IJCRR - 7(18), September, 2015
Pages: 01-05
Date of Publication: 20-Sep-2015
Print Article
Download XML Download PDF
ALTERED LIPID PARAMETERS AND THEIR RELATIONSHIP WITH THYROID STIMULATING HORMONE IN SUBCLINICAL HYPOTHYROIDISM
Author: Bhavesh Sadariya, Suman Jain, Sonal Sogani
Category: Healthcare
Abstract:Background: Subclinical hypothyroidism (SCH) is a common thyroid disease affecting large population of the world. Diversit persists regarding the level of lipid parameters in patients with SCH. Aim and Objectives: Aim of the present study was to estimate the level of lipid parameters in patients with subclinical hypothyroidism of Udaipur population and to see their relationship with TSH values. Materials and Methods: The present study was conducted on 75 patients of subclinical hypothyroidism and 100 euthyroid. Fasting venous blood was collected from each participant and analyzed for thyroid profile (T3, T4 and TSH) and lipid parameters (total cholesterol-TC, triglyceride-TG and high density lipoprotein - HDL). Low density lipoprotein (LDL) and very low density lipoprotein (VLDL) were calculated by using the Friedewald's formula. Results: Mean values of total cholesterol, triglyceride, LDL, VLDL, TC/HDL ratio and LDL/HDL ratio were significantly higher in SCH patients as compared to euthyroid. Mean of Serum HDL was also higher in SCH patients than euthyroid, but was not statistically significant. All lipid parameters were positively correlated with TSH values in SCH patients. Mean values of TC, TG, HDL, LDL and VLDL were higher in female patients as compared to male patients, but were not statistically significant. Conclusion: Subclinical hypothyroidism is associated with dyslipidemia having raise in all lipid parameters, which may increases the risk of atherosclerosis and cardiovascular disease development.
Keywords: Hypothyroidism, Cardiovascular disease, Euthyroid, Subclinical, Dyslipidemia
Full Text:
INTRODUCTION
Worldwide, thyroid gland disorders are most abundant public health problems.1 From total national burden of endocrine disorders, magnitude of thyroid gland disorders constitute approximately 42 millions in India.2 Thyroid disorders results from either hyper or hypo secretion of tri-iodothyronine (T3) and thyroxine (T4) from thyroid gland. Subclinical hypothyroidism (SCH) is defined as an elevated serum thyroid stimulating hormone (TSH) associated with normal serum concentration of thyroid hormone (total or free T4 and T3).3 Patients of SCH are asymptomatic or have minimal symptoms. SCH is more common in elderly people with twice in women than men.4 World-wide prevalence of SCH is about 7.5% to 8.5% in women and 2.8% to 4.4% in men.5 An epidemiological study in eight cities of India shows that prevalence of SCH is 8.73% in females and 7.17% in males.6 It is well known that Thyroid hormones and TSH affects synthesis, fate and mobilization of lipids.7 Several previous studies have shown elevated levels of total cholesterol, triglyceride and LDL-C in SCH patients 8, 9, while some study does not support this findings.10 This shows diversity regarding level of lipid parameters in subclinical hypothyroidism. So, our study was aimed to estimate the levels of lipid parameters in patients with subclinical hypothyroidism of our population and to see their relationship with TSH values.
MATERIALS AND METHODS
The present study was conducted at Biochemistry laboratory, Pacific institute of Medical Sciences, Udaipur. 75 patients of subclinical hypothyroidism and 100 age and sex matched healthy controls were included in the study. Inclusion criteria was patients having serum TSH > 5.0 mIU/L with normal serum T3 and serum T4 level. Patients having diabetes mellitus, renal impairment, alcohol addiction, taking treatment for thyroid dysfunction, psychotic disorders or lipid abnormalities, female patients taking oral contraceptive pills and body mass index > 30 kg/m2 were excluded from the study. Present study was approved by human ethical committee of Pacific Institute of Medical Sciences, Udaipur. History and informed consent was taken from each participants of the study. Fasting blood samples were collected from the SCH patients and from healthy controls and after centrifuging were analyzed for fasting blood glucose, serum creatinine, lipid profile (Total cholesterol, Triglyceride, High density lipoprotein) and thyroid profile (serum TSH, serum T3 and serum T4). Thyroid profile was estimated by using Cobas e 411 analyzer. Rest of the parameters were analyzed by using Cobas C 111 analyzer. Quality controls were done before analyzing all the parameters. Methods of estimating parameters: Total cholesterol: CHOD-POD enzymatic method, Triglyceride: GPO-POD enzymatic method, HDL: Homogeneous enzymatic method, Thyroid profile (TSH, T3 and T4): Electrochemiluminescence immunoassay (ECLIA) method. LDL and VLDL were calculated using the Friedewald’s formula.
STATISTICAL METHODS
Stastical analysis was performed using Graph pad Prism 5.0. Data were presented as mean ± SD (standard deviation). Unpaired t test was applied to compare the results between euthyroid and SCH patients and of male and female results of patients and controls. One way analysis of variance (ANNOVA) was applied to the result data of different group of patients. Correlation of TSH with lipid parameters was done by Pearson correlation coefficient. Results of the study were discussed at 95% confidence interval; Interpretation of the test results was done according to p value (p < 0.05 – significant, p < 0.001 – highly significant and p ≥ 0.05 – not significant).
RESULTS
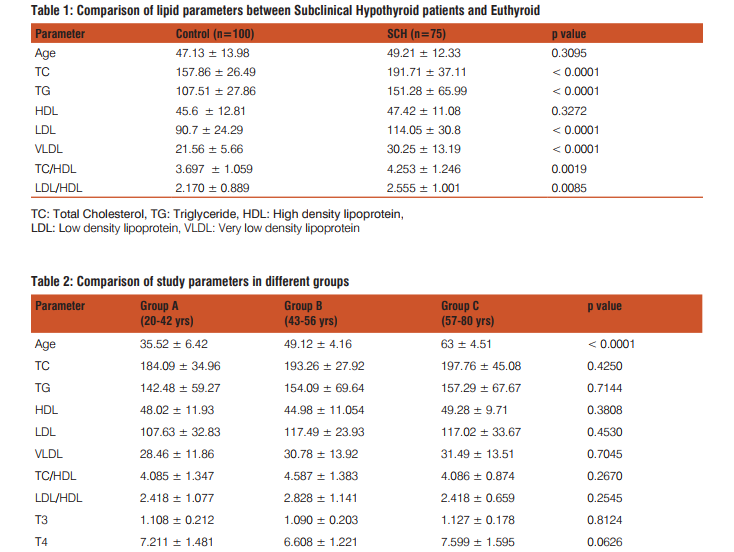
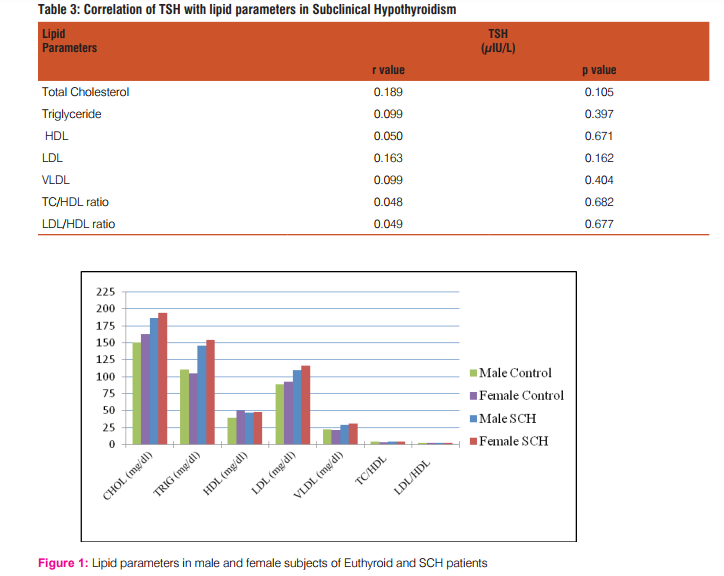
Present study includes 100 healthy controls and 75 subclinical hypothyroidism patients. Control subjects include 59% females and 41% males, while SCH patients comprise 65.3% females and 36.7% males. Mean age of SCH patients was 49.21 ± 12.33 years while that of euthyroid was 47.13 ± 13.98 years (p = 0.3095). TSH level was significantly higher in SCH patients (7.449 ± 2.57 μIU/ml) as compared to Euthyroid subjects (2.581 ± 0.95 μIU/ml, p < 0.0001). Level of serum T4 was decrease in SCH patients (7.139 ± 1.49 μg/ dl) as compared to controls (8.104 ± 1.32μg/dl, p < 0.0001), but was within normal reference limits. SCH patients shows decrease in level of T3 (1.108 ± 0.19 ng/ml) as compared to controls (1.218 ± 0.24 ng/ml, p=0.0016), but was within normal reference range. Mean value of serum Total Cholesterol, Triglyceride, LDL and VLDL were significantly higher in SCH patients as compared to control subjects (p < 0.0001). Mean of TC/HDL and LDL/HDL ratio shows significant difference, while mean value of HDL does not show significant difference between SCH patients and control subjects (Table -1). SCH patients were randomly divided into three age groups: Group-1 (Age 20-42 years), Group-2 (Age 43-56 years) and Group-3 (Age 57-80 years). Values of lipid parameters among these groups were compared by one way analysis of variance (Table-2). All lipid parameters were correlated with TSH values in SCH patients by using Pearson correlation coefficient. Among all lipid parameters, Total cholesterol (r=0.189) show highest positive correlation with TSH values (Table-3). We have also compared the results of lipid parameters and thyroid hormone between male and female of SCH and control subjects. Male and female subjects of euthyroid show significant difference in values of total cholesterol (p=0.0161), HDL (p< 0.0001), TC/HDL (0.0060) and LDL/ HDL (0.0196). Mean value of lipid parameters were higher in female as compared to males of SCH patients, but were not statistically significant (Figure-1).
DISCUSSION
Subclinical hypothyroidism is a laboratory diagnostic condition, which is detected by Serum TSH measurement. Hallowell et al. showed that SCH usually occurs in 40-60 years of age range.11 In our study mean age of the SCH patients was 49.21 years. In present study SCH patients comprises 65.3% women and 36.7% men, which shows that SCH is more common in women that in men. Thyroid hormone plays significant role in cholesterol synthesis and uptake, lipoprotein metabolism and lipolysis by inducing the expressions of different enzymes.12-16 Alteration in level of lipid parameters in SCH patients is unclear. The present study shows that levels of all lipid parameters were significantly increased in SCH patients as compared to the euthyroid subjects, except increase in HDL was not statistically significant. Similar findings were observed by various studies: Adriana Santi et al. concluded that the levels of TC, LDLC and TC/HDL ratio were significantly increase in the subjects with subclinical hypothyroidism than euthyroid.17 In a study conducted by Laway BA et al. found that levels of TC, TG and VLDL were significantly higher in SCH patients as compared to euthyroid subjects.8 Study conducted by Michalopoulou18 showed increase in average level of serum HDL in subclinical hypothyroidism. There is an evidence of increased risk for atherosclerosis and myocardial infarction in elderly female SCH patients.19 The possible explanation of our results are: Decreased thyroid function results in reduction in cell surface receptor for LDL20 and decrease in their activity (abbas et al., 2008) leads to decreased LDL and IDL catabolism; these increases TC and LDL concentration. Decreased activity of hepatic lipase results in increase level of TG rich lipoproteins; these causes high VLDL and TG concentration.21 Tan et al. (1998) showed altered metabolism of HDL in thyroid dysfunction. Our study shows that TSH is positively correlated with values of all the lipid parameters estimated in SCH patients, though it is not good correlation. A Regmi et al.22 showed that values of TC, HDL and LDL, while Shashi A et al.23 found that values of TC, TG and LDL were positively correlated with TSH values in Subclinical hypothyroidism. A study conducted by Ali M. Nouh et al. in a Murzok, Libya Population found that TSH was positively correlated with lipid profile values in subjects with thyroid dysfunction.24
CONCLUSION
From the present study, it is concluded that subclinical hypothyroidism shows secondary dyslipidemia which is associated with increase in levels of total cholesterol, triglyceride, LDL, VLDL, TC/HDL and LDL/HDL ratio. Although good cholesterol (HDL) level increase in SCH, it is not significant. These increases risk of atherosclerosis and cardiovascular disease development. So, all dyslipidemic patients, particularly women with 40-60 years of age should be tested for thyroid dysfunction and accordingly be treated. This may help to reduce mortality and morbidity due to atherosclerosis and cardiovascular diseases.
ACKNOWLEDGEMENT
Authors are thankful to all participants of the study and to the technical staff of biochemistry laboratory of Pacific Institute of Medical Sciences, Udaipur for their help and support during the study. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.

References:
1. Heuck CC, Kallner A, Kanagasabapathy AS and Riesen W. Diagnosis and monitoring of the disease of the thyroid. WHO Document (WHO/DIL/00.4) 2000; 8-9.
2. N. Kochupillai. Clinical endocrinology in India. Current Science. vol.79, no.8, 25 Oct 2000.
3. Mcdermott MT and Ridgway EC. Subclinical hypothyroidism is mild thyroid failure and should be treated. The journal of clinical endocrinology and metabolism 86(10):4585–4590.
4. Tunbridge WMG, Evered DC, Hall R, Appleton D, Brewis M, Clark F, et al. The spectrum of thyroid disease in a community: the Wickham survey. Clin Endocrinol (Oxf). 1977 Dec; 7(6):481-93.
5. Canaris GJ, Manowitz NR, Mayor G and Ridgway EC. The Colorado Thyroid Disease Prevalence Study. Arch Intern Med. 2000; 160:526-534.
6. Unnikrishnan AG, Kalra S, Sahay RK, Bantwal G and John M. Prevalence of hypothyroidism in adults: An epidemiological study in eight cities of India. Indian J Endocrinol Metab. 2013 Jul-Aug; 17(4): 647–652.
7. Pucci E, Chiovato L and Pinchera A. Thyroid and lipid metabolism. INT J OBESITY. 2000; 24:S109–12.
8. Laway BA, War FA, Shah S, Misgar RA and Kotwal SK. Alteration of Lipid Parameters in Patients with Subclinical Hypothyroidism. Int J Endocrinol Metab. 2014 July; 12(3): e17496.
9. Pirich C, Mullner M and Sinzinger H. Prevalence and relevance of thyroid dysfunction in 1922 cholesterol screening participants. J Clin Epidemiol. 2000 Jun; 53(6):623-9.
10. Hueston WJ and Pearson WS. Subclinical Hypothyroidism and the Risk of Hypercholesterolemia. ANNALS OF FAMILY MEDICINE VOL. 2, NO. 4, JULY/AUGUST 2004.
11. Hollowell JG, Staehing NW, Flanders WD, Hannon WH, Gunter EW, Spencer CA et al. Serum TSH, T4, and thyroid antibodies in the United States Population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metabol 2002; 87: 489-99.
12. Simonet WS and Ness GC. Transcriptional and posttranscriptional regulation of rat hepatic 3-hydroxy-3-methylglutaryl-coenzyme A reductase by thyroid hormones. J Biol Chem. 1988; 263: 12448-53.
13. Shin D-J and Osborne TF. Thyroid Hormone Regulation and Cholesterol Metabolism Are Connected through Sterol Regulatory Element-binding Protein-2 (SREBP-2). J Biol Chem. 2003; 278: 34114-8.
14. Saffari B, Ong JM and Kern PA. Regulation of adipose tissue lipoprotein lipase gene expression by thyroid hormone in rats. J Lipid Res. 1992; 33: 241-9.
15. Berti JA, Amaral ME, Boschero AC, Nunes VS, Harada LM, Castilho LN, et al. Thyroid hormone increases plasma cholesteryl ester transfer protein activity and plasma high-density lipoprotein removal rate in transgenic mice. Metabolism. 2001; 50: 530-6.
16. Gagnon A, Antunes TT, Ly T, Pongsuwan P, Gavin C, Lochnan HA, et al. Thyroid-stimulating hormone stimulates lipolysis in adipocytes in culture and raises serum free fatty acid levels in vivo. Metabolism. 2010; 59: 547-53.
17. Santi A, Duarte MMMF, de Menezes CC and Loro VL. Association of Lipids with Oxidative Stress Biomarkers in Subclinical Hypothyroidism. Int J Endocrinol. 2012; 2012: 7p.
18. Michalopoulou G, Alevizaki M, Piperingos G, Mitsibounas D, Mantzos E, Adampoulos P, et al. High serum cholesterol levels in persons with ‘high normal’ TSH levels: should one extendthe definition of subclinical hypothyroidism? Eur J Endocrinol 1998; 138:141-145.
19. Hak AE, Pols HAP, Visser TJ, Drexhage HA, Hoffman A and Witteman JCM. Subclinical hypothyroidism is an independent risk factor for atherosclerosis and myocardial infarction in elderly women: the Rotterdam Study. Annals of Internal Medicine 2000; 132: 270–278.
20. Thompson GR, Soutar AK, Spengel FA, Jadhav A, Gavigan SJP and Myant NB. Defects of receptor mediated low density lipoprotein catabolism in homozygous familial hypercholesterolemia and hypothyroidism. Proc Natl Acad Sci U S A. 1981 Apr; 78(4):2591-5.
21. Brenta G, Berg G, Arias P, Zago V, Schnitman M, Muzzio ML et al. Lipoprotein alterations, hepatic lipase activity, and insulin sensitivity in subclinical hypothyroidism: response to L-T(4) treatment. Thyroid. 2007 May; 17(5):453-60.
22. A Regmi, B Shah, BR Rai and A Pandeya. Serum lipid profile in patients with thyroid disorders in central Nepal. Nepal Med Coll J 2010; 12(4): 253-256.
23. Shashi A and Sharma N. Lipid profile abnormalities in hypothyroidism. I.J.S.N., vol. 3(2) 2012: 354-360.
24. Nouh AM, Eshnaf IAM and Basher MA. Prevalence of Thyroid Dysfunction and Its Effect on Serum Lipid Profiles in a Murzok, Libya Population. Thyroid Science 3(10):CLS1-6, 2008.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





