IJCRR - 7(13), July, 2015
Pages: 09-11
Print Article
Download XML Download PDF
DIAGNOSTIC DILEMMA IN RING ENHANCING LESION- A CASE REPORT
Author: Sahid Imam Mallick, Auriom Kar, Arijit Samanta, Soumava Mukherjee, Sneha Jatan Bothra, Roshni Dasgupta, Ritwik Ghosal, N.B. Debnath
Category: Healthcare
Abstract:Here we report a 22 years old boy with fever, headache and signs of meningitis with CT scan of brain showing multiple small enhancing lesion with minimal perilesional edema seen on both sides of cerebral cortex which was initially thought to be neurocysticercosis (NCC), but diagnosed subsequently to be tuberculomas by Magnetic Resonance (MR) spectroscopy and was subsequently treated with antitubercular drugs. This case report highlights the role of strong clinical suspicion and MR spectroscopy in the conformation of diagnosis of ring enhanced lesions.
Keywords: Neurocysticercosis, Tuberculoma, Ring enhancing lesion, MR spectroscopy.
Full Text:
INTRODUCTION
Neurocysticercosis (NCC) is the most frequent parasitic infestation of CNS in the world. Also cysticercal meningitis is very difficult to distinguish from tuberculomas associated with meningitis, the two most common causes of inflammatory granulomas encountered in clinical practise and differentiation between the two is very difficult and defied conventional investigations1,2. We highlight the importance of strong clinical suspicion and MR spectroscopy in differentiating the lesions. This distinction is important because parenchymal cysticercosis is benign and self limiting condition, but tuberculomas are active infection requiring prolonged therapy that involves potentially toxic drugs.
CASE REPORT
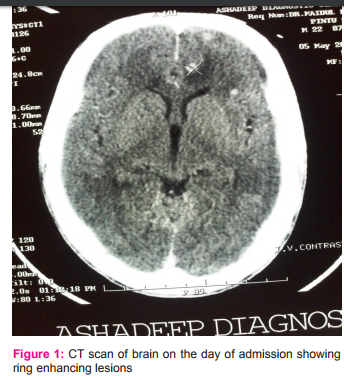
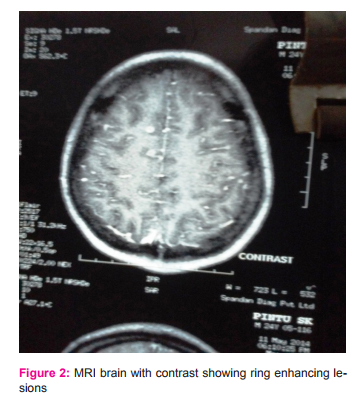
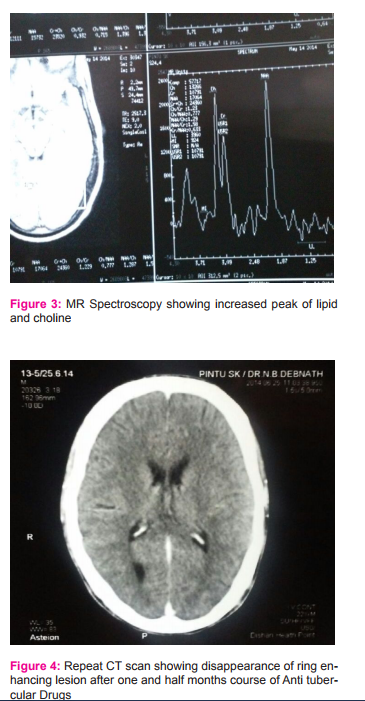
A 21 years old boy presented with 1 month history of low grade continuous fever with frontal headache and vomiting. His symptoms increased over time and gradually became irritable with subsequent drowsiness 4 days prior to hospitalization. He did not have any episode of convulsion during this 1 month period of illness. History of contact with tuberculosis was absent. On examination he was drowsy, febrile, apart from tachycardia vital was stable. Neurological examination was positive for meningeal signs without focal neurological deficits. Other systemic examinations were normal. Chest X-Ray was normal, mantoux test was negative, serology for cysticercal antigen was negative. CT scan revealed presence of multiple small enhancing nodular lesions with minimal perilesional edema seen in both the sides of cerebral cortex, suggestive of neurocysticercosis, there was no evidence of midline shift. On ophthalmological examination there was no papillaedema, or intraocular cysticercal parasite.MRI with contrast was done which showed extensive tiny ring and nodular enhancing focal lesions with mild to moderate perilesional odema scattered in cerebral hemispheres, cerebellum and right thalamic region and mild patchy irregular enhancement in basal cisterns and few cortical sulci of both cerebral hemispheres. Till now diagnostic dilemma persisted between NCC and tuberculoma so CSF was done which showed wbc-120/mm3 with 60% neutrophil and 40% lymphocyte, protein-151mg/dl, glucose-11mg/dl, cl—94m/dl ADA was normal. TBPCR, gram stain, AFB and Indian ink stain was negative. Patient clinical condition deterioted and he became comatose. ATD (HRZE) with steroid was empirically started and MRI spectroscopy was planned, which subsequently identified lipid lactate peaks within the lesions and diagnosis of tuberculoma was considered. In the meanwhile patient responded to treatment, his conscious level improved and was ultimately discharged with ATD and steroid, and advised to follow-up in OPD. After 6 weeks CT scan was done which showed disappearance of many lesions.
DISCUSSION
The diagnostic dilemma of inflammatory granuloma and the use of MR spectroscopy to diagnose tuberculoma and importance of starting ATD early on strong clinical suspicion are highlighted from the above case. Common causes of inflammatory granuloma includes neurocysticercosis, followed by tuberculosis, toxoplasmosis, cerebral abscess, fungal lesion.3 This boy presented with fever, headache, along with meningeal signs with neuroimaging suggestive of neurocysticercosis, all lesions ≤20 mm in size with regular outline and no midline shift. Yet the patient was actually having tubercular granulomatous lesion where we expect ≥20mm lesions with irregular outline and midline shift4 . The deterioting clinical condition of our patient prompted us to review our diagnosis on following facts. NCC commonly present with seizures5, 6, but there was no seizures in our patient. Fever is also present rarely in NCC. Also in several studies it was shown that cysticercal meningitis lacks nuchal rigidity5 . Several diagnostic criteria for NCC has been proposed but none of the criteria has addressed the differentiation between cysticercal granuloma and tuberculoma and this is the most difficult clinical situation a clinician face in developing country like India. Also positive serological test may help to confirm the diagnosis of cysticercosis but negative result does not exclude it7. Here MR spectroscopy may be helpful to differentiate tuberculoma from NCC. In a study by Pretell et all8 MR spectroscopy was used to differentiate single enhancing brain lesions as due to tuberculomas or NCC, tuberculomas has ↑peak of lipids, more choline and less NAA.
CONCLUSION
CNS tuberculomas with tubercular meningitis has a very similar presentation like cysticercal meningitis and differentiating between two is difficult in our country, where both are endemic. With increase in incidence of HIV, coinfection rates have also increased. Clinical examination directed to find evidence of tuberculosis and cysticercosis elsewhere is invaluable, but when absent creates a great diagnostic dilemma. CT scan and MRI can differentiate but again are not confirmatory as in our case. So to conclude, in such case where there is a high index of suspicion, MR spectroscopy may be a non-invasive alternative to determine their etiology.
ACKNOWLEDGEMENTS
The authors like to acknowledge the help rendered by department of General Medicine and also Dr. S.P. Saha, Professor and Head of the Department of Neurology. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Clinicoradiological and pathological correlation in patient with cysticercal granuloma and epilepsy with focus on presence of parasite and edema formation. Vedantan Rajshekar, Geeta Chako et al.
2. Single enhancing ct detected lesion in immunocompetent patients. Ravindra Kumar Garg, M.D, DM neurosurg focus 2002,12 (6)
3. Sethi PP, Wadia Rd, Kiyawat DP, et al ring or disc enhancing lesions in epilepsy in India J. Trop Med Hyg 97:347-353 1994
4. Rajshekhar V, Haran RP, Prakash GS et al. Differentiating solitary small cysticercal granulomas and tuberculomas in patients with epilepsy. Clinical and CT criteria J. Neurosurg 78; 402-407 1993
5. O.H Del Brutto, J. Sotelo and G. Roman. Neurocysticercosis;a clinical handbook, Swets and Zeitlinger Lisse, The netherland 1998
6. O.H Del Brutto, R. Santibonez C, A.Noboa, R. Aguirre, E. Diaz, and TA Alarcan “Epilepsy due to NCC; Analysis of 203 patient; Neurology, vol 42, no 2, pg 389-392,1992
7. Del Brutto OH, Rajshekar V, White AC et al, proposed Diagnostic Criteria Of Neurocysticercosis, Neurology 157:177- 183;2004.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





