1 Patient is usually anxious to have some form of treatment.11 The natural history of CTE is poorly characterized and the prognosis is less certain.1 No specific drug is available for the treatment of CTE. Topical minoxidil 2% has been suggested in anticipation that it will prolong anagen growth.1
CONCLUSION
It is a diffuse hair loss of scalp persisting for more than six months. This condition predominantly affects healthy women in their fourth to fifth decade of life. Most cases are primary. Patients with CTE can however be reassured that the condition is non-progressive and self-limiting.
ACKNOWLEDGEMENT
We acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. We are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Shrivastava SB. Diffuse hair loss in adult female: approach to diagnosis and management. Indian J Dermatol VenereolLeprol 2009;75:20-31.
2. Wadhwa SL, Khopkar U, Nischal KC. Hair and scalp disor- Wadhwa SL, Khopkar U, Nischal KC. Hair and scalp disorders. In: Valia RG, Valia AR, editors. IADVL Text book of dermatology, 3rd edn. Mumbai: Bhalani Publishing House; 2010.p.- 864-948.
3. Sinclair R. Diffuse hair loss. Int J Dermatol 1999;38:1-18.
4. Garcia-Hernandez MJ, Camacho FM. Chronic telogen ef- Garcia-Hernandez MJ, Camacho FM. Chronic telogen effluvium: incidence, clinical and biochemical features, and treatment. Arch Dermatol 1999;135:1123-1124.
5. Steinberg S, Ezers IA. Alopecia in women. Can Fam Physi- Steinberg S, Ezers IA. Alopecia in women. Can Fam Physician 1970;64-66.
6. Trueb RM. Diffuse hair loss. In: Blume-Peytavi U, Tosti A, Whiting DA, Trueb R, editors. Hair growth and disorders, 1st edn. Berlin: Springer; 2008.p.-259-272.
7. Chartier MB, Hoss DM, Grant-Kels JM. Approach to the adult female patient with diffuse nonscarring alopecia. J Am AcadDermatol 2002;47:818-820.
8. Messenger AG, Berker DA, Sinclair RD. Disorders of hair. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook’s text book of dermatology, 8th edn. Oxford: Blackwell Publishing; 2010.p.- 66.1-66.100.
9. Dhurat R, Saraogi P. Hair evaluation methods: Merits and demerits. Int J Trichology 2009;1:108-119.
10. Sinclair R, Jolley D, Mallari R, Magee J. The reliability of horizontally sectioned scalp biopsies in the diagnosis of chronic diffuse telogen hair loss in women. J Am AcadDermatol 2004;51:189-199.
11. Whiting DA. Chronic telogen effluvium. Dermatol Clin 1996;14:723-731.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





