IJCRR - 14(6), March, 2022
Pages: 80-85
Date of Publication: 15-Mar-2022
Print Article
Download XML Download PDF
Non-Echoplanar Diffusion-Weighted Imaging and 3D Fiesta Magnetic Resonance Imaging Sequences with High Resolution Computed Tomography Temporal Bone in Assessment and Predicting the Outcome of Chronic Suppurative Otitis Media with Cholesteatoma
Author: Divya Meenu Preetha, Yuva Balakumaran, Pravitha
Category: Healthcare
Abstract:Introduction: Cholesteatomas are lesions that develop in pneumatized areas of the temporal bone, such as the middle ear and mastoid, or both, and are extremely rarely detected in the external auditory canal. Because it has benefits over CT, diffusion-weighted imaging MRI (DWI-MRI) can be a useful technique in the identification of cholesteatoma. Image distortion and artefacts are less visible with non-echo planar imaging DWI techniques than with other DWI techniques.
Aims and Objectives: 1) To assess the usefulness of HRCT scan in Chronic suppurative otitis media (CSOM) with cholesteatoma in depicting the status of the middle ear structures. 2) To correlate HRCT findings of temporal bone with surgical findings in Chronic suppurative otitis media (CSOM) with cholesteatoma with respect to the following parameters: Presence or absence of cholesteatoma, Extent of cholesteatoma, Status of ossicular chain, Integrity of the facial canal, Detection of erosions or dehisence in the bony labyrinth, and Detection of erosions or dehisence in the dural or sinus plates. 3) Comparison with Non-Echo planar imaging diffusion-weighted for presence or absence of cholesteatoma. 4) 3D FIESTA Magnetic resonance imaging with 3D reconstruction of membranous vestibule and cochlea for better delineating associated complications.
Materials and Methods: Total 40 patients of clinically suspected CSOM with cholestaetoma were enrolled for this study. All patients were scanned using a non-contrast High-resolution computed tomography technique and MRI. HRCT findings were noted according to the proforma. MRI DWI was recorded as either positive or negative for cholesteatoma & directly correlated with post-surgical presence or absence of cholesteatoma.3D FIESTA for detection of membranous labyrinthine erosion/defect was correlated with surgical findings of bony labyrinthine erosions.
Results: Cholesteatoma was shown to be common in the third decade of life in our study. The most often implicated middle ear structures in our investigation were the epitympanum, aditus, and antrum. The most often eroded ossicle is the stapes, followed by the incus. The tympanic section of the facial canal is the most often affected segment, while the posterior semicircular canal is the most commonly degraded of the bony labyrinth structures.
Conclusion: HRCT temporal bone, in combination with non-echoplanar DWI MRI and 3D Fiesta, can help with accurate diagnosis and pre-operative assessment of cholesteatoma.
Keywords: Non-echoplanar diffusion, 3D fiesta magnetic resonance imaging, High resolution computed tomography, Temporal bone, Chronic suppurative otitis media, Cholesteatoma
Full Text:
Introduction:
Cholesteatomas are lesions that develop in pneumatized areas of the temporal bone, such as the middle ear and mastoid, or both, and are extremely rarely detected in the external auditory canal. They are non-neoplastic, locally invasive masses that often appear as unilateral lesions.
Cholesteatomas are categorized into three types: congenital, which affects only children, acquired, which affects both adults and children, and unclassifiable, which is a cholesteatoma whose origin cannot be established correctly .1
The extent of a cholesteatoma is still difficult to identify with current imaging techniques because of its makeup, especially in ears that have already undergone surgery. The standard modality has been computed tomography (CT), which allows for the detection of bone alterations.
Diffusion weighted imaging MRI (DWI-MRI) can be a useful technique in the identification of cholesteatoma since it has benefits over CT, such as a shorter examination duration and no requirement for a contrast medium injection prior to the test.2 Because of its high sensitivity and specificity, DWI-MRI may detect tiny collections of keratin debris that would otherwise be misinterpreted as fluid or edematous mucosa on CT and is capable of detecting recurrent cholesteatoma.2,3
Three-dimensional fast imaging with steady-state acquisition (3D-FIESTA) pictures were introduced recently. 3D-FIESTA imaging can provide significantly better spatial resolution and excellent picture contrast. It takes less time to acquire images than a traditional MRI scan and does not require contrast media.4,5
Materials and methods:
This prospective study was conducted at Radio-Diagnosis at Vinayaka Missions Kirupananda Variyar Medical College Hospital, Salem. Total 40 Patients with cholestaetoma and clinically suspected CSOM were enrolled in this study. Before enrolling in the trial, all patients gave their written informed consent.
Inclusion criteria were patients with clinically suspected atticoantral type of chronic suppurative otitis media of all age groups and either sex; patients willing to give consent.
Patients with previous ear surgeries, patients with a history of temporal bone trauma, patients with neoplastic development involving the middle ear, and patients unwilling to give consent were all excluded.
A complete history of ear discharge, deafness, tinnitus, earache, vertigo, headache, and fever was collected and recorded in a systematic order, with specific attention to any accompanying symptomatology suggestive of any imminent or already established chronic otitis media complication.
All patients were scanned using a non-contrast HRCT on GE revolution CT scanner. The axial sections were acquired in a supine, neutral position, parallel to the superior orbital-meatal line consecutively. Scanning was done extending from the petrous pyramid to the mastoid in spiral mode. The gantry rotation time was 1 s and acquisition parameters were 6 × 1 mm with slice collimation of 1 mm, slice thickness of 2 mm, and increment of 2 mm. Multiplanar reconstruction in axial, coronal, and sagittal planes was performed at a slice thickness of 1.25 mm and an increment of 0.8 mm.
MRI was performed on a 1.5-T (Siemens) with use of the standard Head Matrix coil. Axial propeller DWI for all cases and 3D Fiesta was performed in selective cases and when required.
HRCT findings were noted according to the proforma. Intraoperative findings of mastoid exploration surgery were recorded and were taken as standard for determination of sensitivity and specificity of HRCT scan for various study variables. The data were analyzed using descriptive statistic tools like proportions. MRI DWI was recorded as either positive or negative for cholesteatoma & directly correlated with post surgical presence or absence of cholesteatoma.3D FIESTA for detection of membranous labyrinthin erosion/defect was correlated with surgical findings of bony labyrinthin erosions.
Results:
In present study, 65% of the respondents are male and 35% of the respondents are female.30% of the respondents are less than 20 years, 25% of the respondents are in the age group 21-30, 15% of the respondents are in the age group 31-40 and 22.5% of the respondents are in the age group 41-50 and 7.5 % of the respondents are above 50. Majority of patients had Ear discharge 36(90%), 32(80%) had earache, 22(55%) had hearing loss, 10(25%) had facial weakness and 5(12.5%) had Giddiness, vomiting, others. In majority of patients had cholesteatoma on right side 27(67.5%) and 13 (32.5%) on left side. Since the p-value for the are less than (p-values <0.05) the null hypothesis is rejected. In our study there is significant correlation between the extent of involvement and erosion of Aditus, antrum, facial recess, sinus tympani, Hypotympanum, Eustachian tube, beyond the middle ear cleft, incus, stapes, tympanic and mastoid segment, lateral and posterior semicircular canal of cholesteatoma in HRCT and the surgical findings.
Cholesteatoma was shown to be common in the third decade of life in our study. The most often implicated middle ear structures in our investigation were the epitympanum, aditus, and antrum. The most often eroded ossicle is the stapes, followed by the incus. The tympanic section of the facial canal is the most often affected segment, while the posterior semicircular canal is the most commonly degraded of the bony labyrinth structures.
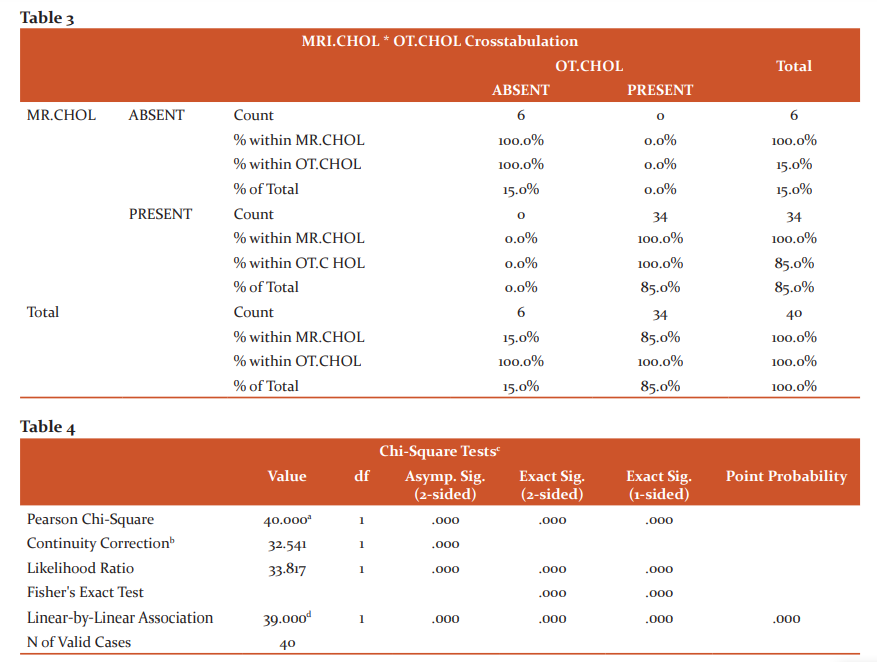
The results of HRCT with non-echoplanar DWI and 3D FIESTA were compared to surgical findings and revealed a statistically significant correlation.
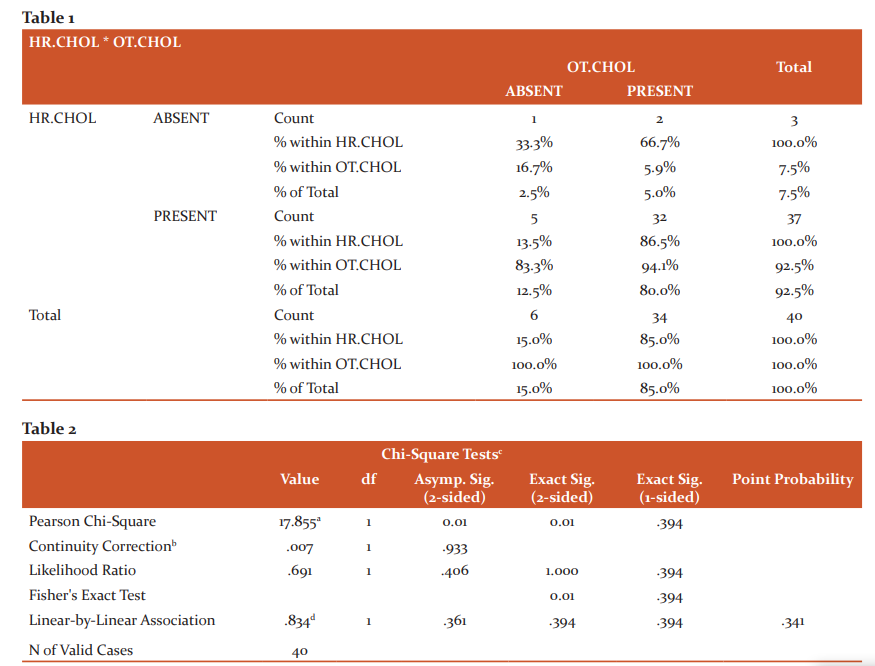
Since the p-value for the Cholesteatoma are less than (p-values <0.05) the null hypothesis is rejected. It infers that there is an Association between the status of Cholesteatomain HRCT and the surgical findings.
Image 1: Near-total opacification of middle ear cavity, filling the epitympanic recess, facial recess, and sinus tympani, as well as round and oval window niches.

Image 2: Diffusion-weighted MRI shows marked restricted diffusion of the middle ear and mastoid lesions bilaterally in a case of bilateral cholesteatoma
Discussion:
The usual imaging approach for the temporal bone is a high-resolution computed tomography (HRCT) scan. Axially and coronally direct projections were used.
In the present study 65% of the respondents are male and 35% of the respondents are female, which is in agreement with other case studies.6,7
30% of the respondents are less than 20 years, 25% of the respondents are in the age group 21-30, 15% of the respondents are in the age group 31-40 and 22.5% of the respondents are in the age group 41-50 and 7.5 % of the respondents are above 50, The peak age group is variable from 20-50 years in literature.8-10
The majority of patients had Ear discharge 36(90%), 32(80%) had earache, 22(55%) had hearing loss, 10(25%) had facial weakness and 5(12.5%) had Giddiness, vomiting, others. In the majority of patients had cholesteatoma on the right side 27(67.5%) and 13 (32.5%) on the left side, which is variable in the literature.8,9
In this study, there is an Association between the status of Cholesteatoma in HRCT and the surgical findings. Similar findings were reported in a study by Leighton et al.,11 who found that a CT scan of the temporal bone had a high predictive value for diagnosing cholesteatoma, and in another study by Gaurano and Joharjy,12 who found that a pre-operative CT scan had a 97 percent correlation with surgical and histopathological findings.
The HRCT scan may also properly detect cholesteatoma in the great majority of patients, according to N W C Chee and T Y Tan.13 In contrast, Firas Q et al discovered that HRCT had a sensitivity of 80% and a specificity of 48% in distinguishing cholesteatoma from chronic mucosal illness.14 Cholesteatoma was identified in 30% of instances when soft tissue mass and bone degradation were present, according to Jackler et al.15
In our study Cholesteatoma was shown to be common in the third decade of life in our study. The most often implicated middle ear structures in our investigation were the epitympanum, aditus, and antrum. The most often eroded ossicle is the stapes, followed by the incus. The tympanic section of the facial canal is the most often affected segment, while the posterior semicircular canal is the most commonly degraded of the bony labyrinth structures.
Knowing the state of the ossicular chain prior to surgery would help the surgeon to properly advise the patient on the level of hearing that could be achieved following surgery. Patients with intact stapes, for example, have better hearing results than those who do not have stapes.16
In our study, there is a significant correlation between the extent of involvement and erosion of Aditus, antrum, facial recess, sinus tympani, Hypotympanum, Eustachian tube, beyond the middle ear cleft, incus, stapes, tympanic and mastoid segment, the lateral and posterior semicircular canal of cholesteatoma in HRCT and the surgical findings. However, it's important to keep in mind that the scan may exaggerate the degree of the disease since it can't always tell the difference between cholesteatoma and granulation tissue.10
The use of echo-planar diffusion-weighted (DWI) MR images has improved MR imaging approaches for identifying cholesteatoma. 17,18 3D Fiesta indicates deterioration of the membrane labyrinth, which is not seen on HRCT, which solely evaluates the bone labyrinth and hence provides a preoperative insight before to surgery. The surgical findings of bony labyrinthine erosions of semicircular canals corresponded well with 3D Fiesta for membranous labyrinthine erosion/defect (100 percent sensitivity and specificity).
Conclusion:
HRCT temporal bone, in combination with non-echoplanar DWI MRI and 3D Fiesta, can help with accurate diagnosis and pre-operative assessment of cholesteatoma by showing the extent of the illness, and the integrity of most middle ear structures, and disease consequences.
Acknowledgment: This study was supported byVMKV Medical college, Salem.
Conflict of Interest Statement: NIL
References:
1. Yung M, Tono T, Olszewska E, Yamamoto Y, Sudhoff H, Sakagami M, et al. EAONO/JOS Joint consensus statements on the definitions, classification and staging of middle ear cholesteatoma. J Int Adv Otol. 2017;13:1–8.
2. Henninger B, Kremser C. Diffusion-weighted imaging for the detection and evaluation of cholesteatoma. World J Radiol. 2017;28:217–222.
3. Corrales CE, Blevins NH. Imaging for evaluation of cholesteatoma: current concepts and future directions. Curr Opin Otolaryngol Head Neck Surg. 2013;21:461–467.
4. Erdogan N, Altay C, Akay E, Karakas L, Uluc E, Mete B, et al. MRI assessment of internal acoustic canal variations using 3D-FIESTA sequences. Eur Arch Otorhinolaryngol. 2013;270:469–475.
5. Rigby PJ. Comparison of FIESTA and gadolinium-enhanced T1-weighted sequences in magnetic resonance of acoustic schwannoma. Radiographer. 2006;53:11–21.
6. Chee NWC, Tan TY. The value of pre-operative high-resolution CT scans in cholesteatoma surgery. Singapore Med J 2001;42(4):155-159.
7. Jackler KR, Dillon PW, Schindler AR. Computed tomography in suppurative ear disease: A correlation of surgical and radiographic findings. Laryngoscope 1984;94(6):746-752.
8. Barath K, Huber AM, Stampfli P, Varga Z, Kollias S. Neuroradiology of cholesteatomas. AJNR 2010;10.3174:1-9.
9. Gaurano LJ, Joharjy AI. Middle ear cholesteatoma:characteristic findings in 64 patients. Ann Saudi Med(online) 2004;24(6):442-447.
10. Mafee F M, Levin CB, Applebaum LE, Campos M, James FC.Cholesteatoma of the middle ear and mastoid: A comparison of CT scan and operative findings. Otolaryngologic clinics of North America 1998;21(2):265-292.
11. Leighton SE, Robson AK, Anslow P, Milford CA. The role of CT imaging in the management of chronic suppurative otitis media. Clin Otolaryngol Allied Sci 1993; 18: 23-9
12. Gaurano LJ, Joharjy AI. Middle ear cholesteatoma: characteristic findings in 64 patients. Ann Saudi Med 2004;24(6):442-447.
13. Chee NWC, Tan TY. The value of pre-operative high-resolution CT scans in cholesteatoma surgery. Singapore Med J 2001;42(4):155-159.
14. Alzoubi FQ, Odat HA, Al-balas HA, Saeed SR. The role of preoperative CT scan in patients with chronic otitis media. Eur Arch Otorhinolaryngol 2009; 266:807–9.
15. Jackler RK, Dillon WP, Schindler RA. Computed tomography in suppurative ear disease: A correlation of surgical and radiographic findings. Laryngoscope 1984; 94: 746-52.
16. Leighton SE, Robson AK, Anslow P, Milford CA. The role of CT imaging in the management of chronic suppurative otitis media. Clin Otolaryngol Allied Sci 1993; 18: 23-9.
17. De Foer B, Vercruysse JP, Bernaerts A, Maes J, Deckers F, Michiels J, et al. The value of single-shot turbo spin-echo diffusion-weighted MR imaging in the detection of middle ear cholesteatoma. Neuroradiology2007;49:841–48.
18. Williams MT, Ayache D, Alberti C, Héran F, Lafitte F,. Detection of postoperative residual cholesteatoma with delayed-contrast-enhanced MR imaging: initial findings. Eur Radiol2003;13:169–74.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





