IJCRR - 7(17), September, 2015
Pages: 20-26
Date of Publication: 11-Sep-2015
Print Article
Download XML Download PDF
OUTCOME OF CONVENTIONAL TRABECULECTOMY WITH OR WITHOUT CATARACT SURGERY
Author: Usha B.R., M. S. Usha, M. Brinda Prasad
Category: Healthcare
Abstract:Purpose: To study the outcome of conventional trabeculectomy with or without cataract surgery in different types of glaucoma in low risk cases. Materials and Methods: 50 consecutive eyes, each undergoing conventional trabeculectomy and, 50 eyes combined with cataract surgery are included in this prospective study; each patient had a minimum period of follow-up for six months. Preoperative details of medications, visual acuity, slit lamp evaluation, applanation tonometry, cup to disc ratio and visual fields were compared with similar parameters postoperatively. \"Complete success\" was defined in this study as intraocular pressure (IOP) < 21mmHg or 30% reduction from the preoperative IOP. Latest IOP recorded in each eye has been considered for this study. Results: Postoperative mean IOP in the trab group was 13.08 + 3.52 mm Hg and in combined group it was 13.70 + 3.31 mm Hg during 100% visits, with follow ups ranging from six months to > 5 years. There was no significant difference in IOP reduction between trabeculectomy and combined groups. 87% of long-term \"Complete Success\" rate in both the groups and 76% visual outcome of > 6/18 in the combined group may be attributed to minimum rate of complications. Conclusion: Conventional trabeculectomy without using antimetabolites is successful even in the present day glaucoma management in low risk glaucoma cases, when performed with technical precision aided by vigilant postoperative care. It is equally effective and convenient when combined with cataract surgery in relevant cases.
Keywords: Glaucoma, Conventional trabeculectomy, Combined surgery, Complete success, Intraocular pressure, Antimetabolites
Full Text:
INTRODUCTION
Cairns1 in 1968, Watson and Grierson2 in 1981 popularized trabeculectomy and it is still regarded as the gold standard to which newer operations are compared. Various studies have shown that conventional trabeculectomy performed without using tissue antimetabolites or releasable sutures or laser suturelysis may yield satisfactory control of intraocular pressure (IOP) for many years3,4,5. Also patients who have financial constraints may not be able to continue with antiglaucoma medications. Conventional trabeculectomy is a safe and economic alternative for such patients, for better control of IOP, stabilization of visual field changes and optic disc damage. Glaucoma and cataract are main causes of visual impairment especially in the age group more than 60 years. Combined glaucoma and cataract surgeries may be considered in patients having glaucoma in its advanced stage with co-existing cataract6 . Despite the proved benefits of current augmented treatment with antimetabolites or shunts they are not totally taken up in developing countries because of their cost, their complexity and the need for regular follow-ups.7 A study done at Nepal mentions complications related to laser suturelysis (which requires costly equipment) like bleb leak and blebitis; early releasable sutures may have higher incidence of hypotony and bleb failure.8 Hence conventional trabeculectomy may be an ideal solution in low risk cases, at the least.
MATERIALS AND METHODS
This five year prospective study was designed to assess the outcome of conventional trabeculectomy with or without cataract surgery in various types of glaucoma at Mysore Race Club charitable Eye Hospital.
Main indications for trabeculectomy were: Failed multidrug antiglaucoma medications, eyes with C/D 0.8 to 0.9, pseudoexfoliation glaucoma, post-angle closure attacks with > 180 degree posterior synechiae, normal tension glaucoma, eyes with severe visual field defects (as per Hodapp Anderson Criteria),9 one eyed, patients from remote rural places, with low compliance, poor socioeconomic status, etc. Cases with significant cataract which precluded fundal view with reduced visual acuity (< 6/24) in presence of uncontrolled glaucoma underwent combined cataract and glaucoma surgery.
Exclusion criterion: Patients aged < 40 years, trauma, aphakia, uveitis, neovascular glaucoma, pseudophakic glaucoma, previous trabeculectomy. These were divided into two groups: Trabeculectomy (trab) group where only conventional trabeculectomy was done and, combined group where conventional trabeculectomy was combined with cataract surgery and intraocular lens (IOL) implantation. Only those eyes that had completed follow up for a minimum period of six months were included in this study. In every case details of preoperative antiglaucoma medications and their duration were noted. Each patient underwent preoperative slit lamp examination, Snellen’s visual acuity test, Goldmann applanation tonometry, gonioscopy, cup-todisc (C/D) ratio, which were compared with similar criteria postoperatively. Humphrey field analysis was done in most of the cases wherever it was possible; field test was performed four to eight weeks postoperatively in the combined group. Informed consent was obtained in all patients.
Surgical technique:
Conventional trabeculectomy was performed by two surgeons of good experience and expertise. Limbus based conjunctival flap was fashioned in upper nasal quadrant. A rectangular block of trabecular tissue was removed after creating a superficial triangular scleral flap of appropriate thickness. Meticulous suturing of scleral flap was done along with water-tight conjunctival closure with 10-0 nylon sutures. Proper postoperative care was taken in each case to detect / control hyphema, shallow anterior chamber, and inflammation, if any. Cataract surgery with IOL implantation was combined with trabeculectomy wherever indicated. Either extracapsular cataract extraction or small incision cataract surgery was performed at the same site; phacoemulsification and trab were done at two different sites. Postoperatively IOP was monitored closely after one week, two weeks, three weeks, four weeks, eight weeks, six months and 3-6 monthly thereafter and more frequently, if found necessary. Most of the cases were followed upto 4-5 years. Postoperative medication included a combination of prednisolone acetate and antibiotic eye drops in tapering doses for a period of 6-8 weeks. Early postoperative pressure spikes were treated with oral acetazolamide. Overdrainage and shallowing of anterior chamber or inflammation were managed with patching /appropriate medication. In every case IOP at the latest follow up was considered for this study. A clear corneal phaco with IOL implantation was performed if necessary, in eyes who developed cataract in the trab group subsequently and their IOP was closely monitored. Criterion of “successful outcome” in this study is defined as a postoperative IOP of < 21mm Hg or a 30% reduction of IOP when compared to the preoperative level; “complete success” is the term used when target pressure could be achieved without adding any glaucoma medication. The data was compiled and results were analyzed statistically using independent samples ‘t’- test or 2 way ANOVA, wherever relevant.
RESULTS
50 consecutive eyes of 43 patients were included for study under conventional trab group; and 50 consecutive eyes of 48 patients under the combined group. There were 11 one-eyed patients in the trab group and 14 in the combined group. Post primary angle closure glaucoma in a 50 year old female, showing middilated pupil, patchy iris atrophy and glaucomflecken. Peripheral anterior synechiae seen on gonioscopy) in more than three quadrants necessitated trabeculectomy in this case.
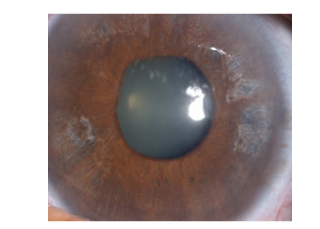
Figure 1: Post primary angle closure glaucoma in a 50 year old female, showing middilated pupil, patchy iris atrophy and glaucomflecken. Peripheral anterior synechiae seen (on gonioscopy) in more than three quadrants necessitated trabeculectomy in this case.
In the combined group small incision cataract surgery was performed in 30 eyes, extracapsular cataract extraction was done in 3 eyes, at the same site; phacoemulsification and trab were done at two different sites in 17 eyes.
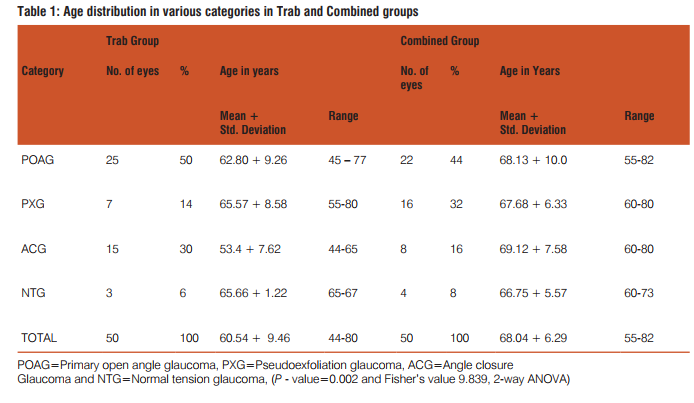
Age is a major risk factor for glaucoma. Incidence of glaucoma increases with age.10, 11
Table 1 shows number of patients included under different types of glaucoma and their mean age under each category in trab group and combined group is compared. Patients in the combined group had a higher overall mean age (68.04 + 6.29) when compared to those in the trab group (60.54 + 9.46) which is statistically significant (P = 0.002) as analyzed by 2-way ANOVA test. ACG patients were of younger age in trab group (mean 53.4 + 7.26) in contrast to those in other group / subgroups, which is statistically significant (P = 0.017). Out of 43 patients in the trab group there were 21 females; and out of 48 patients 21 females in the combined group. It was observed that all 15 eyes with ACG in trab group and 6 out of 8 eyes in the combined group were females, confirming that ACG is more common among females.
Table 2 shows preoperative and postoperative mean IOP in both the groups in all 4 categories, along with standard deviation, range and P-value.
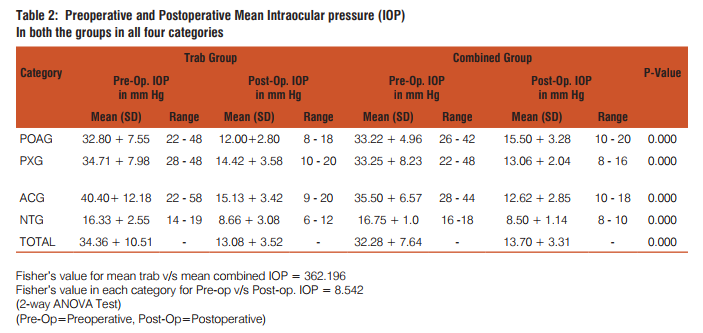
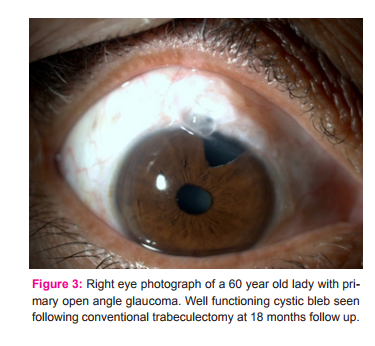
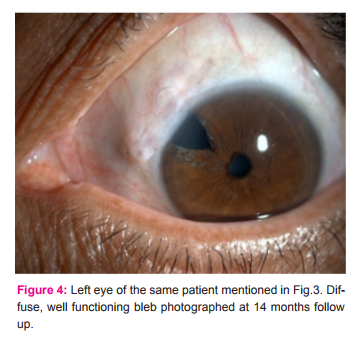
In both Trab and combined groups ACG patients were having higher IOP preoperatively. Postoperative mean IOP in both trab and combined groups at latest follow up is 13.08 + 3.52 and 13.70 + 3.31 mm Hg in both the groups respectively, when compared to the preoperative 34.36+ 10.51 and 32.28 + 7.64 mm Hg (P = 0.0000), which is highly significant, as seen also in each category (POAG, PXG, ACG and NTG), individually (P = 0.000). There is no significant difference in postoperative mean IOP after whether Trab alone or combined is done in PXG/ ACG / NTG eyes. Though the number of cases with NTG is less in this study, IOP reduced by < 50% postoperatively in all seven eyes and it maintained at same level even at sixth month follow up (8 mm Hg postoperatively when compared to preoperative 16 mm Hg). It was observed that in both the groups the postoperative mean IOP was < 16 mmHg in all categories during 100% visits, an IOP level at which visual fields are said to remain stable as mentioned in most of the studies (AGIS : 7).12 It was found that in the trab group out of 50 eyes 19 eyes were not on any antiglaucoma medication preoperatively, 24 eyes were on one or two medicines and seven eyes were on three or more drugs; corresponding figures in the combined group were 11, 27 and 12 eyes respectively. Following surgery 83 eyes did not require any glaucoma medication even when followed up for more than 5 years. One drug was started in six eyes in the trab group and, in seven eyes in the combined group between first and second year follow up, who had advanced field defects, to achieve a target pressure of < 18 mm Hg. In no case two or more drugs were needed even when followed up for 5 years. This indicates that “Complete success” was achieved in 87% of eyes in terms of IOP as defined earlier in this study. In only 13 eyes (13%) a single medication was started, which may be termed “Qualified success”. 13 It was noted that cystic bleb was present in 32 eyes, diffuse bleb in 63 eyes and flat bleb was found in five eyes. Nature of the bleb did not influence IOP in the present study.
Out of 50 eyes in the trab group visual acuity (VA) maintained postoperatively at the preoperative level in 41 eyes; preexisting cataract progressed in six eyes; 3 more eyes developed early lenticular opacities. These cases underwent clear corneal phacoemulsification with IOL implantation, with constant monitoring of IOP. In the combined group visual acuity improved in all but four eyes. 76% of eyes improved to a visual acuity of > 20/80
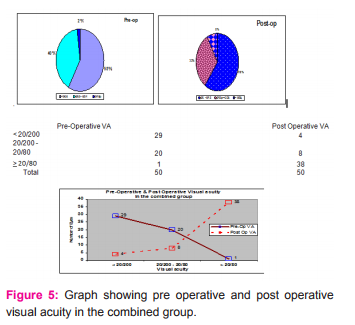
In this group four eyes had near mature cataract; so fundus was not visible. These were postoperatively found to have near total glaucomatous optic atrophy and got VA < 20/200.
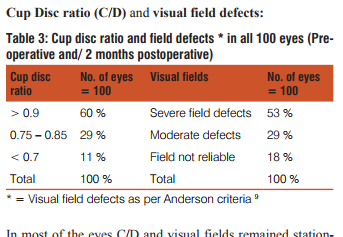
In most of the eyes C/D and visual fields remained stationery following surgery. Four eyes with near mature cataracts in the combined group were postoperatively discovered to be having near total glaucomatous optic atrophy. C/D < 0.7 was found mainly in the ACG group. 60 eyes with C/D > 0.9 were associated with severe field defects. Out of 100 eyes 62 completed five years of follow up, their glaucoma parameters being stable. 34 eyes could be followed upto 4 years post operatively and remaining 4 eyes for 3 years. Mean duration of follow up in trab and combined groups was 46.66+/-9.14 months and 48.17+/-10.12 months respectively
Details of complications noted in this study are shown in Table 4.
DISCUSSION
Rotterdam study, Roscommon, Beaver Dam, Dalby and several other studies emphasize that prevalence of glaucoma increases as age advances (above 50 years of age).10,11 In our study mean age in trab group is 60.54 +9.46 years. Pia Ehrnrooth13 observed that POAG cases had a mean age of 67.8 years. Andreas wedrich has reported that in combined surgery group mean age was 76.40 years,14 whereas in the present study it is 68.04 years. In the present study postoperative mean IOP achieved in the trab group is 13.08 + 3.52mm Hg. This is comparable to a study done by Y.A.Mutsch and F.Grehn in 99 eyes15 (14.7 mm Hg.) M.E. Gyasi at Ghana observed that postoperative mean IOP was 17.06 in 88.48% out of 191 eyes with open angle glaucoma following conventional trabeculectomy and recommended this in low risk cases.16 High success rate achieved in the present study may be due to several factors:
1. Selection of cases for surgery was restricted to low risk cases; high risk cases are supposed to have < 75% success rate following a conventional trabeculectomy.17
2. Precise operative technique plays a major role in yielding good results. IOP reduction with a limbus based conjunctival flap is supposed to be greater than with a fornix based flap.18
3. There were minimum postoperative complications in the present study which were medically managed.
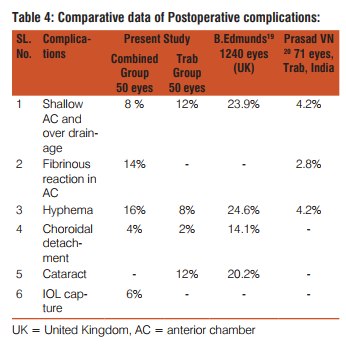
Incidence of hyphema is less when the excision of the tissueblock is anterior to the scleral spur (18% in a study by Konstas AG, 21 which is similar to our study).
4. Intensified postoperative care (IPC) has helped us to achieve target pressure comparable to surgery with antimetabolites.15
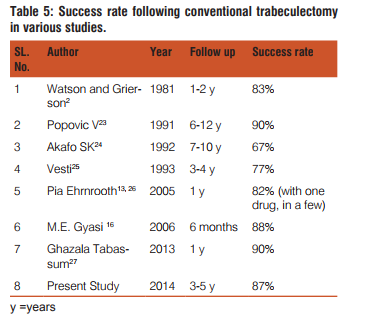
5. There were no bleb related complications in the present study because antimetabolites were not used. ME Gyasi,16 Becker - Shaffer (80-90% success rate) and many authors have obtained good results following conventional trabeculectomy in primary open angle glaucoma( POAG) (Table 5).17, 22
A combined surgery may be helpful in elderly patients especially with severe glaucoma and cataract, who may not withstand the stress of two separate surgical sessions.28 Andreas wedrich reported 91% complete success with IOP of 13.5 mm Hg in Phaco + Trab group,14 (v/s 86% success in the combined group in our study, with postoperative mean IOP of 13.7mm Hg); Chen H reported a mean IOP of 13.01 mm Hg in ECCE + Trab group and 12.63 mm Hg in Phaco + Trab group.6 Urban V reported a mean IOP of 15.3 mm Hg29 comparable with present study. Khurana AK reported postop mean IOP of 16.47 mm Hg with 93% complete success30; Edward J obtained a success rate of 88.2%31 It is recommended to observe IOP in these eyes for longer period and also to compare results of conventional trabeculectomy with wound modulated surgery.
CONCLUSION
Conventional trabeculectomy without wound modulation, with / without cataract surgery done for various types of glaucoma significantly reduces IOP postoperatively even in low risk cases. Success rate is almost equal in both trab and combined groups. Precise surgical technique and careful postoperative monitoring of every case are essential factors in obtaining a sustained reduction of IOP even for > 5 years. A combined surgery may help an elderly person with cataract in a developing country with financial constraints, to have a faster visual recovery along with good glaucoma control. 60% of eyes in our study presented with advanced glaucoma requiring trab / combined surgery between the age group of 60-70 years. This implies the requirement of efficient and economic health care delivery system for earlier detection and management of glaucoma in the community, thereby reducing severity of blindness due to glaucoma.
References:
1. Cairns JE. Trabeculectomy. Preliminary report of a new method. Am J Ophthalmol. 1968. 66:673-9.
2. Watson, P.G. and Grierson. The Place of Trabeculectomy in the Treatment of Glaucoma. Ophthalmology, 88, 175-196.
3. D’Ermo F, Bonomi L, Doro D. A critical analysis of the longterm results of trabeculectomy. Am J Ophthalmol 1979. Nov;88(5):829-835
4. K B Mills Trabeculectomy: a retrospective long-term follow-up of 444 cases. Br J Ophthalmol. 1981 Nov; 65(11): 790–795.
5. Nouri-Mahdavi K, Brigatti L, Weitzman M, Cprioli J. Outcomes of trabeculectomy for primary open-angle glaucoma. Ophthalmology. 1995 Dec; 102(12):1760-9. 6. Chen H, Ge J, LiuX, LuF. The clinical analysis of 260 combined surgery of glaucoma and cataract. Yan Ke Xue Bao (Pubmed Article in Chinese - English) 2000 Jun; 16 (2): 102 - 5.
7. Editor,: “Glaucoma in the developing world” BMJ 2006 (4 Nov.); 33 : 932
8. Kumari R., Badhu BP, Das H. “Effectiveness of combination of permanent and releasable scleral flap sutures in trabeculectomy: A randomized clinical trial”, Kathmandu University Medical Journal 2006 Vol.4; No.4, Issue 16: 419 - 425.
9. Douglas R. Anderson, Vincent Michael Patella in: Automated Static Perimetery: Chapter 7: Interpretation of a single field, 2nd ed. Mosby; 1999 page 164.
10. Klein BEK, Klein R, Sponsel WE: Prevalence of glaucoma. Ophthalmology, 1992; 99: 1499 - 504.
11. Scott Fraser, Richard Wormald: Chapter 210, Epidemiology of Glaucoma, in: Ophthalmology, Vol. 2 by Myron Yanoff, Jay S. Duker, 2nd ed. MOSBY: 2004. pp 1413 - 14.
12. The AGIS investigators. The advanced glaucoma intervention study (AGIS): 7 “The relationship between control of intraocular pressure and visual field deterioration”, Am J Ophthalmol 2000 Oct; 130(4): 429 - 40.
13. Ehrnrooth P, Lento, Puska P, Laatikainenl. Long term outcome of trabeculectomy in terms of IOP. Acta Ophthalmol Scand 2002; 80: 267 - 71.
14. Andreas Wedrich, Rupert Menapace, Ursula Redax, Panos Papapanos and Michael Amon, Cataract surgery and trabeculectomy- technique and results. International Ophthalmology 1992; Volume 16, Numbers 4-5, 409-14.
15. Y.A. Mutsch and F.Grehn. Success criteria and success rates in trabeculectomy with and without intraoperative antimetabolites using intensified post operative care (IPC) ; Graefe’s Archive for clinical and experimental ophthalmology 2000 ;Vol. 238, number 11: 884 - 891.
16. ME Gyasi, WMK Amoaku, OA Debrah, EA Awini and P Abugri. Outcome of Trabeculectomies without Adjunctive Antimetabolites. Ghana Med J. 2006 June; 40 (2): 39-44.
17. R. Rand Allingham, Shields’ Text Book of Glaucoma, chapter 40: Filtering surgery, fifth ed. Lippincott Williams and Wilkins; 2005. pp 583 - 594.
18. Sandra J. Sofinski, Pranav Amin, and R.Rand Allingham, Chapter 226: Glaucoma filtration surgery. In Principles and Practice of Ophthalmology, Albert and Jakobiec, Azar, Gragoudas; volume 4, 2nd ed. W.B. Saunder company; 2000. pp 2959-60
19. B.Edmunds, JR Thompson, JF Salmon: Clinical study: The national survey of Trabeculectomy III-Early and late complications; Eye 2002; 16: 297 - 303.
20. Prasad VN, Narain M, Bist HK, Khan MM. Trepano - trabeculectomy (a combined operation for glaucoma); Indian J Ophthalmol 1984; 32: 73 -75.
21. Konstas AG, Jay JL, Modification of trabeculectomy to avoid postoperative hyphaema: “The guarded anterior fistula” operation; Br J Ophthalmol 1992; 76: 353.
22. Robert L Stamper, Marc F. Lieberman, Michael V. Drake In: Becker - Shaffer’s Diagnosis and therapy of the Glaucomas, Part VIII, chapter 36, 7th ed., Mosby ; 1999: pp 591 - 92.
23. Popovic V, Sjostrand J. Long term outcome following trabeculectomy: Retrospective analysis of intraocular pressure regulation and cataract formation. Acta Ophthalmol (Copenh) June 1991; 69: 299-304
24. Akafo SK, Goulstine DB, Rosenthal AR. Long-term, post trabeculectomy intraocular pressures. Acta Ophthalmol (Copenh) 1992; 70: 312.
25. Vesti E. Filtring blebs: Follow up of trabeculectomy. Ophthalmic surgery 1993; 24:249-255.
26. Pia Ehrnrooth: “Long term outcome of trabeculectomy in primary open angle Glaucoma and Exfoliation Glaucoma”: Department of Ophthal, university of Helsinki, Finland; 2005:17 -32. (http:// ethesis.helsinki.fi / julkaisut / laa / kli in vk /ehrnrooth)
27. Ghazala tabassum, Imran Ghayoor et al. The effectiveness of conventional trabeculectomy in controlling intra ocular pressure in our population. Pak J Ophthalmol 2013 Vol.29 No.1: 26-30.
28. Per Julius Nielsen, MD: Combined Small-Incision Cataract Surgery and Trabeculectomy- A prospective study with 1 year of Follow-up; Ophthalmic surg Lasers 1997; volume 28(1): 21-29.
29. Urban V, Kamman MT, Sturmer JP, Glaucoma and Cataract: Combined operation or, trabeculectomy first and cataract extraction later? Klin Monatsbl Augenheilkd (pubmed article in German – English) 2000 Feb; 216 (2): 105 –11.
30. Khurana AK et al. Combined SICS and trabeculectomy; Nepal J Ophthalmol 2011; 3(5): 13 – 18.
31. Edward J Rockwood. Outcomes of combined cataract extraction, lens implantation, and trabeculectomy surgeries. Am J Ophthalmol 2000 Dec; 130 (6): 704 –11.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





