IJCRR - 7(15), August, 2015
Pages: 40-43
Date of Publication: 11-Aug-2015
Print Article
Download XML Download PDF
PREVALENCE OF ANEMIA AMONG RURAL SCHOOL CHILDREN OF RAJASTHAN
Author: Sanjay Mandot, Subhash Bamnawat
Category: Healthcare
Abstract:Aims: To study the prevalence of anemia among rural school children of Rajasthan. Study Design: A prospective cross sectional study was conducted in 8 government schools in tribal villages of Sirohi district over a period of 6 months. 1462 school children between 5 to15 years of age were clinically examined. Hemoglobin estimation was done using cynmethemoglobin method and peripheral blood smear were also examined. Anemia was diagnosed according to the WHO standard for the given age and sex. Materials and Methods: Hemoglobin estimation was done using cynmethemoglobin method. Peripheral blood film was prepared and stained by Leishman's stain using standard technique. Peripheral smear was examined by Pathologist to know the type of anemia and eosinophilia. Results: Overall prevalence of anemia was 83.6%. Girls had a higher prevalence of anemia than boys except at 10 years of age. Menarcheal age group girls (11 to15 years) were more anemic than boys and lesser age group girls (< 11 years). The commonest blood smear picture was microcytic hypochromic (56.4%). Eosinophilia was observed in 21.6% children. Conclusion: There is high prevalence of anemia in rural school children of this part of the country. Girls were at higher risk of developing anemia. Dietary modification, improvement in hygiene and awareness are the key strategies recommended for prevention.
Keywords: Anemia, Iron deficiency, Peripheral blood smear, Prevalence, School children
Full Text:
INTRODUCTION
Anemia in children, especially iron deficiency is the commonest and widespread health problem in India with an estimated prevalence of 50%. Nearly one-fifth of the population comprises of the school children. Nutritional disorders in the school children account for the majority of morbidity and school dropout. The children of tribal community due to their low socio-economic status, poor hygiene and poor awareness are more vulnerable to anemia. Iron deficiency along with anemia causes impaired growth, behavioral abnormalities and impaired cognitive function leading to poor school performance. It also adversely affects the immune system of the growing child. The main cause of iron deficiency is inadequate iron intake and low bioavailability of iron in the diet. During adolescence, the overall iron requirement of the body increases and in girls repeated menstrual blood loss also adds to iron deficiency. Intestinal parasitic infections are widely prevalent in many developing countries including India. These parasitic infections especially hookworms are particularly important in the school children as they aggravate malnutrition including iron deficiency. Numerous studies have shown prevalence of anemia between 22-94% as the methodology and criteria for diagnosing anemia has been variable (1-6).
MATERIALS AND METHODS
The study was conducted on 1462 children aged 5-15 years of government schools in villages namely Ker, Issara, Daanava, Kacholi, Delwara, Torna, Phula Bai Kheda and Panchdeval of Sirohi district. Children in selected schools were from low socioeconomic status and majority of them were scheduled tribes. A detailed proforma which included data regarding socioeconomic status, medical history and consent was given to school children to be completed by parents/guardians. A detailed medical examination including anthropometry was done by medical officer and recorded on the proforma. For hemoglobin estimation and peripheral smear examination blood was drawn by finger prick using 26G needle. Hemoglobin estimation was done using cynmethemoglobin method. Peripheral smear was examined by Pathologist to know the type of anemia and eosinophilia. Anemia was diagnosed and the children were grouped under different grades of anemia by adopting WHO guidelines (7). Analysis of the results was done using the statistical method – chi square test and p value.
RESULTS
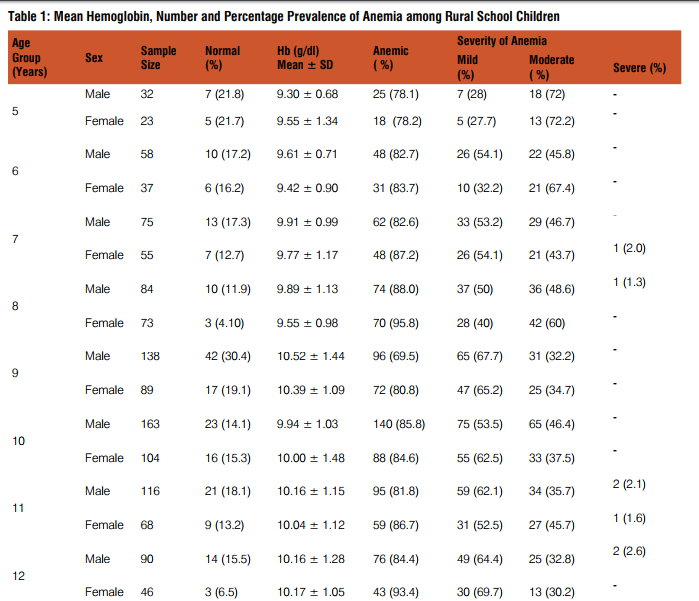
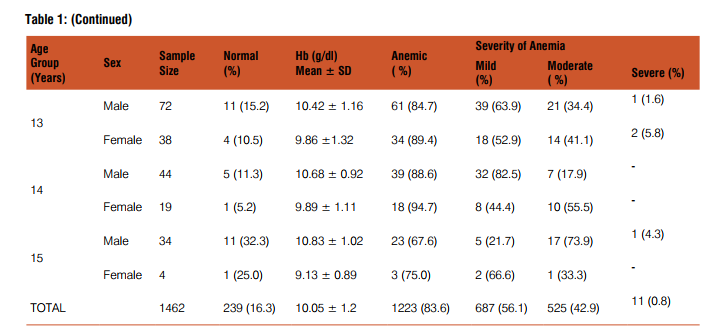
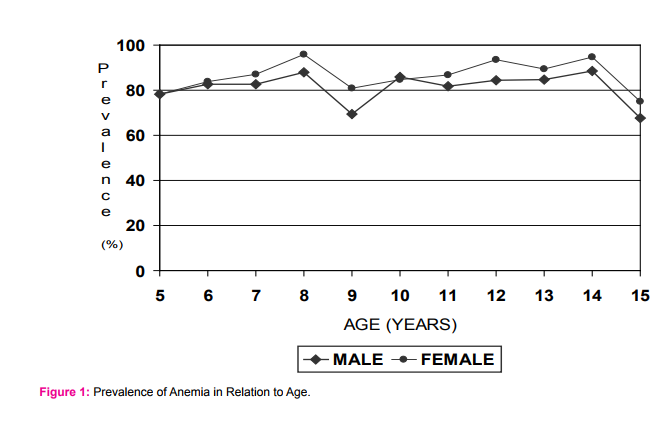
Out of 1462 school children studied only 239 (16.4%) were normal and 1223 (83.6%) were affected with various grades of anemia i.e. 664 (56.1%) mildly anemic, 525 (42.9%) moderately anemic and 11 (0.89%) severely anemic. The mean hemoglobin, number and percentage prevalence of anemia according to age in both sexes is shown in Table I. Girls had high prevalence of anemia (87%) compared to boys (81.5%) [Chi-square test value: 7.5 (df =1); p value ≤ 0.05, significant] at all ages except at 10 years age (Fig. I). A higher proportion (89.7%) of menarcheal girls (11-15 years age) had anemia. Moderate degree of anemia was more common in girls (45.4%) than boys. The commonest blood picture was microcytic hypochromic seen in 56.4% followed by normocytic normochromic and dimorphic in only 0.5%. Eosinophilia (>6%) on peripheral smear was observed in 21.6% school children.
DISCUSSION
The present study shows a high prevalence of anemia among school children of lower socio-economic status from tribal/ rural background .Occurrence of anemia in children from poor socio-economic status is a well fact and many studies have reported high prevalence of anemia among rural/tribal school children (8-11). It is apparent from Table I that out of 1462 children studied, only 16.3% were normal and 83.6% were affected from various grades of anemia. Iron deficiency is common in healthy, non anemic and high socio-economic status children also as reported by Thavraj et al3 . These children may have latent iron deficiency and possible reason for this could be the poor bio-availability of iron in the Indian diets. Male to female ratio was 1.6:1 which suggests that the lesser number of girls are enrolled in schools for education. Reasons could be due to gender bias as males are given better care over females. The girls had a higher prevalence of anemia except at 10 years of age. More menarcheal age group girls were anemic as compared to others because of increased iron requirement during adolescence and repeated menstrual blood loss .Various studies have also observed a high prevalence of iron deficiency anemia among adolescent girls of urban and rural areas (12-14). Predominantly Microcytic hypochromic (55.4%) blood picture was also reported in a study by Verma. M et al. on urban school children of Punjab (15). Eosinophilia was observed in 21.6% school children. This could be due to intestinal helmenthiasis especially hookworm infestation. Other common causes of eosinophilia like allergy and drug intake could not be applied to these school children at the same time. Filariasis is also commonly associated with eosinophilia but it is rare in this part of the country.
CONCLUSION
The present study shows that anemia is a major health problem among rural school children belonging to poor socioeconomic status. Dietary modification, routine iron supplementation, improvement in hygiene and awareness are the key strategies recommended for prevention.
Conflict of Interest: None.
Source of funding: By Investigator
Ethical Clearance: Obtained
ACKNOWLEDGEMENT
We acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. We are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Sundaram VM, Sankaranaraynan VS, Rajendran S, Varalakshmi, Sarasa. Health profile of school children in Madras City. Indian Pediatr 1978; 15: 586-725.
2. Gopaldas T, Kale M. Prophylactic Iron supplementation for underprivileged school boys. Indian Pediatr 1985; 22: 731- 743.
3. Thavraj VK, Reddy V. Serum Ferritin in healthy school children. Indian Pediatr 1985; 22: 51-57.
4. Goyal RC, Chavan VA. Health status of school children in Ahmednagar City. Indian J Maternal and Child Health 1993; 4: 81-83.
5. Aggarwal KN, Khanduja PC, Aggarwal PK, Madhavan S, Tarkar AD. Normal hematological levels for school children (5- 16 years). Indian Pediatr 1972; 9: 785- 795.
6. Malhotra AK, Srivastava RN. A study on impact of socio-economic status on hemoglobin levels of rural school children of district Wardha. Indian J Prev Soc Med 1982; 13: 95-99.
7. WHO. Indicators for assessing iron deficiency and strategies for its prevention. WHO/UNICEF/UNU 1998 Technical workshop. Geneva, World Health Organization 1998.
8. Gupta VM, Shukla KK. Epidemiology of anemia in preschool children from a rural and a slum community, Varanasi. Indian J Prev Soc Med 1985; 15: 85-89.
9. Aggarwal DK, Bhardwaj B, Singla PN, Tripathi AM, Aggarwal KN. Etiology of maternal and early childhood deficiency anemia. Indian J Pediatr 1986; 53: 389-396.
10. Sharma A, Sharma SK, Grover AK, Tewari AD, Abrol P. Anemia in protein energy malnutrition. Indian Pediatr 1985; 22: 841- 843.
11. Desai N, Chaudhry VP. Nutritional anemia in protein energy malnutrition. Indian Pediatr 1993; 30: 1471-1483.
12. Vasanthi G, Pawashe AB, Susie H, Sujatha T, Raman L. Iron nutritional status of adolescent girls from rural area and urban slum. Indian Pediatr 1994; 31: 127- 132.
13. Kapoor G, Aneja S. Nutritional disorders in adolescent girls. Indian Pediatr 1992; 29: 969-973. 1
4. Aggarwal K.N. Assessment of prevalence of anemia and iron in response to daily/weekly iron folate supplement in adolescent girls (10-18) from urban slums of North Delhi. UNICEF Contract No. 95/0075/1998, 1-9(1998).
15. M. Verma, J. Chhatwal and Gurmeet Kaur . Prevalence of anemia among urban school children of Punjab. Indian Pediatr 1999; 36: 1181-1186.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





