IJCRR - 7(16), August, 2015
Pages: 54-58
Date of Publication: 21-Aug-2015
Print Article
Download XML Download PDF
A STUDY OF HISTOPATHOLOGICAL CHANGES IN FALLOPIAN TUBES IN ECTOPIC PREGNANCY
Author: Richa Sharma, Dayanand S. Biligi
Category: Healthcare
Abstract:Aim: The study was conducted with the aim of studying histopathological changes in ectopic pregnancy in the fallopian tube and correlate them with clinical history. Methodology: Fifty cases of tubal ectopic were studied retrospectively to compare the histopathological changes in the lining of fallopian tube. Routine haematoxylin and eosin stain with special stains were employed to study the sections. Ratio of ciliated to secretory cells was calculated. Associated inflammation and other pathology was also studied. Results: Out of 50 cases studied majority of ectopics were on right side and presented at less than 8 weeks of gestation. Most common age group to be affected was between 28-32 yrs. Around 28 of cases had previous history of surgeries and 14% previous ectopic or abortions. We also noted a significant degree of deciliation in the tubal lining with maximum number of cases showing deciliation in fimbrial ectopics. Significant number of cases showed association with salpingitis isthmica nodosa (22%) and inflammation was seen in three fourths of all cases.
Conclusion: The study highlights the association with deciliation in tubal ectopics and also the significant association with inflammation and abdominal interventions
Keywords: Ectopic, Deciliation, Fallopian tube, Salpingitis isthmica nodosa
Full Text:
INTRODUCTION
Ectopic pregnancy is the term applied to implantation of the fetus in any site other than a normal intrauterine location. The most common site is within the fallopian tubes (~90%). Other sites include ovary, the abdominal cavity and intrauterine portion of the fallopian tube (cornual pregnancy). Ectopic pregnancy occur about once in every 150 pregnancies. (1) In a multicentric case control study in India, (ICMR Task Force Project, 1990) the incidence of ectopic pregnancy was 3.12 per 1000 pregnancies or 3.86 per 1000 live births. (2) While there has been about four fold increase in incidence over the couple of decades but the mortality has been slashed down to about 80%. (3)
AIMS
1. To study the changes in fallopian tube in tubal ectopic pregnancy
2. To correlate the changes with age group, medications, other medical conditions and previous surgical history.
METHODOLOGY
It was a retrospective study of fifty cases conducted in the Department of Pathology, Victoria Hospital, Bangalore medical college and research institute over the period from January 2010 to December 2010. Haematoxylin and eosin stain with special stains were done on all the sections. The pathological findings were correlated with clinical data like age distribution, parity, associated medical conditions, previous pregnancies and history of surgical procedures. Microscopically, ratio of ciliated to secretory cells was calculated. An area of 1x1 mm was screened and number of ciliated and secretory cells were counted. We also did mas son’s trichrome (fig 8) on the sections which clearly showed secretory cells with granules in them and cilia as well. Also additional findings of inflammation (acute, chronic, follicular ) and salpingitis isthmica nodosa were noted.
RESULTS
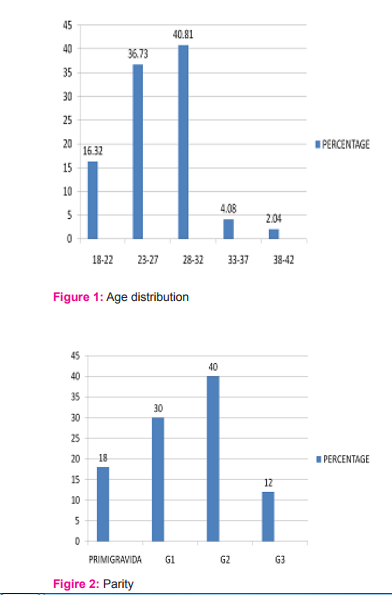
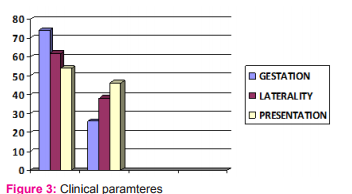
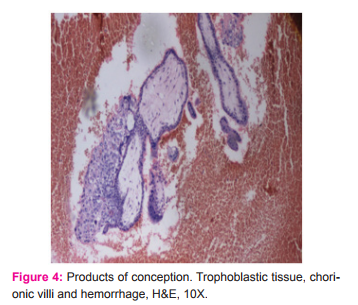
The study showed that maximum cases of ectopic were in the age group (fig 1) of 28 to 32 years ( 40.81 %) . Most of the women were multigravidae, maximum cases seen in gravida2 (fig 2). Primigravida presenting with ectopic constituted just 18% (fig 2) of all the cases. Most commonly women presented in less than 8 weeks gestation (74% cases - fig 3). There was a striking predominance of right sided ectopics ( more than 60% - fig 3). Over half of the cases presented with ruptured pregnancy (54% - fig 3).
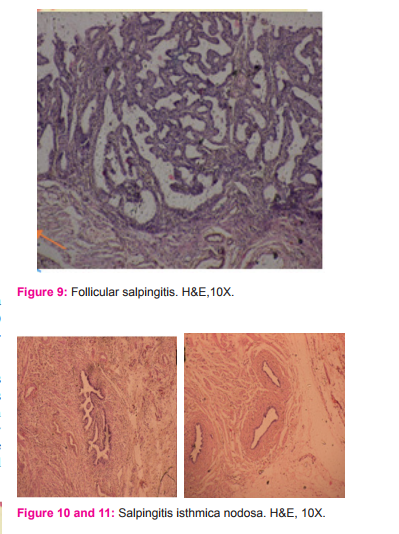
Intra operatively the common site of ectopic was fimbriae (52.1%) followed by ampulla (39.13%) and 8.6% cases in cornua. There was also a significant association seen with previous surgeries. Six cases had previous history of ectopic pregnancy (12%) . Seven cases had previous history of abortions and medical termination of pregnancy (MTP). Six cases had previously undergone tubectomy/fimbriectomy and 8 cases had history of bilateral abdominal tubectomy. In the study, 6 cases had lower segment caesarean section (LSCS) in their previous pregnancies. One patient had history of tuboophorectomy in the past. Two cases were treated with Methotrexate but needed surgery owing to failure to respond to medical management. Histopathologically, majority ectopics were in ampulla(54%). Along with findings like tubal dilation, congestion, hemorrhage, trophoblastic tissue (fig 4) , presence of villi, ratio of ciliated to secretory cells (fig 6 and 7) were also calculated. The sections also showed concurrent presence of acute salpingitis (16%) , chronic salpingitis (56%) and follicular salpingitis (12%) (fig 9).
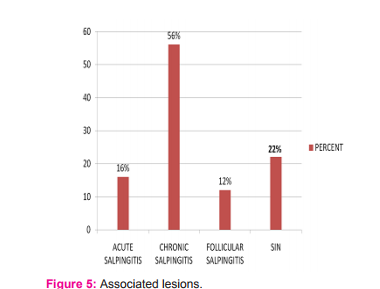
There was a significant association with salpingitis isthmica nodosa -22%(abbreviated as SIN in the graph above - fig 5) . Salpingitis isthmica nodosa (fig 10 and 11) is a known etiological factor for infertility and ectopic pregnancy. Another very significant finding noted in the study was marked deciliation in majority of cases. Around 20 cases were in fimbria and all of them showed marked deciliation ( fig 8) in tubal epithelium. Out of 27 cases of ampullary ectopic 18 showed features of decilaition and only 9 were normal. The 3 cornual ectopic showed 2 cases with reduced cilia and only 1 case showed normal cilia distribution.

DISCUSSION
Anatomy of fallopian tube : The Fallopian tubes are paired, tubular, seromuscular organs whose course runs medially from the cornua of the uterus toward the ovary laterally. Each tube is about 10 cm long with variations in length from 7 to 14 cm. The fallopian tube is shaped like an elongated funnel and is divided anatomically into four parts – infundibulum, ampulla, isthmus and interstitial part. (4) The tubal wall consists of three layers: the internal mucosa (endosalpinx), the intermediate muscular layer (myosalpinx), and the outer serosa, which is continuous with the peritoneum of the broad ligament and uterus, the upper margin of which is the mesosalpinx. The serosal layer and broad ligament have a lining of mesothelium. The muscular wall has two layers , an inner circular and outer longitudinal. (5) The inner aspect of the tube is lined by mucosa arranged in the shape of longitudinal, branching folds ( known as plicae) , which merge with the fimbriae. (6) Microscopically the epithelium is composed of three distinct cell types: secretory, ciliated and intercalated “(peg). (7) There are fewer ciliated cells in the isthmus than in the ampullary portion of the tube, whereas they are most prominent in the fimbriated infundibulum. Ciliation and deciliation is a continuous process throughout the menstrual cycle. Ciliation is maximum in the periovulatory period, particularly in the fimbria. Estrogen enhances the process of ciliation, whereas progesterone inhibits it, so significant deciliation occurs in atrophic postmenopausal tube. (8) Diagnosis of ectopic pregnancy is clinical. In tubal pregnancy the gestational sac is completely made up of tubal tissue, with no participation from the ovarian or intraligamentary tissues.(9) Hydropic changes and polar trophoblastic proliferation can occur; they should not be overdiagnosed as hydatiform mole.(10) Changes resembling atherosclerosis may be seen in tubal arteries at the site of implantation, analogous to those occurring in the uterus in orthotopic pregnancy. (9) The fallopian tube epithelium may undergo clear cell hyperplasia. (11) In a multicentric case control study in India, (ICMR Task Force Project, 1990) the incidence of ectopic pregnancy was 3.12 per 1000 pregnancies or 3.86 per 1000 live births. In our series the ectopic pregnancy rate is 7.06 per 1000 deliveries or in other terms 1 in every 141 deliveries. Tubal ectopic commonly seen in 28-32 years age group. Previous studies have shown a higher frequency in 25-28 years of age (Cole and Corelett (12)). Another study by Andersen et al (13) showed 1.4% of all pregnancies in young age group to 6.9% in older age groups. Murray et al (14) showed common gestational age at diagnosis to be 6 to 10 weeks. Our series of cases showed predominance in less than 8 weeks of gestation. Our study showed a predominance of ectopic gestation in parous women. Studies conducted by Hlavin et al (15) and De Cherney et al (16) showed highest incidence in those with two to three children. 62% cases were seen on right side. This is thought to be due to spread of infection from appendicitis. (17) Majhi et al (18) in the study had 72% cases presenting as ruptured ectopic. With a significant number of cases in our study too presenting with rupture explains why we consider ectopic a life threatening condition. Majhi et al(18) also noted ectopic in patients with history of tubectomy (14.4%), abortion (26.1%), previous caesarean section (11.1%). Our study also showed a similar association with tubectomy and other intraabdominal surgeries. Histopathologically, common site was ampulla (54%) then fimbria (40%) consistent with previous studies. Dahiya et al (19) estimated 79% cases in ampullary region and 16% in fimbria. Our study showed reduction in ciliated cells in affected fallopian tubes with all the fimbrial ectopics showing marked deciliation indicating that deciliation of the lining cells play a significant role in the pathogenesis of tubal ectopic. Our findings correlate with that of Vasquez et al (20). Dahiya et al showed incidence of 6% of salpingitis isthmica nodosa (SIN), while studies done by Homm et al (21) and Dubuisson et al (22) showed incidence of 45.9% and 36.4% respectively. Our study showed a significant association of 22% with SIN and very marked association with acute salpingitis or chronic or follicular salpingitis. These findings suggests that there is a indicative contribution of inflammation in causation of ectopics.
CONCLUSION
The study highlights the association of deciliation with ectopic pregnancy. The cilia of the fallopian tube physiologically helps in fertilisation and implantation of the embryo. Deciliation can happen for various reasons for example pelvic inflammatory disease and this predisposes for ectopic pregnancy. Ectopic pregnancy in theory can be prevented by preventing and timely management of conditions predisposing it.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles / journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Kumar Vinay, Abbas Abul K, Fausto Nelson, Aster Jon C. Robbins and Cotran Pathologic Basis of Disease. 8th edition. Elsevier. 1053-1054.
2. Vyas Priti S, Vaidya Pratibha. Epidemiology, diagnosis and management of ectopic pregnancy -an analysis of 196 cases. Bombay hospital journal.
3. Dutta DC. Textbook of Obstetrics. Edited by Hiralal Konar. 6thed.Central book agency .2004.179.
4. Young Barbara, Lowe James S, Stevens Alan, Heath John W. In: Wheater’s Functional histology. 5th ed. 367.
5. Young Barbara, Lowe James S, Stevens Alan, Heath John W. In: Wheater’s Functional histology. 5th ed. 368.
6. Rosai Juan. Female reproductive system. In: Rosai and Ackerman’s Surgical pathology. Vol 2. Ed.9. Elsevier Inc.2009.1636
7. Hendrickson MR, Kempson RL. Normal histology of the uterus and fallopian tubes. In : Sternberg S (ed): histology for pathologist, ed.2. Philadelphia, 1997; Lippincott-Raven: 879-928
8.http://www.gfmer.ch/International_activities_En/El_Mowafi/ Fallopian_tube.htm
9. Rosai Juan. Female reproductive system. In Rosai and Ackerman’s Surgical pathology. Vol 2. Ed.9. Elsevier Inc,2009: 1639
10. Burton JL, Lidbury EA, Gillespie AM, Tidy JA, Smith O, Lawry J, Hancock BW, Wells M. Over-diagnosis of hydatidiform mole in early tubal ectopic pregnancy. Histopathology 2001, 38: 409- 417.
11. Blaustein A, Shenker L, Vascular lesions of the uterine tube in ectopic pregnancy. Obstet Gynecol 1967, 30: 551-555.
12. Cole T, Corlett RC 1982. Chorionic ectopic pregnancy. Obstetrics and Gynecology 59: 63-68.
13. Nybo Anderson AM, Wohlfahrt J, Christens P, Olsen J, Melbye M.Maternal age and fetal loss:population based register linkage study. BMJ. 2000 Jun 24;320(7251):1708-12.
14. Heather Murray, Hanadi Baakdah, Trevor Bardell, Togas Tulandi. Diagnosis and treatment of ectopic pregnancy. CMAJ.2005 Oct11; vol173:no8: 905-12.
15. Hlavin GE, Ledoski LT, Bren JL.Ectopic pregnancy: an analysis of 153 patients. International Journal of Gynaecology and Obstetrics.1978;16:42-47.
16. De Cherney AH, Minkin MJ, Spangler S 1981a. Contemporary management of ectopic pregnancy. Journal of Reproductive Medicine 26:519-523.
17. F. Cunningham, Kenneth Leveno, Steven Bloom, John Hauth, Larry Gilstrap, Katharine Wenstrom. Williams Obstetrics. 22nd Edition. McGraw Hill Professional;2005:266.
18. Majhi AK, Roy N, Karmakar KS, Banerjee PK. Ectopic pregnancy – an analysis of 180 cases. J Indian Med Assoc.2007 Jun;105(6): 308, 310, 312.
19. Dhaiya N, Singh S, Kalra R, Sen R, Kumar S. Histopathological changes associated with ectopic tubal pregnancy. IJPSR,2011;Vol.2(4): 929-933.
20. Vasquez G, Winston RM, Brosens IA. Tubal mucosa and ectopic pregnancy. Br J Obstet Gynaecol. 1983 May;90(5): 468-74.
21. Homm RJ, Holtz G, Garvin AJ. Isthmic ectopic pregnancy and salpingitis isthmica nodosa. The American fertility society.1987;48: 756-60.
22. Dubuisson JB, Aubriot FX, Cardone V, Vaucher-Lavenu MC. Tubal causes of ectopic pregnancy. Fertil steril 1986; 46: 970-2.
26. Milman N1, Byg KE, Bergholt T, Eriksen L, Hvas AM. Body iron and individual iron prophylaxis in pregnancy--should the iron dose be adjusted according to serum ferritin? Ann Hematol. 2006 Sep;85(9):567-73. Epub 2006 May 30.
27. WHO. Iron deficiency anaemia: assessment, prevention, and control. A guide for programme managers. Geneva, Switzerland: World Health Organization, 2001. (WHO/NHD/01.3.)
28. Albonico M1, Stoltzfus RJ, Savioli L, Tielsch JM, Chwaya HM, Ercole E, Cancrini G. Epidemiological evidence for a differential effect of hookworm species, Ancylostoma duodenale or Necator americanus, on iron status of children. Int J Epidemiol. 1998 Jun;27(3):530-7.
29. Bakta, I. M., Wijana, D. P., and Sutisna, P. (1993). Hookworm infection and iron stores: a survey in a rural community in Bali, Indonesia. The Southeast Asian journal of tropical medicine and public health, 24(3), 501-504.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





