IJCRR - 14(6), March, 2022
Pages: 64-70
Date of Publication: 15-Mar-2022
Print Article
Download XML Download PDF
A Comparative Study of the Effectiveness of Anticonvulscants in the Treatment of Tinnitus
Author: Anagha Rajguru, Kaenat Ahmed, Yarlagadda Lakshmi Sravya, Samiksha Karna
Category: Healthcare
Abstract:Introduction: Tinnitus has defined perception of an audiological sensory impulse in the absence of any external force. There are various causes considered for the pathophysiology of tinnitus but none are established. Carbamazepine is a commonly used anti-epileptic drug that functions by depressing the CNS response to excitatory stimuli. Gamma aminobutyric acid (GABA) is the major inhibitory neurotransmitter throughout the central nervous system and is also expressed in the inner ear. Piracetam is a commonly used anti-epileptic that is known to increase cerebral blood flow and perfusion.
Methods: A group of 80 patients were evaluated by taking a detailed history and a subjective assessment of the tinnitus using Tinnitus Handicap Inventory Questionnaire. The patients were followed up for 3 months and were assessed with Pure Tone Audiometry both pre and post treatment to evaluate which drug is better. The patients were randomized into 3 groups and one control group. Each group consisted of 20 patients.
Results: The study consisted of 46 males and 34 females. A significant difference was seen when the results of group A and C were compared with p-value 0.00512, 0.00512 and 0.0083 and U value 0, 0 and 1 showing improvement from severe to moderate, moderate to mild and mild to normal. A comparison of group A and D showed a significant change from severe to moderate, moderate to mild and mild to normal with p-value 0.00512, 0.00512 and 0.0512 respectively and U values 0, 0 and 0 respectively.
Conclusions: In our study, we concluded that use of Piracetam helps in reducing tinnitus and the treatment should continue as long it persists. Thus, Piracetam and Gabapentin are effective as a modality of treatment in suppressing tinnitus according to this study. We hope that our outcomes will be helpful for patients suffering from chronic tinnitus.
Keywords: Tinnitus, Hearing loss, Antiepileptics, Gabapentin, Piracetam, Vascularity
Full Text:
INTRODUCTION:
Tinnitus is defined perception of an audiological sensory impulse in the absence of any external force. It is considered to be a symptom rather than a disease and presents differently in each patient in characteristics and cause. There are various causes considered for the pathophysiology of tinnitus but none are established. Although it is most commonly associated with acoustic or cranial trauma, presbycusis, systemic or metabolic disorders, otological infections, arthritis, or pharmacological interactions, it may be present in patients without any other ear complaints. It has a prevalence of about 10-25% and is seen in adults from all walks of life.
Tinnitus can present variably in different patients. Some may perceive a low background humming while others may complain of loud disruptive noise interfering with day-to-day conversations. It is classified in two ways: subjective or objective. Subjective is the kind of sound that is audible to the patient only, while the objective is when the examiner too can hear the sound. It is usually due to vascular causes such as AV malformations or glomus jugulare. A simple examination by listening through a stethoscope can help differentiate the two.
It is usually associated with some audiological impairment. Hearing loss associated with tinnitus may be conductive, sensory or central depending on the pathology causing the symptom. An audiogram in a patient complaining of tinnitus may thus be a useful investigation to help single out the cause. However, even in today’s day, there is no investigation or test that leads to the cause and hence the management of tinnitus. Therefore, the primary area of effort has been to alleviate the symptoms and improve the quality of life. Tinnitus retraining therapy is a habituation-based therapy in order to make the patient comfortable with the symptom and lead a productive life. It is based on the idea that combining educational counseling and sound therapy to reduce the patient’s anxiety and uneasiness. 1
Carbamazepine is a commonly used anti-epileptic drug that functions by depressing the CNS response to excitatory stimuli. It acts by binding with voltage-gated sodium channels and stabilizes it in the inactive state. It, therefore, acts by reducing neural firing.3-6
Gamma-aminobutyric acid (GABA) is the major inhibitory neurotransmitter throughout the central nervous system and is also expressed in the inner ear. When GABA binds to the GABAA receptor, it opens the associated chloride (Cl–) channels and allows a flow of Cl– into the neuron. Thus, GABA hyperpolarizes the neuronal membrane and makes the cell less reactive to the excitatory neurotransmitters. Tinnitus has been hypothesized to be the result of spontaneous hyperactivity at one or multiple levels in the auditory pathway, and this means that a reduction in GABA levels could theoretically result in increased spontaneous activity in the auditory pathway and contribute to the sensation of tinnitus.
Piracetam is a commonly used anti-epileptic that is known to increase cerebral blood flow and perfusion.7-9
Tinnitus is a symptom of pathology rather than a disease. There are various probable mechanisms of action that were studied over the years.
(a) Abnormal afferent excitation at a cochlear level due to
i) Mechanical tinnitus based on spontaneous otoacoustic emissions
ii) Glutamate neurotoxicity
iii) Enhanced sensitivity of NMDA and non-NMDA receptors
iv) Abnormal ion channel conductance calcium channel dysfunction
(b) Efferent dysfunction/reduction of GABA effect
(c) Alteration of spontaneous activity and tonotopic reorganization.
There are many treatment modalities that have been tried with varied results depending on the patients and the underlying pathologies. Antidepressants, GABA analogs, Calcium channel blockers, Prostaglandin blockers and ginkgo Biloba extracts are some of the medical treatments that have been tried. Surgical modalities such as cochlear destruction and the auditory nerve section have been tried with very little success. 10-11
There are no reliable means of curing tinnitus at its source. Current efforts thus aim to reduce the effect of tinnitus on health-related quality of life, with some evidence for the efficacy of cognitive-behavioral therapy. Tinnitus retraining therapy (TRT), an internationally recognized habituation-based treatment grounded in the neurophysiological model of tinnitus, also aims to reduce the effect of tinnitus on health-related quality of life. Tinnitus retraining therapy combines tinnitus-specific educational counseling (TC), synonymous with directive counseling, and low-level broadband sound therapy (ST) to habituate the patient to perceived tinnitus so as to lessen the patient's associated negative emotional reactions (eg, annoyance or anxiety) and improve the patient's quality of life.12
Materials and Methods
This study was conducted between June 2020 and July 2021 on patients between the ages 20 years to 60 years of both sexes that presented with a history of chronic idiopathic tinnitus to Krishna Institute of Medical Science, Karad.
A detailed history was taken and a subjective assessment of the tinnitus using the Tinnitus Handicap Inventory Questionnaire. Clinical examination, auditory assessment and imaging were done wherever appropriate. The patients were followed up for 3 months and were assessed with Tinnitus Handicap Inventory Questionnaire and Pure Tone Audiometry both pre and post-treatment to evaluate which drug is better. The patients were randomized into 3 groups and one control group. Group A consisted of patients that were given B complex capsules once a day. Group B patients were given tb Carbamazepine 200mg thrice a day. Group C patients were given Piracetam 800mg thrice a day. Group D patients were given Gabapentin 1800mg/ day divided into doses. Each group consisted of 20 patients. Thus 80 patients were studied in this study.
Inclusion Criteria:
1. Minimum age 20 yrs
2. Tinnitus for a minimum of 6 months
3. Cochlear and retrocochlear pathology
Exclusion Criteria:
1. Tinnitus due to systemic vascular or diabetic disease, anxiety, depression.
2. Tinnitus due to external and middle ear causes.
3. Meniere disease, Vestibular schwannoma or cerebellopontine angle tumors.
RESULTS
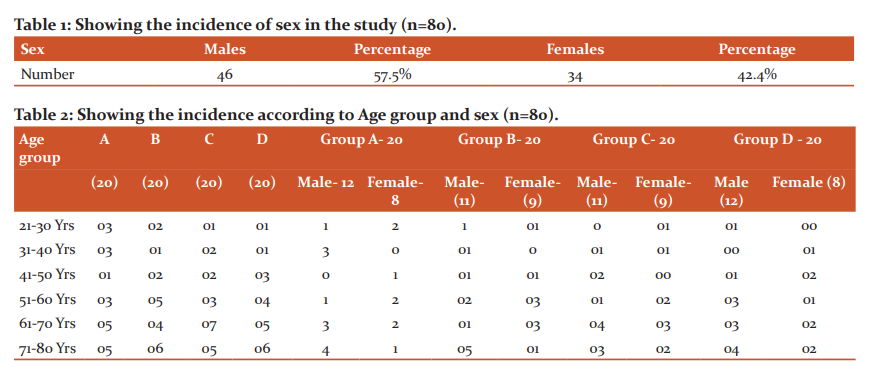
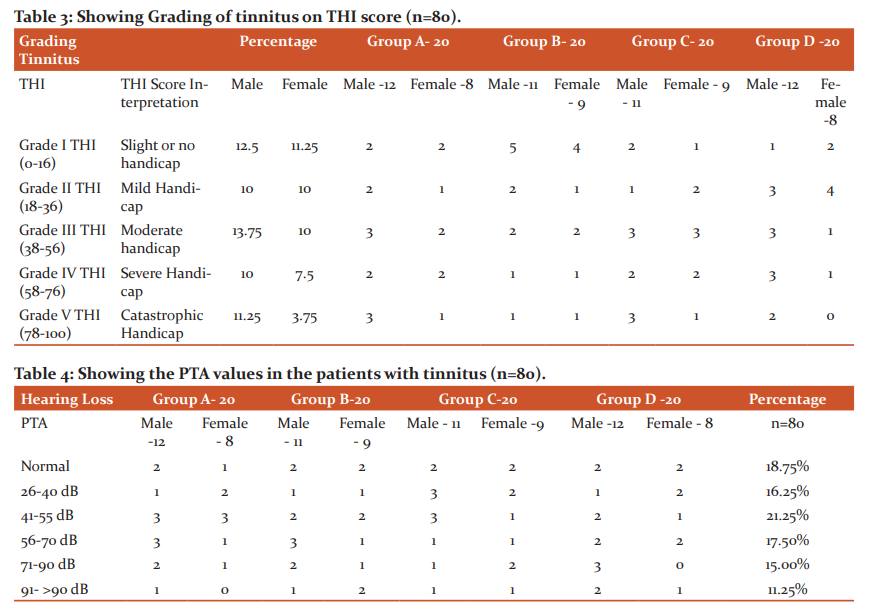
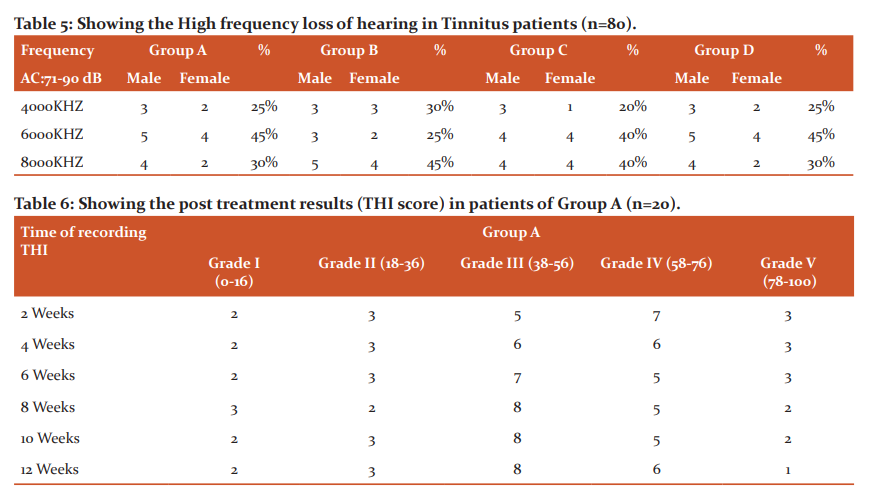
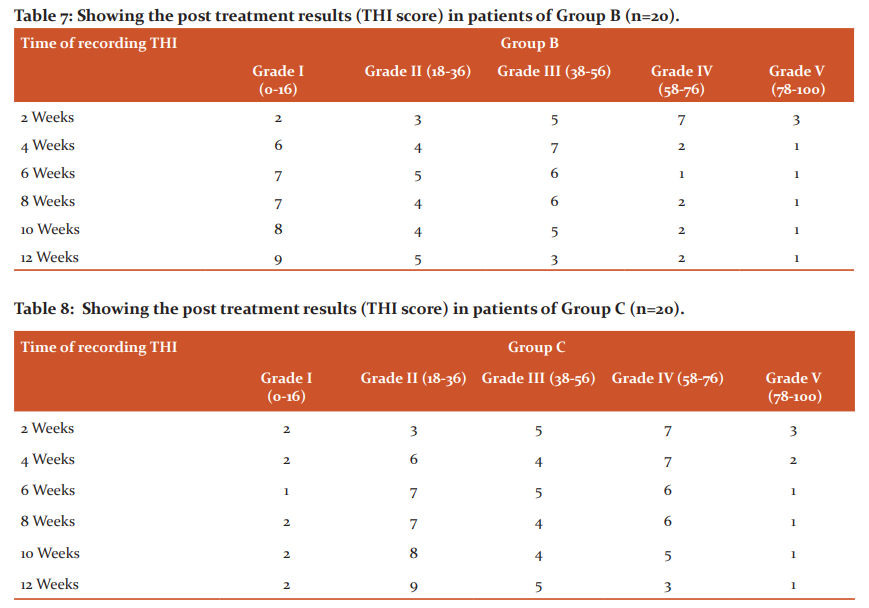
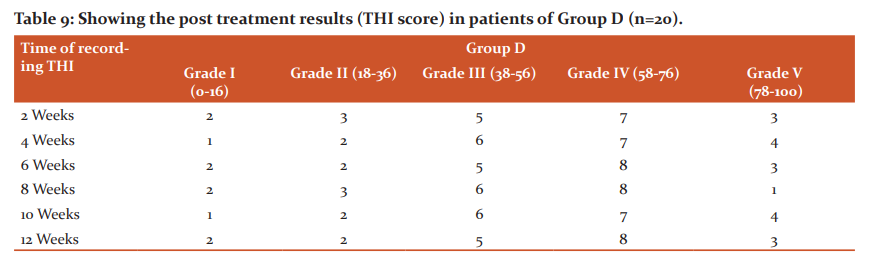
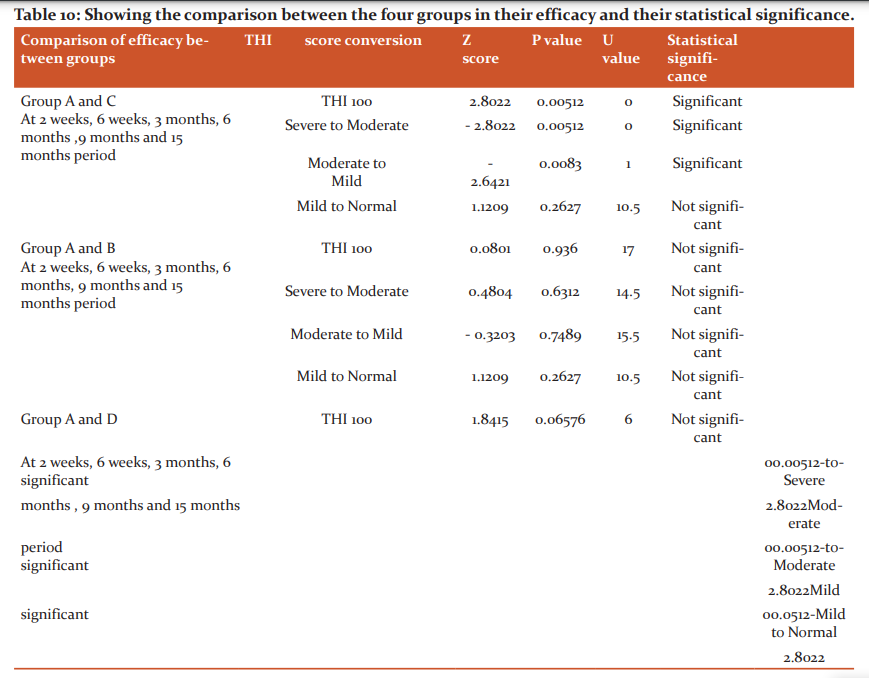
This study was conducted in the Out-Patient of the Department of ENT with 80 patients. The study consisted of 46 males and 34 females. The study group was divided into group A, B, C and D randomly. Each group had 20 members assigned randomly. Group A and D consisted of 12 males and 8 females and 11 males and 9 females in group B and group C respectively. All patients that were included were cases of idiopathic chronic tinnitus and were explained the premise of the study in detail. All patients were rated according to the tinnitus handicap inventory on the day of inclusion in the study. Group A consisted of 4(M-2, F-2) that had grade I and 3(M-2, F-1), 5(M-3, F-2), 4(M-2, F-2) and 4 (M-3, F-1) scoring grade II, III, IV and V respectively. Group B consisted of 9(M-5, F-4) that had grade I and 3(M-2, F-1), 4(M-2, F-2), 2(M-1, F-1) and 2 (M-1, F-1) scoring grade II, III, IV and V respectively. There were 3 patients with grade I and II and 6 patients with grade III, 4 patients with grade IV and V in group C. There were 3 patients with grade I, 7, 4, 4 and 2 with grade II, III, IV and V respectively in group D. All patients also underwent pure tone audiometry to record any hearing loss if present. Group A had 3 patients with normal hearing, 3 with 26-40db hearing loss, 6 with 41-55db hearing loss, 4 with 56-70 db hearing loss, 3 with 71-90 db hearing loss and 1 with >90 db hearing loss. Group B had 4, 1, 4, 4, 3 and 3 with normal, 26-40 db hearing loss, 41-55 db hearing loss, 56-70 db hearing loss, 71-90 db hearing loss and > 90 db hearing loss respectively. Group C had 4, 5, 4, 2, 3 and 2 with normal, 26-40 db hearing loss, 41-55 db hearing loss, 56-70 db hearing loss, 71-90 db hearing loss and > 90 db hearing loss respectively. Group D had 4, 3, 3, 4, 3 and 3 with normal, 26-40 db hearing loss, 41-55 db hearing loss, 56-70 db hearing loss, 71-90 db hearing loss and > 90 db hearing loss respectively. In all there were 18.75 % patients with normal hearing, 16.25%, 21.25%, 17.50%, 15.00% and 11.25% with 26-40db hearing loss, 41-55 db hearing loss, 56-70 db hearing loss, 71-90 db hearing loss and > 90 db hearing loss respectively. THI score was recorded over a span of 12 weeks and the results were compared as explained in the tables seen below. The results were compared using software SPSS 22.0 and the results were analysed and explained in table stated below. A significant difference was seen when the results of group A and C were compared with p-value 0.00512, 0.00512 and 0.0083 and U value 0, 0 and 1 showing improvement from severe to moderate, moderate to mild and mild to normal. A comparison of group A and D showed a significant change from severe to moderate, moderate to mild and mild to normal with p value 0.00512, 0.00512 and 0.0512 respectively and U values 0, 0 and 0 respectively.
DISCUSSION:
Tinnitus is an abnormal perception of sound without an external mechanical or electrical stimulant. Tinnitus is one of the frequent otological complaints reflecting an abnormality in perception which may be subjective or objective. There are local and systemic factors causing tinnitus. Among three-quarters of persons with tinnitus, the main cause is unknown (idiopathic). This study was done to ascertain the percentage of patients who had relief or reduction of symptoms by using Piracetam, Carbamazepine and Gabapentin and to compare whether Piracetam, Carbamazepine or Gabapentin is better in reducing tinnitus in a selected placebo-controlled group of patients. We studied a series of 80 patients with chronic tinnitus over a period of 2 years at the department of ENT, KIMS, Karad. The first study group comprised of 20 patients and was administered with Placebo which consisted of B complex tablets once daily for three months. It was considered the control group. Group B was administered Carbamazepine 200mg thrice daily for 3 months. Group C comprising of 20 patients was administered Piracetam 800mg thrice daily for 3 months. And group D was administered with 600mg of gabapentin three times a day for 3 months. The results were recorded and studied extensively to draw conclusions. All four groups were matched by the distribution of age, sex and duration of tinnitus. In our study maximum numbers of patients were seen in the age group of 71- 80 years and 61-70 years with a mean 57.2 years and standard deviation of 15.656. This is comparable to a study by Scherer et al. in 2019. (1) The treatment pure tone audiogram findings were compared before and after and the results were compared. The patients were also compared on the basis of their response to the THI. A specific comparison was done to compare the response of the drugs in group A with group B, C and D. A significant difference was seen between group A and C and A and D with p values 0.00512, 0.00512 and 0.0083 and 0.00512, 0.00512 and 0.0512 respectively. This is in congruence with a study by Simha et al. (13) and Aazh et al. (2) Similarly there was a significant improvement in hearing in those patients who had sensorineural hearing loss when treated with Piracetam. Those patients treated with Carbamazepine also showed a reduction in post-treatment THI score, but it was not statistically significant. Gabapentin is an effective modality of treatment of tinnitus showing significant improvement in the group of patients with sever to moderate hearing loss. Thus, in our study we concluded that use of Piracetam helps in reducing tinnitus and also improves sensorineural hearing loss in patients with tinnitus and the treatment should continue as long as tinnitus persists. Carbamazepine was not found to be effective in reducing tinnitus. Thus, Piracetam and Gabapentin are effective as a modality of treatment in suppressing tinnitus according to this study.
CONCLUSION:
Tinnitus does not represent disease itself but instead is a symptom of a variety of underlying diseases. Otologic causes include noise-induced hearing loss, presbycusis, otosclerosis, otitis, impacted cerumen, sudden deafness, Meniere’s disease, and other causes of hearing loss. Because tinnitus is a subjective symptom, we used the subjective scale—the Tinnitus Handicap Index—as the only parameter. In our study, we concluded that use of Piracetam helps in reducing tinnitus and also improve sensorineural hearing loss in patients with tinnitus and the treatment should continue as long as tinnitus persists. Carbamazepine was not found to be effective in reducing tinnitus. Thus, Piracetam and Gabapentin are effective as a modality of treatment in suppressing tinnitus according to this study. We hope that our outcomes will be helpful for patients suffering from chronic tinnitus.
Acknowledgment: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to the authors/editors/publishers of all those articles, journals and books from which the literature for this article has been reviewed and discussed.
Source of funding: none
Conflict of Interest: none
Authors’ Contribution:
Dr.AnaghaRajguru: lead researcher and guide
Dr.Kaenat Ahmed: second author and corresponding author
Dr.Lakshmi SravyaYarlagadda: third author
Dr. Samiksha Karna: forth author and data corresponding
Ethical Clearance: KIMSDU/IEC/17/2019
References:
-
Scherer R, Formby C. Effect of Tinnitus Retraining Therapy vs Standard of Care on Tinnitus-Related Quality of Life. JAMA Otolaryngology–Head & Neck Surgery. 2019;145(7):597.
-
Aazh H, El Refaie A, Humphriss R. Gabapentin for Tinnitus: A Systematic Review. AJOA. 2011;20(2):151-158.
-
Penner MJ. An estimate of the prevalence of tinnitus caused by spontaneous otoacoustic emissions. Archives of otolaryngology-Head and Neck Surgery.1990; 116:418-23.
-
Pujol R.Lateral and medial efferents: A double neurochemical mechanism to protect and regulate inner and outer hair cell function in the cochlea. British Journal of Audiology.1994; 28:185-91.
-
d’Aldin C, Eybalin M, Puel JL, Charachon G, Ladrech R, Renard N et al. Synaptic connections and putative functions of the dopaminergic innervation of the guineapig cochlea. European Archives of Otorhinolaryngology.1995; 252:270-4.
-
Bobbin RP, Jastboff PJ, Fallon M, Littman T. Nimodipine, an L-channel Ca++ antagonist, reverses the negative summating potential recorded from the guinea pig. Hearing Research.1990; 46:277-88.
-
. Dobie RA. Clinical trials and drug therapy for tinnitus. In: Snow J, ed. Tinnitus: Theory and Management. Hamilton, Ontario, Canada: BC Decker; 2004:266-277.
-
.Parnes SM. Current concepts in the clinical management of patients with tinnitus. Eur Arch Otorhinolaryngol. 1997;254(9-10):406-409. doi:10. 1007/BF02439968
-
. Martinez-Devesa P, Perera R, Theodoulou M, Waddell A. Cognitive behavioural therapy for tinnitus. Cochrane Database Syst Rev. 2010;(9): CD005233.
-
. Jastreboff PJ. Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neurosci Res. 1990;8(4):221-254. doi: 10.1016/0168-0102(90)90031-9
-
Gold SL, Formby C, Gray WC. Celebrating a decade of evaluation and treatment: the University of Maryland Tinnitus & Hyperacusis Center. Am J Audiol. 2000;9(2):69-74. doi:10.1044/1059-0889 (2000/014)
-
Jastreboff PJ, Hazell JWP. Treatment of tinnitus based on a neurophysiological model. In: Vernon J, ed. Tinnitus and Relief. Boston, MA: Allyn & Bacon; 1998:201-217.
-
Simha V, Ravishankar S. N Comparative Study to Determine the Efficacy of Piracetam over Carbamazepine in the Treatment of Idiopathic Tinnitus. International Journal of Innovative Research in Medical Science (IJIRMS). 2017 ;02(07):1015-1017.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





