IJCRR - 14(7), April, 2022
Pages: 24-31
Date of Publication: 05-Apr-2022
Print Article
Download XML Download PDF
Preoperative Anxiety in Cardiac Surgery Patients
Author: Adhyapak Sadhana
Category: Healthcare
Abstract:Introduction: People with high level of anxiety experience significant distress & impairment in interpersonal as well as social functioning. There are many medical conditions where patients develop high levels of anxiety. Anxiety with surgery is associated with autonomic changes, supplementary doses of anesthetic drugs, increased level of postoperative pain & more chances of postoperative nausea & vomiting. To prevent & treat anxiety effectively, one must assess level of anxiety accurately. A nurse can assess anxiety & reduce it to a manageable & comfortable level. Aims: A study was conducted to anticipate preoperative anxiety among patients undergoing cardiac surgeries & to identify dimensions of anxiety. Methodology: A quantitative approach was used for this cross-sectional study. Content validity of the tool was done&reliability was calculated using Karl Pearson's coefficient of correlation. The sample was calculated by 80 % confidence level with 5% error. Total sample was 80 patients admitted in cardiothoracic ward. Samples were selected by convenient sample technique. Anxiety level was identified with the help of Amsterdam Preoperative Anxiety & Information Scale. Along with anxiety level, researcher also tried to find the possible causes of anxiety. Result: Descriptive data was analyzed & association between variables was identified. 82.5% of patients were males & 17.5 % were females. Most of them i.e., 86.3 % underwent coronary artery bypass graft (CABG) & 13.8% underwent valvular surgeries. It was seen that 16.3% of patients had high level of anxiety related to anesthesia, 27.5% of patients had high level of anxiety related to surgery & overall high anxiety level was seen in 21.3% of patients. The association was seen with gender, previous experience of surgery & duration of hospitalization. Most common causes of anxiety identified were worried about postoperative pain & family concern. Conclusion: Nurses can identify triggers of anxiety, recognize the symptoms of onset of anxiety & intervene before patient reaches to panic stage.
Keywords: Preoperative, Anxiety, Cardiac surgery, Coronary artery, Valvular surgery, Bypass graft
Full Text:
Introduction
Anxiety is a strong concern for something happening. Many times, anxiety disturbs activities of daily living. People with a high level of anxiety experience significant distress & impairment in interpersonal as well as social functioning. There are many medical conditions where patients develop high levels of anxiety. Anxiety with surgery is associated with autonomic changes, supplementary doses of anesthetic drugs, increased level of postoperative pain & more chances of postoperative nausea & vomiting. A cohort study was conducted & Amsterdam Preoperative Anxiety & Information Scale was used to assess anxiety. The various sources of anxiety were related to anesthesia, surgery & other related factors. Anxiety scores were seen on the higher side with higher education & patients undergoing general anesthesia. The association was also seen with female gender. 1
Leopold Eberhart et al analyzed anxiety in preoperative period & also found predictors of anxiety. It was a cross-sectional study where anxiety was assessed with the help of Amsterdam Preoperative Anxiety & Information Scale. 40.5% patients showed high level of anxiety & total preoperative anxiety score was 9.9. Main concern for fear was mistaken by the anesthetist, as fatigue & drowsiness. It was seen that gender, positive & negative anesthesia experience predicted anxiety subscales.2 Ghogiang Gu3 determined the relationship between coronary surgeries & symptoms of anxiety & depression in coronary heart disease patients. Patients were asked to complete the Hospital Anxiety & Depression Scale & separate questionnaire before & after surgery. Coronary surgeries were found to be significantly associated with symptoms of anxiety & depression. It was also seen that symptoms related to anxiety increased one day before & after surgery.
According to Sigdel S4 One of the main risk factors for the development of anxiety is the presence of cardiac disease & surgery. Total 140 patients were investigated with the help of the State-Trait Anxiety Inventory (STAI)& preoperative anxiety was seen in 58.5% of patients. Female gender & previous anesthesia exposure were identified as risk factors.
Cardiovascular disease is associated with increased risk of morbidity in the short & long term. One of the major treatments for cardiovascular disease is surgery. Today there are various surgical options available for patients to relieve cardiac symptoms & improve quality of life. But during any form of treatment, patient-reported outcome is the most important aspect.5 Under patient-reported outcomes, patient himself/herself assesses the various physical & psychological symptoms. Anxiety is one of the important reactions noted in patients waiting for surgeries. Increased level of anxiety is associated with negative consequences of postoperative outcome & rehabilitative process.6 To prevent & treat anxiety effectively, one must assess level of anxiety accurately. Nurse can assess anxiety & reduce it to a manageable & comfortable level. The nurses’ goal is to assist patients with anxiety to develop adaptive coping strategies.
Jose Prado7 Olivares et al. assessed level of anxiety using State-Trait Anxiety Inventory in patients undergoing cardiac surgeries. Coronary artery bypass graft (CABG) was performed on 47% of patients & valvular surgeries were performed on 26.7% of patients. Total 60 samples were included in the study. Moderate to high level of anxiety was seen in 80% of patients. First surgical intervention was found to be related with level of anxiety. It was concluded that patients undergoing cardiac surgeries should be given well-framed program through individualized education. Similarly, Jitendra Jeenger et al.8 found the prevalence of depression & anxiety after first myocardial attack. 60 cases of diagnosed acute myocardial infarction were compared with 60 healthy individuals. Patients with myocardial infarction were seen to be enduring from depression and anxiety symptoms. 40% of myocardial infarction patients showed depressive episodes & 35% showed anxiety symptoms.
Objectives
The main objectives of the study were to assess preoperative anxiety among patients undergoing cardiac surgery, to identify the association between preoperative anxiety & demographic variables & to find possible causes of preoperative anxiety.
Methodology
Research design
A quantitative approach was used for this cross-sectional study. The study population was patients admitted for cardiac surgeries i.e., coronary artery bypass graft & valvular surgeries. Sample was calculated by 80 % confidence level with 5% error. Total sample was 80 patients admitted in cardiothoracic ward. Samples were selected by convenient sample technique.
Development of tool
Tool included three sections. Section I included demographic details like age, gender, education, occupation, marital status, type of family, BMI, previous experience of surgery & type of surgery.
Section II was Amsterdam Preoperative Anxiety & Information Scale (APAIS) to assess level of anxiety. Boker A9 et al. evaluated different scales of anxiety i.e., state-trait anxiety inventory, Amsterdam Preoperative Anxiety & Information Scale & Visual analogue scale. It was seen that it was an advantage to use APAIS as patients could easily answer the questions. Consistent correlation of APAIS was seen with other anxiety scales. So, the investigator decided to use this scale.
Amsterdam Preoperative Anxiety & Information Scale consists of 6 questions with a Likert scale ranging from 1 (not at all) to 5 (extremely). Out of these four questions show level of anxiety & two questions identify patient’s need for information. Researcher identified anxiety related to anesthesia, anxiety related to surgery, total anxiety & patient’s need for information. Researcher decided the scoring system to divide anxiety in mild, moderate & severe levels.
Section III was a self-administered questionnaire. This included 10 yes/ no type questions related to possible causes of preoperative anxiety. All the questions were easily understood & readily answered by the sample.
Ethical consideration
The researcher got approval from the institutional research & recognition committee & institutional ethical committee. Written informed consent was taken from each sample before data collection.
Validity & reliability
Content validity was done from 12 experts of related field. Reliability was done using the test-retest method. The formula used was Karl Pearson’s coefficient of correlation. It was found to be 0.99. So, the tool was considered reliable & was retained. A pilot study was done on 10 samples to assess the feasibility of the study. It was done in the month of December 2020.
Data collection
Data was collected from January 2021 to June 2021. It was a private charitable hospital from Pune. Data was collected on the day of surgery prior to surgery. Patients took approximately 10 minutes to answer the questions. They completed it in the wards before they were shifted to the operation theatre.
Inclusion & exclusion criteria
Patients admitted only for coronary artery bypass graft & valvular surgeries were included & patients undergone emergency surgeries were excluded from the study. It was assumed that patients waiting for cardiac surgeries present high levels of anxiety & assessment of preoperative anxiety have better postoperative outcomes.
Results
Section I
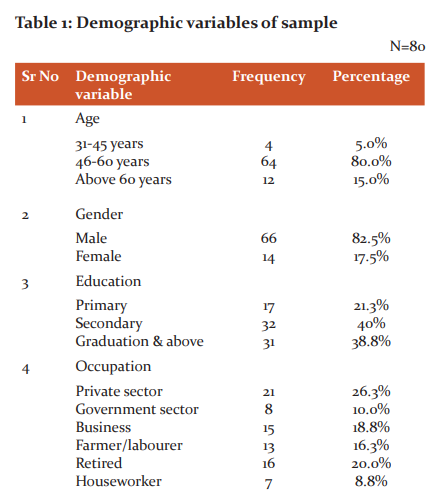
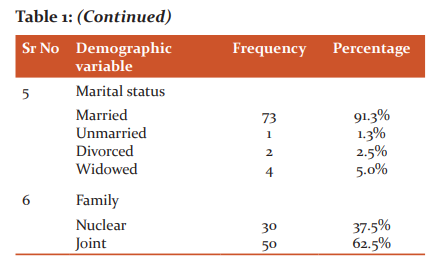
Above table indicates that 5% of the patients undergoing cardiac surgery were in the age group of 31-45 years, 80% of them were in 46-60 years and 15% of them were above 60 years. 82.5% of them were males and 17.5% of them were females.
21.3% of them had primary education, 40% of them had secondary education and 38.8% of them were educated up to graduation and above.26.3% of them were working in private sector, 10% of them were from government sector, 18.8% of them had business, 16.3% of them were farmers/laborers, 20% of them were retired and 8.8% of them were houseworkers.91.3% of them were married, 1.3% of them were unmarried, 2.5% of them were divorced and 5% of them were widow.37.5% of them were from nuclear family and 62.5% of them were from joint family.
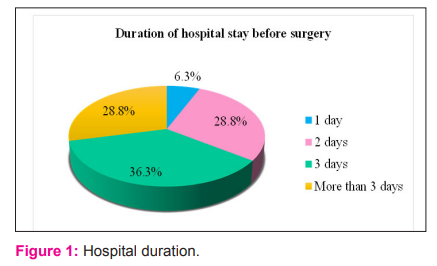
Fig 1 shows that 6.3% of them were admitted in the hospital for 1 day before surgery, 28.8% of them were admitted for 2 days before surgery, 36.3% of them 3 days before surgery and 28.8% of them for more than 3 days before surgery.

Table No 2 shows that 20% of them had history of chronic illness, 31.3% of them had history of previous surgery & 17.5% of them used substance. It is also seen that 86.3% of them underwent CABG and 3.8% of them had valvular surgery.
Section II - It deals with analysis of data related to preoperative anxiety among patients undergoing cardiac surgery.
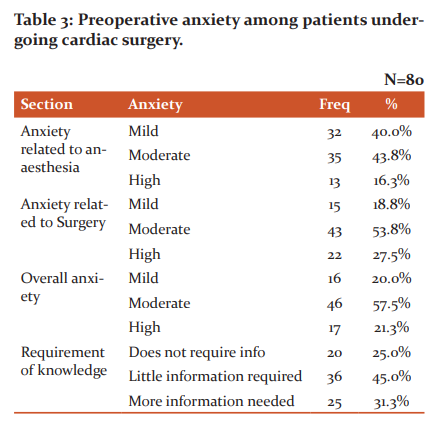
Table No 3 suggests that 40% of the patients had mild preoperative anxiety related to anaesthesia, 43.8% of them had moderate preoperative anxiety and 16.3% of them had high preoperative anxiety related to anaesthesia.
18.8% of the patients had mild preoperative anxiety related to surgery, 53.8% of them had moderate preoperative anxiety and 27.5% of them had high preoperative anxiety related to surgery.
20% of the patients had mild overall preoperative anxiety, 57.5% of them had moderate overall preoperative anxiety and 21.3% of them had severe overall preoperative anxiety.
25% of them did not require information, 45% of them needed litter information and 31.3% of them needed more information.
Section III
Analysis of data related to association between preoperative anxiety & demographic variables.
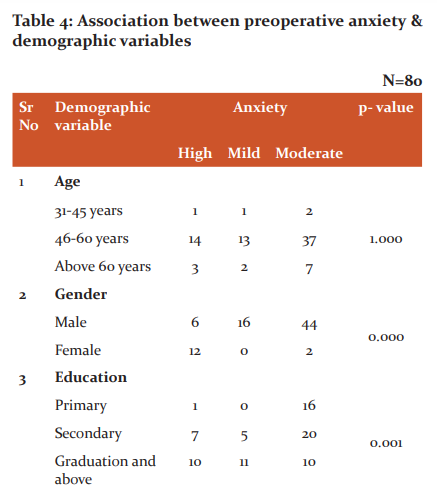


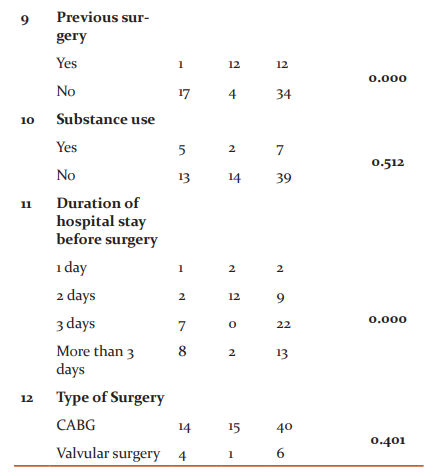
Table No 4 indicates that Since p-values corresponding to gender, education, occupation, family type, BMI, previous surgery, and duration of hospital stay before surgery were small (less than 0.05), the demographic variables gender, education, occupation, family type, BMI, previous surgery and duration of hospital stay before surgery were found to have significant association with the preoperative anxiety among patients undergoing cardiac surgery.

Fig 2 shows that 66.3% of the patients undergoing cardiac surgery were worried about post-operative pain. 36.3% of them were anxious about pain during surgical pain. 2.5% of them were afraid of unknown. 30% of them anxious about the improvement after surgery. None of them were anxious about post-operative nausea and vomiting. 21.3% of them were anxious about the complications. 2.5% of them were anxious about the loss of job. 62.5% of them were anxious about the family concern. 23.8% of them were worried about economic conditions.
Discussion
Mehdi F et al.10 evaluated preoperative anxiety & susceptible components in cardiac surgery patients. Patients between the age group of 18-65 were assessed for anxiety & association was found with various demographic variables. Females & patients with opioid addiction exhibited high level of anxiety (p<0.001). No association was seen with factors like family support & underlying disease. In present study association was seen with factors like gender, education, occupation, family type & hospital stay before surgery.
C. Ramesh et al.11 studied preoperative anxiety among patients with coronary artery bypass graft surgery. State – trait anxiety inventory was used to assess anxiety level. It was found that 84% of patients presented with preoperative anxiety. Chi-square test (11.57, p<0.001) was used to find association & gender was found to be associated with preoperative anxiety. In present study Amsterdam Preoperative Anxiety & Information Scale was used to assess anxiety &Fisher exact test was applied to find association between preoperative anxiety & demographic variables.
JoaquinH P et al.12 identified preoperative anxiety level in patients posted for heart surgery. Visual analogue scale was used to measure anxiety level. Anxiety was seen in 28% of patients & similar findings are seen in present study. But coronary artery bypass graft (OR 3.026, p<0.001) was associated with preoperative anxiety which is contradictory to present study where no association was seen with type of surgery.
Priya Gangadharan et al.13 conducted a descriptive study on 20 admitted patients posted for elective surgery. The anxiety was measured using State Trait Anxiety Inventory. Findings indicated that 60% of patients had high level of anxiety, 30% had moderate anxiety & low anxiety was seen by 10% of patients. Various levels of anxiety were associated with marital status. In these cases, nurses can plan interventions accordingly.
Anna R14et al. evaluated intensity of stress & level of anxiety in heart surgery patients. Intensity of stress was measured by standardized questionnaire in 58 patients admitted for heart surgery.
Mistakes by anesthetist was the main reason for anxiety.2 In present study postoperative pain & family concern were the main causes of anxiety. In another study common causes found were death worry, chances of complications & unpredicted postoperative consequences. In Present study 30% patients were worried about improvement after surgery & 21.3% were worried about complications after surgery.
High levels of anxiety 11,2,15 is seen in patients waiting for surgeries. Different studies have identified level of anxiety as well as possible causes of preoperative anxiety. It is seen that there are variables like gender, previous surgical experience, social support has association with preoperative anxiety. Different causes like inability to recover, harm from health professionals, fear of unknown, blood transfusion fear is found.
Shiho Takenaka16 measured mean value of intraoperative nociception in patients undergoing thoracic surgeries. It was found that nociception during intraoperative period was likely to be associated with preoperative anxiety. Even Rodrigues17 identified association of preoperative anxiety symptoms with hemodynamic instability in the postoperative period.
Association of anxiety was found with low level of education, potential cardiac function & sequence of surgery. In present study also association was seen with previous surgery.3
If preoperative anxiety is evaluated, the factors that would cause anxiety also can be explored. According to identified factors causing anxiety, intervention programme can be planned for patients undergoing cardiac surgeries.7
Janesson18discussed about factors that affected patient’s recovery in postoperative period. It was seen that those patients who were involved in decision making & to whom adequate preoperative knowledge was provided, had better satisfaction level in postoperative period. It was also suggested that patient’s literacy skills should be identified before surgery because that affects recovery in postop period.
Antonia K19 conducted randomized control trial on 395 patients where 205 patients were in intervention group. Preoperative education was given by nurses to intervention group & anxiety was assessed on admission day, before surgery & before discharge. State trait Anxiety Inventory was used to assess anxiety level. It was observed that level of anxiety was decreased before surgery in intervention group. Even there was decrease in mean anxiety score during follow up period. It was concluded that education delivered by nurses in preoperative period reduced anxiety & complications in postoperative period. Niknejad R20 inspected effect of orientation tour on anxiety in preoperative period & it was seen that preorientation tour has reduced anxiety level in CABG patients. Such interventions can be planned by nurses working in cardiothoracic ward. Ping G21 revealed effectiveness of preoperative education among cardiac surgery patients. Extensive review of literature was done & it was found that some studies proved that preoperative education improved physical as well as psychological recovery of patients. So, training to staff nurses regarding preoperative education becomes greatest important. Similarly Pazar B22 investigated effect of preoperative education regarding patient comfort & anxiety to patients undergoing cardiac surgeries. A randomised control trial was performed on 200 patients & it was seen that those patients who received preoperative education exhibited low levels of anxiety.
Asilioglu K23educated cardiac surgery patients about preoperative anxiety & patients in the experimental group had lower anxiety scores than patients in the control group.
Mousari M24Nurses should be aware of complementary therapies & they should be able to use these supportive & nonpharmacological interventions to help patients reduce preoperative anxiety levels. Similarly Joke Bradt25 patients who are waiting for surgery often have higher levels of anxiety. This may end up with prolonged wound healing & dismissive physical effects. It may even increase the risk of infection. Drugs help to reduce anxiety levels, but nurses can plan & make use of some nonpharmacological measures & control anxiety levels. Nurses can plan individualized care plan as each individual is unique & presents individual character & coping style.26
Conclusion
After analysing objectives of this study, it can be concluded that it is crucial for each patient to recognize about his or her own anxiety. Nurses are the ones who can assess anxiety of patients by different ways & help patients use variety of coping techniques to relieve it. Coping strategies like reading, verbalizing, physical activity reduces level of anxiety. Individualized education is also important. This enhances level of confidence. Even though similar studies are done previously, present study suggests that factors like female gender, occupation, type of family & hospital duration should be given more concern to reduce post operative problems. Different findings may be seen with different type of sample & dissimilar hospital environment. Education to nurses regarding preoperative assessment will give more fruitful services & better patient outcome. Patients with high anxiety have more desire to gain the knowledge. So, high risk patients must undergo proper evaluation & management to minimize anxiety levels.
Nursing implications
Preoperative assessment is required to distin
References:
-
Celik F., Edipoglu I.S. Evaluation of preoperative anxiety and fear of anesthesia using APAIS score. Eur J Med Res 23, 41 (2018). https://doi.org/10.1186/s40001-018-0339-4
-
Eberhart L., Aust H., Schuster M. Preoperative anxiety in adults - a cross-sectional study on specific fears and risk factors. BMC Psychiatry 20, 140 (2020). https://doi.org/10.1186/s12888-020-02552-w
-
Gu G, Zhou Y, Zhang Y, Cui W. Increased prevalence of anxiety and depression symptoms in patients with coronary artery disease before and after percutaneous coronary intervention treatment. BMC Psychiatry. 2016 Jul 22;16:259. doi: 10.1186/s12888-016-0972-9. PMID: 27450548; PMCID: PMC4957885.
-
Sigdel S, Ozaki A, Basnet M, Kobashi Y, Pradhan B, Higuchi A, Uprety A. Anxiety evaluation in Nepalese adult patients awaiting cardiac surgery: A prospective observational study. Medicine (Baltimore). 2020 Feb;99(9):e19302. doi: 10.1097/MD.0000000000019302. PMID: 32118748; PMCID: PMC7478669.
-
Adam J Z , “Measures of Preoperative Anxiety”, Aanesthesiology Intensive Therapy, 2019; 51(1):64:69 doi:10.5603/AIT.2019.0013
-
https://pdfs.semanticscholar.org/8bed/773045cee544a29d69a0691226c3899ad8bb.pdf
-
Jose PO & Elena CS, “Preoperative anxiety in patients undergoing cardiac surgery”, Diseases, 2019 Jun; 7(2): 46 doi: 10.3390/diseases7020046
-
Jeenger J, Wadhwa S, Mathur DM, “Prevalence of depression & anxiety symptoms in first attack myocardial infarction patients of Mewar region: A cross sectional study”, Int J Cur Res Rev, volume 6 (07), April 2014, pg no 79-85
-
Boker A., Brownell L. Donen N, “The Amsterdam preoperative anxiety and information scale provides a simple and reliable measure of preoperative anxiety”, Can J Anesth 49, 792–798 (2002). https://doi.org/10.1007/BF03017410
-
Fathi M, Alavi SM, Joudi M, Joudi M, Mahdikhani H, Ferasatkish R et al. “Preoperative anxiety in candidates for heart surgery”, Iran J Psychiatry Behav Sci, 2014, 8(2), 90-96
-
Ramesh C, Baby S. Nayak, Pai VB, George A, George LS, Devi ES, Pre-operative anxiety in patients undergoing coronary artery bypass graft surgery – A cross-sectional study, Int. J. Afr. Nurs. Sci., Volume 7, 2017, Pages 31-36, ISSN 2214-1391, https://doi.org/10.1016/j.ijans.2017.06.003.
-
Hernández-Palazón J, Fuentes-García D, Falcón-Araña L, Roca-Calvo MJ, Burguillos-López S, Doménech-Asensi P, Jara-Rubio R. Assessment of Preoperative Anxiety in Cardiac Surgery Patients Lacking a History of Anxiety: Contributing Factors and Postoperative Morbidity. J Cardiothorac Vasc Anesth. 2018 Feb;32(1):236-244. doi: 10.1053/j.jvca.2017.04.044. Epub 2017 Apr 26. PMID: 28803768, pg no 236-244.
-
Gangadharan P, Assiri R A M, Assiri F A A, “Evaluating the level of anxiety among pre-operative patients before elective surgery”, Int J Cur Res Rev, volume 6, issue 22, November 2014, pg no 37-41
-
Rosiek A, Kornatowski T, Rosiek-Kryszewska A, Leksowski L, Leksowski K, “Evaluation of stress intensity & anxiety level in preoperative period of cardiac patients”, BioMed Res. Int., vol 2016, article ID 1248396, 8 pages, 2016. https://doi.org/10.1155/2016/1248396
-
Bedaso A., Ayalew M. Preoperative anxiety among adult patients undergoing elective surgery: a prospective survey at a general hospital in Ethiopia. Patient Saf Surg 13, 18 (2019). https://doi.org/10.1186/s13037-019-0198-0
-
Takenak S,, “Preoperative anxiety & intraoperative nociception in patients undergoing thoracic surgery”, J. Surg. Res., 2020 May;249:13-17. doi: 10.1016/j.jss.2019.12.017.
-
Rodrigues HF, Furuya RK, Dantas RAS, Rodrigues AJ, Dessotte CAM, “Association of preoperative anxiety and depression symptoms with postoperative complications of cardiac surgeries.”, Rev Lat Am Enfermagem. 2018 Nov 29;26:e3107. doi: 10.1590/1518-8345.2784.3107. PMID: 30517589; PMCID: PMC6280174.
-
Jaensson M., Dahlberg K., Nilsson U. Factors influencing day surgery patients’ quality of postoperative recovery and satisfaction with recovery: a narrative review. Perioper Med 8, 3 (2019). https://doi.org/10.1186/s13741-019-0115-1
-
Kalogianni A, Almpani P, Vastardis L, Baltopoulos G, Charitos C, Brokalaki H. Can nurse-led preoperative education reduce anxiety and postoperative complications of patients undergoing cardiac surgery? Eur J Cardiovasc Nurs. 2016 Oct;15(6):447-58. doi: 10.1177/1474515115602678. Epub 2015 Aug 24. PMID: 26304701.
-
Niknejad R, Mirmohammad-Sadeghi M, Akbari M, Ghadami A. “Effects of an orientation tour on preoperative anxiety in candidates for coronary artery bypass grafting: A randomized clinical trial.” ARYA Atheroscler. 2019 Jul;15(4):154-160. doi: 10.22122/arya.v15i4.1806. PMID: 31819748; PMCID: PMC6884734.
-
Guo P, “Preoperative education interventions to reduce anxiety & improve recovery among cardiac surgery patients”, J. Clin. Nurs., 2015 Jan; 24(1-2):34-46 doi: 10.1111/jocn.12618.
-
Pazar B, Iyigun E, “The effects of preoperative education of cardiac patients on haemodynamic parameters, comfort, anxiety and patient-ventilator synchrony: A randomised, controlled trial.” Intensive Crit Care Nurs. 2020 Jun;58:102799. doi: 10.1016/j.iccn.2020.102799. Epub 2020 Jan 25. PMID: 31987684.
-
Asilioglu K, Celik SS, “The effect of preoperative education on anxiety of open cardiac surgery patients.” Patient Educ Couns. 2004 Apr;53(1):65-70. doi: 10.1016/S0738-3991(03)00117-4. PMID: 15062906
-
Mousavi M N, Zakerimoghadam M, Esmaeili M, Kazemnejad A. Effects of Nurse-Led Intervention on Patients' Anxiety and Sleep Before Coronary Artery Bypass Grafting. Crit Care Nurs Q. 2018 Apr/Jun;41(2):161-169. doi: 10.1097/CNQ.0000000000000195. PMID: 29494371.
-
Bradt J, Dileo C, Shim M. Music interventions for preoperative anxiety. Cochrane Database of Systematic Reviews 2013, Issue 6. Art No.:CD006908. DOI:10.1002/14651858.CD006908.pub2. Accessed 21 July 2021.
-
Domar AD, Everett LL, Keller MG. Preoperative anxiety: is it a predictable entity? Anesthesia and Analgesia. 1989 Dec;69(6):763-767.
-
Polit, Beck, “Nursing Research”, Lippincott William and Wilkins, 9th edition, 2012, pg no 50-55, 264
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





