IJCRR - 7(13), July, 2015
Pages: 19-21
Print Article
Download XML Download PDF
ELONGATED STYLOID PROCESSES OF HUMAN DRIED SKULLS OSTEOLOGICAL STUDY - RESEARCH ARTICLE
Author: Raju Sugavasi, Moula Akbar Basha
Category: Healthcare
Abstract:Existence of abnormal elongated styloid process is rare, traumatic fractures of this may entrap the neurovascular structures anatomically surrounding it. Aim: We conducted an osteological study in 100 human dried skulls to find out elongated styloid process, Results: found only one unusual case of elongated styloid processes situated bilaterally. Conclusion: Awareness on this kind of bilateral variation is useful to the surgeons for better diagnosis and treatment.
Keywords: Styloid processes, Elongation, Skull
Full Text:
INTRODUCTION
Styloid process is a slender bony projection extending from anterio inferior aspect of the temporal bone, with an average length of 2.5 cm. Anteriolateral surface of the base of styloid process is ensheathed by tympanic plate and distal part is attached by muscles and ligaments. The process is covered laterally by parotid gland, stylohyoid ligament connects tip to the lesser horn of hyoid bone. Styloglossus, stylopharyngeus and stylohyoid muscles take origin from anterior, medial surface and the tip in respect to Styloid process. The facial nerve crosses the base and external carotid artery crosses the tip of styloid process within the parotid gland (Gray’s) [1]. The symptoms, diagnosis and treatment associated to abnormal elongated styloid process were first described by eagle (Eagle, 1962) [2]. The normal length of Styloid process is 5 to 50 mm, but according to some authors more than 30 mm length was considered as elongated styloid processes (Skrzat et al, 2007) [3].
MATERIALS AND METHODS
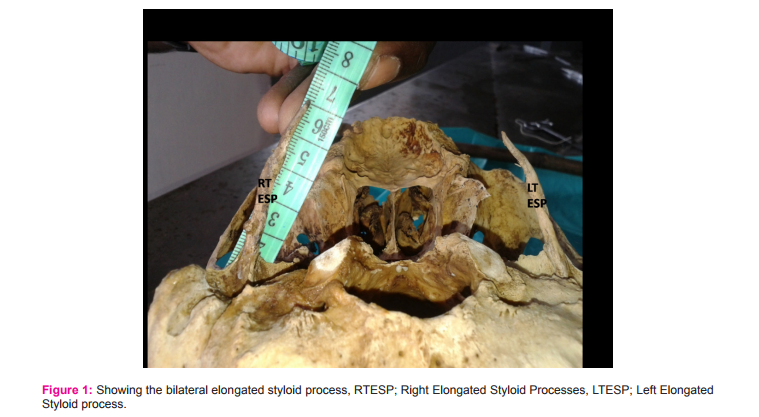
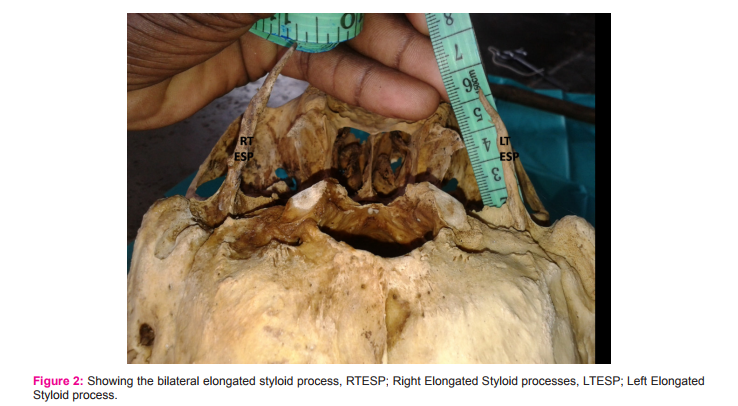
The present study was conducted in Osteology section of department of anatomy at Rajiv Gandhi institute of medical sciences (RIMS), Kadapa, Fathima Institute of Medical sciences (FIMS), Kadapa and Viswabharathi Medical College Kurnool, Andhra Pradesh, India. In this present osteological study we were searched for elongated styloid process in 100 human dried skulls but we found bilaterally elongated styloid processes in only one skull. The measurements were taken from base to tip by measuring tape and the length of styloid process was 6.5 cm on right side and 5.9 cm on left side (Figure 1 and Figure 2). These processes were extending downwards forwards but with more of medial deviation, which may aggravate the symptoms. Existence of bilateral variation of elongated styloid process is very rare, but has much clinical significance.
RESULTS
The present osteological study was found only one unusual case of elongated styloid processes on either side bilaterally among 100 dried human skulls. The incidence of existing variation is 1%.
DISCUSSION
The styloid process is derived from the second branchial arch. Apex of the styloid process and lesser cornu of hyoid bone are connected by stylohyoid ligament. This ligament represents as continuation of the styloid processes apex embryologically, styloid processes, lesser cornu of hyoid bone, stylohyoid ligaments are called as styloid chain (Reichert’s cartilage), and the whole chain derives from four cartilages embryologicaly, tympanohyale, stylohyale, ceratohyale, and hypohyale (Standing S., 2004) [4].
The styloid process is generally composed of dense connective tissue but may retain its embryonic cartilage and the possible for ossification (Rodriguez Vazquez JF et al, 2006) [5]. There are many cases of unilateral elongated styloid processes already previously reported, so the presence of the above said is very frequent (Scaf et al, 2003) [6]. Bilateral variation reported in the present case is rare as there were only few authors who reported it, that too recently. (Rathee et al, 2010) [7] reported it in 50 yrs old female by MRI scan (Length was 3.8 cm on right and 4 cm on left side), According to (Sanjeev iranna kolagi et al, 2010) [8] the total length of process is 8 cm and (Padeyappanavar KV et al, 2010) [9] the incidence was 3 out of 40 skulls. (Cawich et al, 2009) [10] reported bilateral elongation was seen in 75% of cases and occurrence was four times more in males than females. Various studies and theories were proposed for the occurrence of elongated styloid processes. According to (Camarda et al, 1989 and Ferrario et al, 1990) [11] ossification of stylohyoid ligament may lead to this asymptomatic variation although frequency varies (2-4% to 84.4 %). According to (Murtagh et al, 2001) [12] elongated styloid process was due to persistence of stylohyal cartilage, calcification of stylohyoid ligament and abnormal growth of bony tissue at the insertion of stylohyoid ligament. According to (Langlais et al, 1986 and Gossman et al, 1977) [13] elongated styloid process may produce symptoms like throat pain, foreign body sensation in the pharynx, otalgia, headache, dysphasia, pain while rotation of neck, , vertigo, syncope and facial pain. It also reduces the range of mandibular opening, changes the voice and taste with hyper salivation. Fracture of ossified stylohyoid ligament due to trauma or spontaneous is one of the causes for symptoms, only nine such cases were reported so far according to (Blomgren et al, 1999) [14].
CONCLUSION
Bilateral elongated styloid processes of human dried skulls were rarely present, so traumatic fractures of this may entrap the neurovascular structures anatomically surrounding it. Awareness on this kind of bilateral variation is useful to the surgeons to improve the diagnosis and treatment.
ACKNOWLEDGEMENTS
The authors are grateful to previous publishers of all those articles, journals and books from where the present literature has gathered and also for technical support.
References:
1. Standing S. Gray’s Anatomy. 2005. The Anatomical basis of clinical practice. 39th Ed Skull and Mandible. Edinburg. Elsevier Churchill Livingstone: 470.
2. Eagle WW. 1962. The symptoms, diagnosis, and treatment of elongated styloid process. Am Surgery, 28:1-5.
3. Skrzat J, Mroz I, Walocha J, Zawilinski J, Jaworek JK. 2007. Bilateral ossification of the stylohyoid ligament. Folia Morphol. 66(3):203-206.
4. Standing S. Gray’s Anatomy. 2005. The Anatomical basis of clinical practice. 39th Ed Skull and Mandible. Edinburg. Elsevier Churchill Livingstone: 470.
5. Rodriguez-Vazquez JF, Merida-Velasco JR, Verdugo-Lopez S, Sanchez-Montesinos I, Merida-Velasco JA. 2006. Morphogenesis of the second pharyngeal arch cartilage (Reichert’s cartilage) in human embryos. J Anat. 208: 179–189.
6. Scaf G, de Freitas DQ, de Castro Monteiro Loffredo L. 2003. Diagnostic reproducibility of the elongated styloid process. J Appl Oral Sci. 11: 120–124.
7. M. Rathee, A. Hooda, S.P.S. Yadav, J.S. Gulia. 2010. Bilateral Elongated Styloid Process: A Case Report and Review of Literature. The Internet Journal of Otorhinolaryngology. 12 (1). DOI: 10.5580/902.
8. Sanjeev iranna kolagi, Anita Herur, Ashwini Mutalik. 2010. Elongated styloid process – report of two rare cases. International Journal of Anatomical Variations. 3: 100–102.
9. Kiran V.Padeyappanavar, P.S. Bhusareddy and A.S. ?agaleekar.2010. Case Report on Elongated Styloid Process. Al Ameen J Med Sci. 3(1):99-101.
10. Cawich SO, Gardner M, Shetty R, Harding HE. 2009. A post mortem study of elongated styloid processes in a Jamaican population. The Internet Journal of Biological Anthropology; (3):1.
11. Camarda AJ, Deschamps C, Forest D. 1989. Stylohyoid chain ossification: A discussion of etiology. Oral Surg Oral Med Oral Pathol . 67: 512-520.
12. Murtagh RD, Caracciolo JT, Fernandez G. 2001. CT findings associated with eagle syndrome. AJNR Am J Neuroradiol. 22: 1401–1402.
13. Langlais RP, Miles DA, Van Dis ML. 1986. Elongated and mineralized stylohyoid complex: A proposed classification and report of a case of Eagle’s syndrome. Oral Surg Oral Med Oral Pathol. 61: 527-532.
14. Blomgren K, Qvarnberg Y, Valtonen H. 1999. Spontaneous fracture of an ossified Stylohyoid ligament. Journal of Laryngology and Otology. 113:854-855.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





