IJCRR - 7(17), September, 2015
Pages: 59-65
Date of Publication: 11-Sep-2015
Print Article
Download XML Download PDF
EMPOWERMENT AND ENGAGEMENT OF SHE WOMEN AGAINST VIOLENCE DURING SEX INTIMACY: AN INTERVENTION STUDY FROM KARNATAKA, INDIA
Author: Manoj Kumar Gupta, Veena R.
Category: Healthcare
Abstract:Objective: To empower and engage the Self Help Groups (SHGs) women against violence during sex/intimacy with the use of IEC strategy so that they can act as change agents for other women in the community. Methods: This was a 'Multi-centric Action Research Demonstration Study'. As an intervention, series of workshops were conducted with the help of pre-developed IEC material. Results: The intervention was found effective in the form of a significant change in level of perception among SHG women that violence during sex or intimacy is abnormal, improvement in awareness about women's right to decline to the partner from having sex while encountering violence from him and significant reduction in their experience of facing violence during intimacy or sex in last one year. Conclusion: This study provides experience of the feasibility; efficacy and impact of health education interventions and an insight into the development and implementation of effective interventions against violence during sex or intimacy in India.
Keywords: Health education, Sexual violence, IEC, Self help group (SHG)
Full Text:
INTRODUCTION
Domestic violence is manifested through physical, sexual, psychological and economic abuse (Domestic violence against women and girls 2000). The “protection of women from Domestic Violence Act, 2005” says that any act, conduct, omission or commission that harms or injures or has the potential to harm or injure will be considered domestic violence by the law. Even a single act of omission or commission may constitute domestic violence (Kaur R, 2008; the protection of women from domestic violence act, 2005). However, even in the presence of this act, there is a gloomy picture. In depth analysis of National Family Health Survey-3 (NFHS-3) (2006-2007) showed that the prevalence of physical violence among Indian women is as high as 31% and that of sexual violence is also as high as 8.3% (Kimuna SR, 2013). Sexual abuse and rape by an intimate partner is not considered a crime in most countries, and women in many societies do not consider forced sex as rape if they are married to, or cohabiting with, the perpetrator. The assumption is that once a woman enters into a contract of marriage, the husband has the right to unlimited sexual access to his wife. In Zimbabwe women were told that the use of force by a husband is “a part of life”. In Nicaragua and Haiti, it is believed that women do not have the right to refuse sex if they do not feel like it and that in some circumstances men are justified to beat their wives (Population council, 2004). More than two decades of research has shown that sexual violence and intimate partner violence within or outside marriage are major public health problems with serious longterm physical and mental health consequences, as well as significant social and public health costs (Breiding MJ, 2008; Logan TK, 2007; Randall T, 1990; WHO, 2002). An expanding and persuasive body of evidence from diverse settings has documented the connection between sexual violence and reproductive and sexual health risks (Koenig M, 2004; Kishor S, 2004; Parish WL, 2004; Martin SL, 1999; Caceres CF, 2000; WHO, 2005). Many studies are of the view that violence by intimate partner most likely undermines the sexual and reproductive health of the women. This extensive violence has significant harmful effects like unwanted pregnancy (Khan ME, 1996),gynecological disorders (Golding JM, 1996) and physical injuries to private parts (Stark E, 1979). Internationally, one in three women have been beaten, coerced into sex or abused in their lifetime by a member of her own family (Heise L, 1999). Looking at the domestic front, staring from Vedic age to twenty first century, women in India perhaps have never experienced equal rights and freedom compared to their male counterparts. Underdevelopment, lack of economic opportunities for both sexes, and entrenched inequalities in the distribution of power, resources, and responsibilities between men and women (gender inequalities) create a risk environment that supports high levels of intimate-partner violence (Mane P, 1994; Gupta GR, 2002; Garcia-Moreno C 2000). In many developing countries women “believe” that the use of force is a man’s “right” and submission is the only way to avoid pain and ensure security in the marital home. Young women from various settings in South Asia said or were told: “I had feelings of discomfort but I had to accept my husband’s wishes.”“If you won’t give him then he will force you and you would have pain” (George A, 2003). A few studies in South Asia have explored the various coping strategies used by young married women to avoid situations of high personal risk for sexual violence. These studies revealed that young married women try to avoid unwanted sex with their husbands by threatening to scream, in order to endanger the husband’s prestige, threatening to commit suicide, waking up young children, and feigning menstruation (Santhya KG, 2005; Puri M, 2007; Puri M, 2010; Women’s Rehabilitation Centre, 2002; Khan ME, 2002; George A, 2002). Alternatively, some women try to develop a greater intimacy with their husbands, communicate sexual desire, and participate more equally in sex-related decision making to avoid unwanted sexual experiences (Khan ME, 2002; George A, 2002; Joshi AM, 2001). It has been proved that, if the women are given an intervention (life cycle education) regarding the sexual violence at the beginning of their sexual life then there might be a long term impact on reduction in incidence and prevalence of sexual violence. However, in a conservative society like India, talking about sex and other gynecological problems of women is a taboo. Across all strata of the society, these issues are not discussed with the girls before marriage (George A, 2003; Alaudin M, 1999). Even teachers and parents hesitate in talking sexual health issues with the young girls and boys. In this regard a ‘culture of silence’ prevails that inhibits women from revealing their private problems to others due to various social factors. In order to develop effective intervention programme and policy for sustained behavioural change, which is a longdrawn process, it is vital to know the attitude and perception of the women towards the issue in-depth. Communication strategies at the community level by integrating Information, Education and Communication (IEC) tools into public health programs may have great role to influence the change in attitudes, perceptions and behavior of people in the community. Development and use of IEC material along with active participation by the community ensures delivery of appropriate information and knowledge to people which in turn empowers them to make informed decisions about their life. IEC involves building social networks and communicating the information through appropriate channels and methods in a manner that is culturally accepted by the community. Health care workers in rural areas act as change agents and are trained to communicate the information contained in these materials to the community. Studies have proved that education can be a protective factor towards sexual violence by empowering women (Kimuna SR, 2013). With this background the present study was designed to empower and engage the SHG women against violence during sex/intimacy by creating awareness and sustaining interest through lesson plans in the IEC material so that they can act as change agents for other women in the community.
METHODS
A ‘Multi-centric Action Research Demonstration Study’ (Karnataka, Rajasthan and Chhattisgarh) was conducted to sensitize and engage Self Help Groups (SHGs) women through community mobilization. These women were sensitized and empowered and empowered to take care of their reproductive health including cervical cancer. Besides that it was expected that those SHG women will act as change agent for other women in the community. This study was conducted from May 2012 to October 2013. In the preparatory phase of this study (three months), extensive literature search was done, tools were designed and finalized, IEC materials were developed and baseline data was collected through household survey (HHs) and focus group discussions (FGDs). In the intervention phase (one year), a series of workshops were conducted for the SHG women to meet the objectives. In those workshops the pre-developed IEC materials were used to increase the awareness of SHG women. After that, an end-line data was collected through HHs and FGDs. The data was analyzed and report was prepared and submitted to fun ding agency. This paper has taken data from that original study. The primary study site was Kolar District of Karnataka state. From five taluks of Kolar district, Bangarpet taluk was selected as intervention taluk by applying simple random sam-pling. With the help of purposive sampling the nearby taluk, Malur was selected for adequate counter-factual which has socio-demographic, climatic, developmental and health indicators similar to Bangarpet taluk. In both these taluks HHs and FGDs were conducted to collect quantitative and qualitative information, respectively both during baseline and endline. During intervention phase, fifteen 3-day workshops were conducted targeting 75-80 SHGs in Bangarpet taluk. The local NGOs working in intervention site were involved in those sensitization workshops. In Dharwad, Koppala, Jaipur and Raipur districts only qualitative evaluation using FGDs were done, and only two workshops, each consisting three days, were conducted. Only quantitative data analysis of intervention district of Karnataka has been included in the present article.
Sample size: As per the literature search and by assuming the minimum prevalence (50%) about correct perception of SHG women regarding violence during sex/intimacy and considering 10% permissible level of error in the estimated prevalence, the sample size was calculated using the formula n= z2 pq/L2 . The calculated sample size (384) was rounded up and fixed to 400 and decided to interview 200 SHG women from Bangarpet and 200 from Malur taluks during baseline and end-line each.
Selection of Households: There are 3 Community Mobilization Research Centers (CMRCs) in Bangarpet taluk (Kamsamudra, Toppanahalli and Budikote) and 2 CMRCs in Malur taluk (Thoralakki and Dinnahalli). From each CMRC, 6 villages were selected by simple random sampling method. Thus a total of 30 villages were selected for the study. In the selected villages total enumeration of SHG women was done to prepare a sampling frame. The required study subjects for each taluk were selected adopting probability proportion to size (PPS) sampling technique. In order to get required study subjects, simple random sampling was done. SPSS v16.0 software was used to analyze the generated data. For statistical inference chi-square test was applied. The statistical significance was decided based on the p value. A p value of <0.05 and <0.01 were taken as significant and highly significant, respectively.
RESULTS
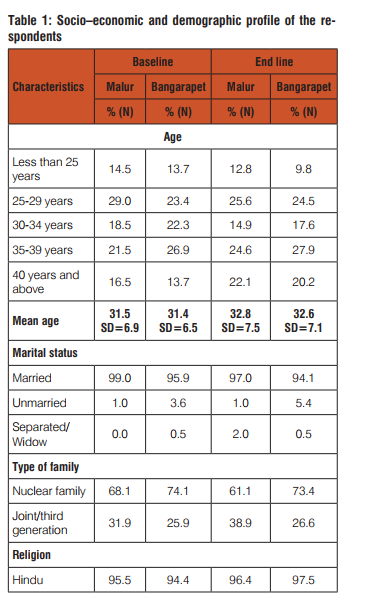
Table 1 presents the socio-economic and demographic profile of the respondents in Malur and Bangarapet taluks in Kolar district during baseline and end line surveys. The total number of households covered during baseline survey was 397 (200 in Malur and 197 in Bangarapet) and end line survey was 401 (197 in Malur and 204 in Bangarapet). It is evident from the table that the mean age of the respondents during baseline survey and end line survey was 31.4 years (SD= 6.7) and 32.7 years (SD=7.3), respectively. There was no significant variation in the mean age of the respondents in Malur and Bangarapet taluks. More than 95 percent of the respondents in both the taluks were married. More than 60 percent of the respondents in Malur and around three fourth of the respondents in Bangarapet taluk were belonging to nuclear family. A vast majority of the respondents were Hindus. With regard to caste of the respondents, more than 35 percent of the respondents belong to scheduled caste or scheduled tribes and more than one fourth belong to Other Backward Castes (OBC) in both the taluks. More than 90 percent of the respondents have a ration card. It is to be noted here that majority of the respondents in both Malur and Bangarapet taluks belong to either Below Poverty Line (BPL) or extremely BPL category.

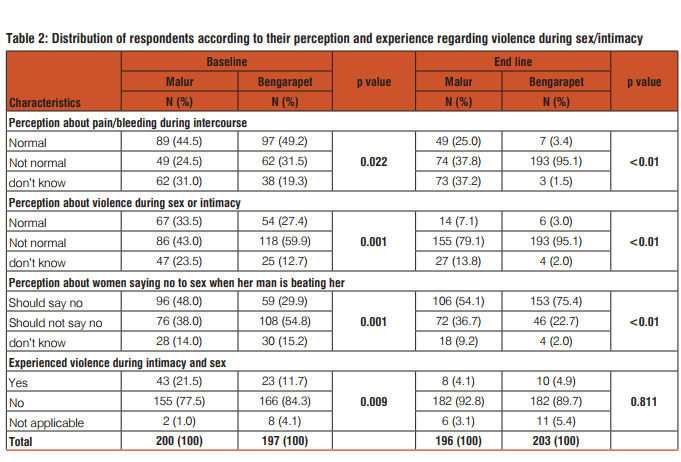
During baseline survey 24.5% of respondents from Malur taluk and 31.5% respondents from Bangarpet taluk reported that pain/bleeding during intercourse is not a normal phenomenon. There was found a highly significant (p<0.01) difference in the level of perception about pain/bleeding during intercourse in Bangarapet (95.1%) and Malur (37.8%) during end line survey. More than one third of the respondents in both the taluks had perception that violence during sex or intimacy is normal. With the help of planned workshops this perception could be reduced to less than five percent in the intervention taluk. Considering the selection of nearby taluk as control to match the socio demographic milieu and longevity of intervention (one year), some knowledge diffusion was observed in control taluk in the form of improvement (~80%) in perception that violence during sex or intimacy is abnormal. Respondents were asked to report their perception about woman’s right to decline from having sex while encountering violence from her partner. Forty-eight percent of the respondents from Malur and near about 30 percent respondents from Bangarapet reported on an affirmative note. During end line survey, a highly significant improvement (75.4%) was observed in the awareness level of SHG women in intervention taluk about their rights. A highly significant change in level of perception that violence during sex or intimacy is abnormal and improvement in awareness about women’s right to decline to the partner from having sex while encountering violence from him was clearly reflected in their experience of facing violence during intimacy or sex in last one year. Before intervention more than 20 percent of women in intervention taluk and nearly 10 percent women in control taluk had experienced violence during intimacy or sex. The corresponding percentage during end line survey was less than five percent for both the taluks.
DISCUSSION
Violence against women and gender inequality result from a complex array of interwoven factors and is often embedded in social customs that allow it to be perpetrated with impunity – even, in many cases, without being considered as violence, let alone a crime. International and regional legal and policy instruments have clarified the obligations of countries to eradicate and punish violence against women. However, States are failing to meet the requirements of the international legal and policy framework. Laws have continued to change over the decades to reflect a definition of what constitutes sexual assault that is more sensitive to the needs of victims, yet the shift in societal attitudes is not necessarily keeping pace. Efforts to empower women must address current norms and traditional social customs that legitimize violence against them. Educational sessions are perhaps the most commonly recognized form of sexual violence prevention work. According to UNESCO, 2009, the primary goal of sexuality education is to equip children and young people with the knowledge, skills and values to make responsible choices about their sexual and social relationships in a world affected by HIV. In addition to learning about the risks of pregnancy and sexually transmitted infections (including HIV), children and young people also need to learn about the risk of sexual exploitation and abuse in order to recognize these when they occur, to protect themselves as far as possible and to identify and access available sources of support. Nearly half of the respondents in the present study were considering pain/bleeding during intercourse as a normal phenomenon and more than one third of the SHGs women in both the study taluks had perception that violence during sex or intimacy is normal. These findings represent that perception of women regarding violent behavior of their intimate partner during sex is trapped and modulated by deep rooted culture sense of sexual obligation in a marital relationship. This statement is supported by Culbertson K and Dehle C, 2001 stating that women may internalize the cultural sense of sexual obligation in a marital partnership due to the perceptions that, a woman is obliged to be sexually available to her partner once a past sexual relationship has been established. As far as the perception about woman’s right to decline from having sex while encountering violence from her partner is considered, more than one third of the respondents from both the study taluks had perception that women should not refuse sex to her partner under any of the given circumstances. This figure was quite higher than the findings of many other studies (Garcia-Moreno C, 2006; Sharma KK, 2011). The planned intervention in the present study could significantly improve the awareness level of SHG women in intervention taluk about their right to refuse for sex when her partner is showing any kind of violent behavior. Similar findings have been reported by Breitenbecher KH, 1999. The paucity of nationally representative data makes it difficult to establish the prevalence of non-consensual sex among married young women in developing countries. In the present study, more than fifteen percent women in the study area had experienced violence during intimacy or sex. This is supported by the findings of many other research studies on domestic violence from developing countries which suggests that anywhere from 10-60% of married women of reproductive age report experiencing some form of domestic violence (Santhya KG, 2005; Khan ME, 2002; Sharma KK, 2011; Jejeebhoy S, 2003; Watts C, 2002; Koenig MS, 2003). Similar kind of evidence have been proposed by the Demographic and Health Surveys (DHS) and other surveys which suggests that between 3 and 23 percent of married young women (aged 15-24) in developing countries such as Cambodia, Colombia, Haiti, India, Nepal, Nicaragua and Zambia have ever experienced non-consensual sex by a current or former spouse (Hof C, 1999). Many other studies on ever-married or -partnered young women in Asia had also shown that between 3% and 33% of them have experienced coerced sex within a formal union or marriage (Santhya KG, 2005; Im-em W, 2006; Allen DR, 2003; Alexander M, 2006). But the findings of the present study are quite lower than the findings of many other studies conducted in India (Martin SL, 1999; Puri M, 2011; Santhya KG, 2007) and higher than the findings of NFHS III (IIPS, 2007) and a study conducted by Mishra A et al. in 2014. The corresponding percentage of experiencing sexual violence was reduced to less than five percent in the present study. Similar kind of findings showing effectiveness of women’s empowerment intervention in reducing sexual violence has been reported by a pilot study “an intergenerational women’s empowerment intervention to mitigate domestic violence” conducted in Bangalore, India (Krishnan S, 2012). The consequences of violence during sex/intimacy can be severe, and in fact, intimate partner violence is one of the leading causes of death among women 15-44 years of age (Im-em W, 2003). This kind of violence is strongly associated with physical and mental health morbidity, including homicide, suicide, physical injuries and emotional distress as well as HIV seropositivity (Watts C, 2002; Chowdhary N, 2008; Ellsberg M, 2008; Maman S, 2002; Decker MR, 2009). However the present study shows its limitation in exploring those consequences. In summary, despite the grave consequences of sexual violence, and its persistence both within and outside marriages, this subject has received relatively little attention from researchers, policy makers, and programme managers in India. The experience of sex violence undermines the empower-ment women and certainly is a barrier to the socio- demographic and economic development of the country. As it is found to be deep rooted in the socio cultural practices and both the perpetrator as well as victim takes it granted, there is need of major transformation in the socio cultural milieu through proper and effective behavior change of the community and empowerment of women is the key to break this negative persistent culture sense. The results of present study provide an insight into the development and implementation of effective interventions against violence during sex or intimacy in India. Again, though the present findings are silent about the legal side of the issue, stringent laws against the perpetrators of the violence should be implemented effectively to curb the issue.
CONCLUSION
This study provides experience of the feasibility, efficacy and impact of health education interventions with the help of IEC materials on improving awareness and right practices of women (empowerment) in regard with violence during sex/ intimacy. The study highlights that further research is needed in this direction to address the issues more sensibly. In view of the above results it can also be concluded that we need to have effective strategies for empowering women against violence during sex / intimacy through proper information, education, and behavior change in culturally acceptable manner.
Ethical approval This study was approved by the ethical review committee of Karnataka Institute of Medical Sciences (KIMS), Hubli, Karnataka on November 15th 2011. Written consent was taken from the respondents before starting the interviews.
Competing interests None declared
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of Funding
This study was funded by Indian Council of Medical Research, New Delhi (File No.5/11/33/11-SBR,02/05/2012).
References:
1. Alaudin M, Maclaren L. Reaching newlywed and married adolescent. In Focus: Focus on young adults 1999 July; 1-7. Available at: http://www.pathfinder.org/publications-tools/pdfs/Reaching-Newlywed-and-Married-Adolescents.pdf (Last accessed on 07/9/2014).
2. Alexander M, Garde L, Kanade S, Jejeebhoy SJ, Ganatra B. Formation of Partnerships Among Young Women and Men in Pune District, Maharashtra, New Delhi: Population Council, 2006. Available at http://www.popcouncil.org/uploads/pdfs/Pune_Report.pdf (Last accessed on 17/9/2014)
3. Allen DR, Carey JW, Manopaiboon C, Jenkins RA, Uthaivoravit W, Kilmarx PH, Van Griensven F. Sexual health risks among young Thai women: implications for HIV/STD prevention and contraception, AIDS and Behavior 2003;7(1):9–21.
4. Breiding MJ, Black MC, Ryan GW. Chronic disease and health risk behaviors associated with intimate partner violence—18 U.S. states/territories, 2005. Annals of Epidemiology 2008;18:538–544.
5. Breitenbecher KH. A Longitudinal Evaluation of the Effectiveness of a Sexual Assault Education Program. J Interpers Violence 1999;14(5):459-478.
6. Caceres CF, Marin BV, Hudes ES. Sexual coercion among youth and young adults in Lima, Peru. Journal of Adolescent Health 2000;27(5):361-367.
7. Chowdhary N, Patel V. The effect of spousal violence on women’s health: findings from the Stree Arogya Shodh in Goa, India. J Postgrad Med. 2008;54(4):306–312.
8. Culbertson K, Dehle C. Impact of sexual assault as a function of perpetrator type. Journal of Interpersonal Violence 2001;16(10):992–1007.
9. Decker MR, Seage GR, Hemenway D, Raj A, Saggurti N, Balaiah D, Silverman JG. Intimate Partner Violence Functions as Both a Risk Marker and Risk Factor for Women’s HIV Infection: Findings from Indian Husband-Wife Dyads. J Acquir Immune Defic Syndr 2009;51(5):593-600.
10. Domestic violence against women and girls. Innocenti Digest, 6. Florence, Italy: UNICEF Innocenti Research Centre; 2000. Available at: http://www.unicef-icdc.org/publications/pdf/digest6e.pdf . (Last accessed on 29/11/2014).
11. Ellsberg M, Jansen HA, Heise L, Watts CH, Garcia-Moreno C. Intimate partner violence and women’s physical and mental health in the WHO multi-country study on women’s health and domestic violence: an observational study. Lancet. 2008;371(9619):1165–1172.
12. Garcia-Moreno C, Jansen HA, Ellsberg M, Heise L, Watts C. Prevalence of intimate partner violence: findings from the WHO multi-country study on women’s health and domestic violence. Lancet 2006;368(9543):1260-9.
13. Garcia-Moreno C, Watts C. Violence against women: it’s importance for HIV/AIDS. AIDS 2000;14(3):253–65.
14. George A. 2003. Newly married adolescent women: Experiences from case studies in urban India. In S Bott, Jejeebhoy S, Shah I, Puri C. eds, Towards Adulthood: Exploring the Sexual and Reproductive Health of Adolescents in South Asia, pp. 67-72, Geneva: WHO. Available at http://whqlibdoc.who.int/publications/2003/9241562501.pdf (Last accessed on 25/9/2014)
15. George A. Embodying identity through heterosexual sexualitynewly married adolescent women in India. Culture, Health and Sexuality 2002;4(2):207-222.
16. Golding JM, Taylor DL. Sexual Assault History and Premenstrual Distress in two General Population Samples. Journal of Women’s Health 1996;5(2):143-152.
17. Gupta GR. How men’s power over women fuels the HIV epidemic. BMJ 2002;324:183–84.
18. Heise L, Ellsberg M, Gottemoeller M. Ending Violence Against Women. Population Reports, Series L, No.
11. Baltimore, JohnHopkins University School of Public Health, Population Information Program, December 1999.
19. Hof C, Richters A. Exploring intersections between teenage pregnancy and gender violence: Lessons from Zimbabwe. African Journal of Reproductive Health 1999;3(1): 51-65.
20. IIPS and Macro International, National Family Health Survey (NFHS-3), 2005–2006, India: Chapter 15, Mumbai: IIPS and Macro International, 2007.
21. Im-em W, Kanchanachitra C, Archavanitkul K, Sexual coercion among ever-partnered women in Thailand, in: Jejeebhoy SJ, Shah I and Thapa S, eds., Sex Without Consent: Young People in Developing Countries, London: Zed Books, 2006, pp. 74–85.
22. Im-em, W. 2003. Sexual coercion among women in Thailand: Results from the WHO multi-country study on women’s health and life experiences, Presentation at the Global consultative meeting, New Delhi, India.
23. Jejeebhoy S, Santhya KG. 2003. Forced sex within marriage among young women: Evidence from South Asia, Paper presented in a consultative meeting on non-consensual sexual experiences of young people in developing Countries, New Delhi, India; 2003:22-25.
24. Joshi AM, Dhapolam E. Experiences and perceptions of marital sexual relationships among rural women in Gujrat, India. AsiaPacific Population Journal 2001;16(2):177-194.
25. Kaur R, Garg S. Addressing domestic violence against women: An unfinished agenda. Indian J Community Med 2008;33:73-6.
26. Khan ME, Townsend JW, D’Costa S: Behind closed doors: A qualitative study on sexual behaviour of married women in Bangladesh. Culture, Health and Sexuality 2002;4(2):237-256.
27. Khan ME, Townsend JW, Sinha R, Lakhanpal S. Sexual Violence within Marriage. In: Seminar. New Delhi, Population Council 1996. No. 447 Pp 32-35.
28. Kimuna SR, Djamba YK, Ciciurkaite G, Cherukuri S. Domestic violence in India: Insights from the 2005-2006 national family health survey (NFHS). J Interpers Violence 2013;28(4):773- 807.
29. Kishor S, Johnson M. Profiling domestic Violence: a MultiCountry Study. Measure DHS 2004. Available at: http://www. dhsprogram.com/publications/publication-OD31-Other-Documents.cfm (Last accessed on 23/9/2014).
30. Koenig M, Zabolkota I, Lutalo T, Nalugoda F, Wagmen J, Gray R. Coerced first intercourse and reproductive health among adolescent women in Rakai, Uganda. International Family Planning Perspectives 2004;20(4):156-163.
31. Koenig MS, Ahemed M, Hossain Mozumder ABM. Women’s status and domestic violence in Rural Bangladesh: Individualand-community level effect. Demography 2003;40(2):269-288.
32. Krishnan S, Subbiah K, Khanum S, Chandra PS, Padian NS. An intergenerational women’s empowerment intervention to mitigate domestic violence: results of a pilot study in Bengaluru, India. Violence Against Women. 2012;18(3):346–370
33. Logan TK, Cole J. The impact of partner stalking on mental health and protective order outcomes over time. Violence and Victims 2007:22:546–562.
34. Maman S, Mbwambo JK, Hogan NM, Kilonzo GP, Campbell JC, Weiss E, Sweat MD. HIV-positive women report more lifetime partner violence: findings from a voluntary counseling and testing clinic in Dar es Salaam, Tanzania. Am J Public Health. 2002;92(8):1331–1337.
35. Mane P, Gupta GR, Weiss E. Effective communication between partners: AIDS and risk reduction for women. AIDS 1994;8(1):325–331.
36. Martin SL, Tsu AO, Maitra Singh K, Kupper LL. Sexual behaviours and reproductive health outcomes: associations with wife abuse in India. The Journal of the American Medical Association 1999;28(20):1967-72.
37. Mishra A, Patne SK, Tiwari R, Srivastava DK, Gour N, Bansal M. A cross-sectional study to find out the prevalence of different types of domestic violence in Gwalior city and to identify the various risk and protective factors for domestic violence. Indian J Community Med 2014;39:21-5.
38. Parish WL, Wang T, Laumann EO, Pan S, Luo Y. Intimate partner violence in China: National prevalence, risk factors and associated health problems. International Family Planning Perspectives 2004;30(4):174-81.
39. Population council 2004. Available at: www.popcouncil.org/uploads/pdfs/popsyn/PopulationSynthesis1.pdf . (Last accessed on 20/11/2014).
40. Puri M, Cleland J. Assessing the factors sexual harassment among young female migrant workers in Nepal. Journal of Interpersonal Violence 2007;22(11):1363-1381.
41. Puri M, Shah I, Tamang J. Exploring the nature and reasons associated with sexual violence within marriage among young women in Nepal. Journal of Interpersonal Violence 2010;25(10):1873-1892.
42. Puri M, Tamang J, Shah I (2011). Suffering in silence: consequences of sexual violence within marriage among young women in Nepal. Bio Med Central Public Health 2011;11:29.
43. Randall T. Domestic violence intervention: Calls for more than treating injuries. Journal of the American Medical Association 1990;264:939–940.
44. Santhya KG, Haberland N, Ram F, Sinha RK, Mohanty SK. Consent and Coercion: Examining Unwanted Sex among Married Young Women in India. International Family Planning Perspectives 2007;33(3):124-130
45. Santhya KG, Jejeebhoy S. Young women’s experiences of forced sex within marriage: evidence from India. In Sex without consent: Young people in developing countries. Edited by S. Jejeebhoy, I. Shah and S. Thapa. New York: Zed Books; 2005. pp:59-73
46. Sharma KK, Vatsa M. Domestic violence against nurses by their marital partners: A facility-based study at a tertiary care hospital. Indian J Community Med 2011;36:222-7.
47. Stark E, Flintcraft A, Frazier W. Medicine and Patriarchal Violence: The Social Construction of Private Event. International Journal of Health Services 1979;9:461-493.
48. The protection of women from domestic violence act, 2005, Indian Laws and Bare Acts at Vakilno1.com. Available at: http:// www.vakilno1.com/bareacts/Domestic-Violence/Domestic-Violence-Act-2005.html . (Last accessed on 20/11/2014).
49. UNESCO (2009). International technical guidance on sexuality education. Paris: UNESCO. Online at http://data.unaids.org/ pub/ExternalDocument/2009/20091210_international_guidance_sexuality_education_vol_2_en.pdf (Last accessed on 05/9/2014)
50. Watts C, Zimmerman C. Violence against women: global scope and magnitude. Lancet 2002;359(9313):1232–1237.
51. Women’s Rehabilitation Centre (WOREC): Breaking the Silence: Needs Identification of Victims of Gender-based Violence. Kathmandu, Nepal; 2002.
52. World Health Organisation (WHO): World Report on Violence and Health. World Health Organization, Geneva; 2002. Available at: http://www.who.int/violence_injury_prevention/violence/world_report/en/ (Last accessed on 25/10/2014).
53. World Health Organization: WHO Multi-Country Study on Women’s Health and Domestic Violence against Women. World Health Organization, Geneva; 2005. Available at: http://www. who.int/gender/violence/who_multicountry_study/en/ (Last accessed on 24/9/2014).
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





