IJCRR - 14(2), January, 2022
Pages: 60-67
Date of Publication: 16-Jan-2022
Print Article
Download XML Download PDF
Health Problems of Low Skilled Indian Male Migrants Living in Gulf Countries: A Cross-sectional Study
Author: Mohammed Rafiuddin, Kosalram Kalpana
Category: Healthcare
Abstract:Introduction: Due to an increase in migrant's movement, health has become a key issue. Moving across different ecological conditions may expose migrants to new diseases and promote disease transmission. Aims: The present study aimed to determine among low-skilled male migrants health problems and their access to health services in gulf countries. Methodology: This cross-sectional study involved only male migrants from six countries. The study took place at Warangal district, Telangana, India. The survey questionnaire was interviewed. The questionnaire consisted of items pertaining to general health, illness, treatment and diseases including access to health care services in the host countries. Data were analyzed using frequencies, percentages and the chi-square test was used for comparison. Results: A total of 410 participated with a response rate of 82.32%. The majority of sampled respondents were from Saudi Arabia 183(44.63%) and UAE 101(24.63%). The greater number of respondents were employed as construction labour (25.4%), re-tail salesperson (10.2%) and driver (10.5%). The health problem frequently occurring reported are headaches (62.0%), difficulty concentrating (50%), stomach or digestive problems (58.5%) pain or a tight feeling in the chest (42.4%), irritated eyes (57.6%) and dry skin (50.5%). High blood pressure (41%), Cardiovascular diseases (33%), Insomnia (35%), Muscular or joint problems (53%) and Neck problem (60%) are the major illness are ailments reported. Hypertension (196), metabolic arthritis (159), cardiovascular (133) and diabetes (114) are the sufferings of the current disease. The majority of the participants reported having access to health care (77%) in their respective countries of employment provided by the employer. The biggest obstacles are no transportation availability, travelling issues, no time, language problem and lack of finance to access the healthcare services. Conclusions: The findings showed that a substantial portion of health problems were attributed to prolonged working conditions among low-skilled migrants. It emphasizes implementing various strategies or policies to protect the health and well-being and improve their access to essential health services to all types of migrant workers in the host countries government and Indian government by tracking them.
Keywords: Gulf countries, Health problems, Healthcare, Low skilled workers, treatment and Migrants.
Full Text:
Introduction
Nearly, 8.5 million Indian migrants are present and working under various employment categories in the gulf nations. Thus, it has the largest population of migrants in the world.1 Due to the rejection of jobs by local workers, low skilled workers work under risk-prone jobs that lead to serious health problems among Indians. Further, these migrants are forced to work under (3Ds) dangerous, dirty and degrading jobs.2 Due to an increasing number of people moving from one country to another, migrant’s health has become a key global public health issue.
At present not only the US, UK, Canada and the Gulf, but also a larger number of countries like members of European Union, Africa and Asia are emerging major destinations for Indians.3 Majority of them go to gulf countries as temporary unskilled or semi-skilled workers and work until the expiry of the contract.4 The state of Kerala is considered as the ‘migration hub’ or central node of the India-Gulf migration corridor.5 These migrants are employed either directly by the employer or through the consulted agency. The study reported that while about two-thirds of the migrant workers were semi-skilled or unskilled and only 14% were employed in professional technical and managerial occupations.6 Due to the restrictive immigration policies in the Gulf countries, most of the Gulf migrants return to India.7 It is documented that the reasons for returning are due to low income, poor work conditions, health problems and factors related to the situation at home.8
Moving across different ecological conditions may expose migrants to new diseases and promote disease transmission. Further, a couple of studies showed that social, cultural and economic factors are influenced among men and women during the migration process in different groups and locations.9, 10 There is evidence that many migrants when arriving to the host country were healthy but that good health can deteriorate over time in the receiving society.11 It is noted that across European countries there is high rate of depression and anxiety among asylum migrants including Indians compared to the national population.12 In another study, migrants showed health symptoms such as back pain, abdominal pain, headaches, dizziness, gynecological infections, depression and anxiety.13 Several studies showed that rates of schizophrenia (Mental Disorder) were higher among migrant’s groups compared to native white population.14 In addition, migrants usually have poor access to healthcare services.15
However, the labour markets in the destination countries often do not provide enough services for the low paid workers, despite accepting long working hours for low pay. It is reported that, most of the migrant workers in dangerous jobs, low skilled and manual work are vulnerable and pose an increasing risk for psychosocial health issues and mental health problems.16 An extensive review of the literature did not yield any result of health problems of Indian migrants in gulf countries. Therefore, the present context of this study is intended to examine the health problems among low skilled Indian migrants working in gulf countries. Further, explore the use of health care services and barriers in the host countries.
Methods
This research design utilized a cross-sectional approach using random sampling procedure and received ethical approval (2965/IEC/2021) from SRM University, Tamil Nadu, India. This study took place in Warangal District, Telangana State, India. The participants of 410 migrants from six countries (Saudi Arabia, United Arab Emirates (UAE), Qatar, Oman, Bahrain and Kuwait). The study only recruited male participants who had at least one year of working experience. The informed consent of the participants was obtained and ages between 20 to 60 were included. Females are excluded because most of them are homeworkers and are not allowed to work.
The data was collected from April to August 2019; Ramzan and Bakrid as most of the migrants returned to India on a vacation to celebrate the festivals with their families. Prior to data collection a list of participants was made by contacting the known person and his relatives or friends who are living gulf countries. These participants were contacted through mobile phones and discussed the current study in detail. Those who were interested were interviewed by the researcher at their residence. The researcher checked the copy of participant’s employment identification card of respective countries and employment status to make sure as per the inclusion criteria. Researchers filled the questionnaires based on the response of the participants. All the questions were interview and no physical examination of the participants were taken.
The validated study questionnaire was designed and modified from the previous literature review.17-19 The questionnaire was adopted in English only. The questionnaire consisted of four main sections. These are demographic; characteristics of general health; illness and treatments and access to healthcare. To measure various outcomes three options never, sometimes and often and dichotomous variables such as yes or no were also used wherever applicable. In addition, few generalized questions were used to know the perspective of the migrants. All parameters were summarized to compute frequencies, means and percentages using SPSS. Chi-square and Fisher’s exact test was performed to estimate the significance among study variables. Pearson's χ2 test was used and differences were considered statistically significant at p < 0.05.
Results
General Results
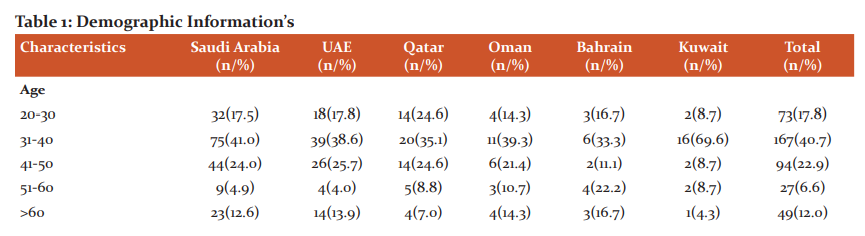
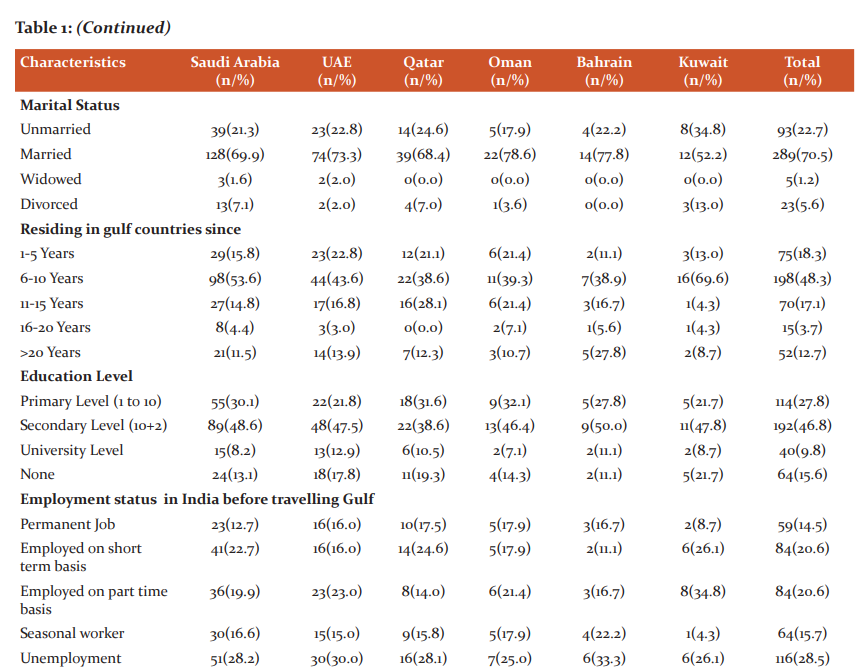
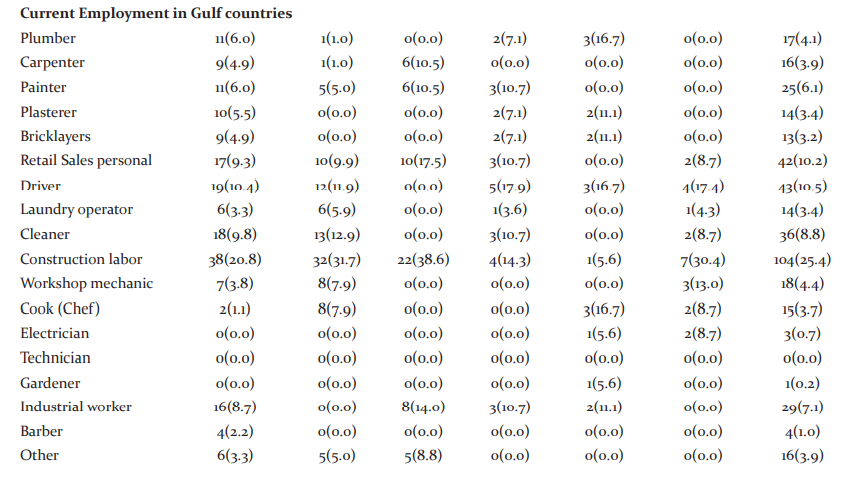
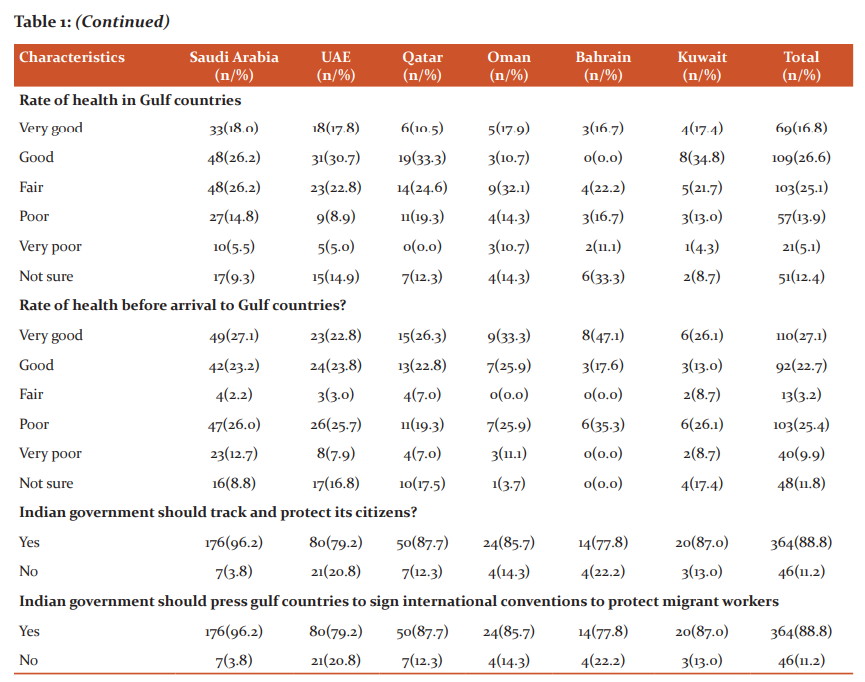
A total of 410 participated, yielding an overall response rate of 82.32%. The majority were from Saudi Arabia 183(44.63%) and UAE 101(24.63). Half of the sampled were educated up to secondary level of education (46.8%). The greater number of respondents were employed as construction labour (25.4%), retail salesperson (10.2%) and driver (10.5%) respectively. It is worth noting that respondents with regards to the status of health were poor (13.9%) in gulf countries compared to 25.4% of poor health before arrival. Interestingly more than one-third of the majority reported that they should be tracked and protected by Indian government and signed international labour conventions in protecting the rights of the workers (Table 1).
Characteristics of general health
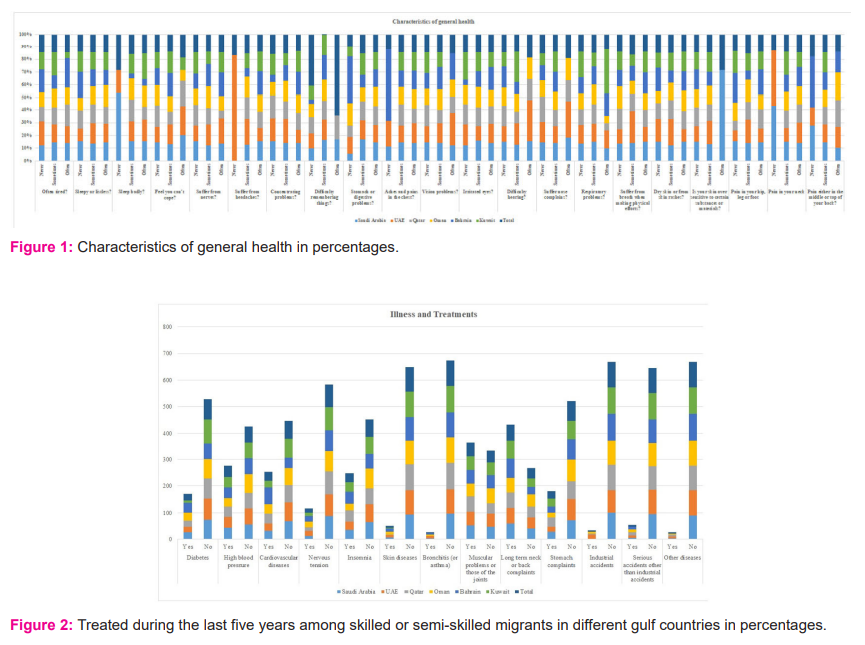
The health problem frequently occurring reported are headaches (62.0%), difficulty concentrating (50%), stomach problems (58.5%) pain or a tight feeling in the chest (42.4%), irritated eyes (57.6%) and dry skin or skin rashes (50.5%) and found slightly significant compared between the countries. Respondents reported often suffering posture movements such as pain in hip, leg or foot (50.0%), neck pain (58.5%) and found it slightly significant. Nevertheless, reported sometimes (88.5%) suffered pain either middle or top of their back (Figure 1).
Illness, treatment and access to health care
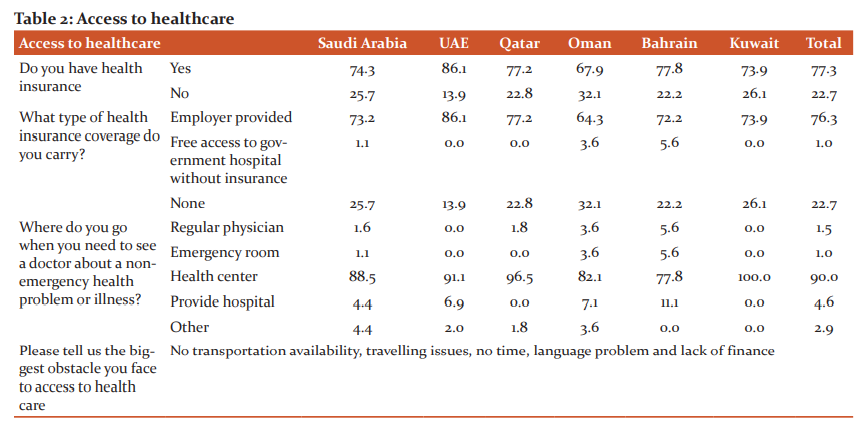
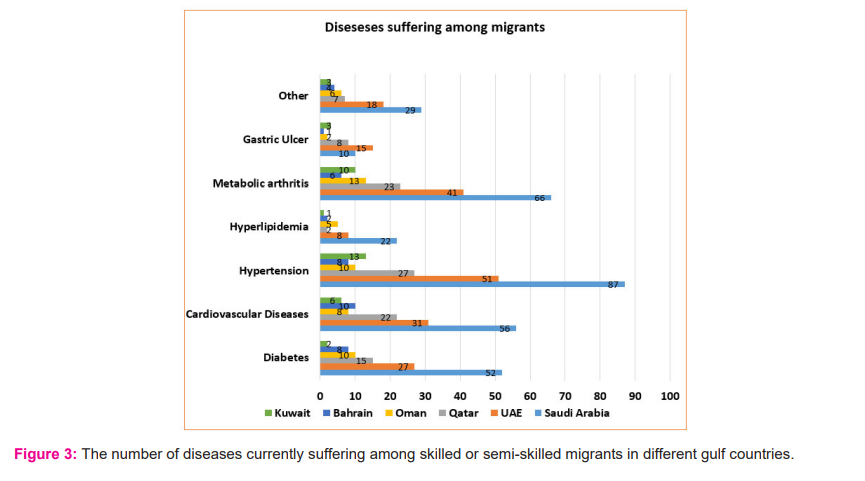
High blood pressure (41%), Cardiovascular diseases (33%), Insomnia (35%), Muscular or joint problems (53%) and Neck problem (60%) are the major illness reported that have been treated during the last five years (Figure 2). The study also reported a lower percentage of industrial accidents and found significance when compared with different countries. Hypertension (196), metabolic arthritis (159), cardiovascular (133) and diabetes (114) are the current diseases reported (Figure 3). Majority of the participants reported having access to health care (77%). To seek medical health, (90%) visit the health center for the treatment of illness. The biggest obstructs are no transportation availability, travelling issues, no time, language problem and lack of finance to access the healthcare services (Table 2).
Discussions
Indian migrants are world’s top recipient of remittances as well largest supplier of international migrants.20 These migrants pose unprecedented health and livelihood challenges for the millions of Indians working in the middle east regions. The study found that half of the migrants completed their secondary education level. This led to a drop in the Emigration Check Required (ECR) to only those job applicants whose educational qualifications are Class 10th failed or uneducated.21 These outcomes indicate that the middle east countries are approaching the migrants of at least secondary or university level of education in the category of unskilled or skilled workers. This study supports previous findings that a close correlation exists between the level of education and job performed by the migrants.22 The study found a greater number of migrants were employed as construction labour, retail sales and drivers. The current study strongly supports the similar findings in which report that 70% of Indian migrants work as the driver, domestic servant or as labor at the construction sites.23 This evidence that Indian workers became the pillars for the development of the construction work in the Gulf countries.
In the current study the status of migrant health was poor in India (25.4%) compared to staying in Gulf countries (13.9%). The reason for the poor condition of health in India could be due to poverty, poor access to health care, unemployment, psychological stress, work-related injuries and communicable and non-communicable diseases. In addition, behavioral risks such as the use of tobacco and alcohol are reported.24,25 The health condition is little improved in gulf countries probably due to availability of health insurances from the employer, advanced health care’s system, personal finance due to employment and environmental factors perhaps influence the health status. One of the most significant findings is that 90% of the migrants reported that they should be tracked and protected by Indian government in protecting the rights of the workers. These results are prompting greater attention needed by the Government of India and the host governments to diaspora affairs and worker welfare issues. The vast majority of migrants are blue collar workers who have paid highly excessive recruitment fees to sell their labor through uncertain existence due to a foreign labor sponsorship system that formalizes their lack of assurance.26 This system known as Kafala system of foreign labor sponsorship, that binds workers to their employers is common widespread in the many gulf countries and has contributed to labor migrants' uncertainty.27 Many of them criticized the system as unfavorable called as "modern-day slavery" or a maze of exploitation by human rights groups due to poor living conditions of the migrant workers.28 These are contributing factors that lead them to need to track the migrants for better living conditions under the convention of labor agreements between the governments. There are evidence that both countries governments are now committed to managing their contract labour arrangements in such a way as to provide mutual benefit, and to avert the risk of exploitative practices at variance with international standards of human and labour rights.29 However, not a single of them has amended the convention which binds itself to this international treaty. The gulf countries have to take the reforms seriously so that they can make a suitable environment for the migrant laborers.
The most common general health issues among them are headache, digestive problems, irritated eyes, skin rashes, concentration difficulties and ailments of the heart (Figure 1). These percentages of health problems reported such as headache and digestive problems among Indian migrants are much higher compared to similar studies reported among Indian subcontinent and Nepalese migrants.19,30 Further, results are consistent with a similar type of health study that reported cardiopulmonary, gastrointestinal (GI), and pseudo neurologic and medical symptoms are higher among migrants in Qatar and found statistically significant.31 Half of the respondents reported often suffering posture movement such as pain in hip, leg or foot and neck pain. High blood pressure, Cardiovascular diseases, Insomnia, Muscular or joint problems and Neck problems are the major illnesses reported (Figure 2). This is clearly evident in the health of the Indian migrant getting through different health crises pertaining to longer employment and longer duration of stay in these gulf countries.19 In contrast, reported a lower percentage of industrial accidents and found significance. This lower percentage is much lower when compared with a similar study where construction workers reported having experienced injuries or accidents at their workplace.19 The explanation for these health reasons that the migrants are neglecting to participate in preventive care or possible delay in treatment process. In addition, low wages, dangerous working conditions, long working hours, poor housing and overcrowded accommodation are detrimental to the quality of life of migrants, which resulted in their health crisis.32 The overall reported diseases currently suffering among migrants are hypertension, metabolic arthritis, cardiovascular, diabetes and the least reported gastric ulcer (Figure 3). These diseases reported are similar as well as higher in the general population and migrants.33,34 Despite the high burden, prevention and management did give any prioritized consideration in the host countries.
The current study reported that 77% of them have access to health care in their respective countries of employment provided by the employer through insurance. This is the element contributing the authors believe the health of the migrants shown in this study are much better when compared to their health in India. The curiosity is that 90% of them visit the health center for the treatment of illness other than regular physicians or hospitals. The authors believe that the extremely low rates of health insurance coverage to health centers instead of hospitals was hindering access to better health care services. Only 23% of them do not have health insurance and reported biggest obstacles are no transportation availability, travelling issues, no time, language problem and lack of finance to access the healthcare services (Table 2). The current study findings support what previous studies found concerning barriers to healthcare.35,36 These barriers lead to consequences of their health and well-being, both in terms of the actual treatment and other possible health-related consequences among migrants.
Limitations
The study was performed in a single district and the results cannot be attributed to the completely migrant population. Although the current study focuses on migrants from different gulf countries, the majority of respondents were from Saudi Arabia. The responders in the current study have nothing to gain or to fear by reporting their health problems. Thus, the authors believe that such interests have not affected our results. Additional studies are needed to observe factors besides those reported in this study. Despite these limitations, the study sheds light on the issues of migrant health to greater extent considering messages for the migration policy makers in India and the hosting government in conjugation to improve the health services.
Conclusions
In conclusion, the present findings demonstrate that the status of health problems were occupying wide space among migrants and reported suffering more than one type of health problem. Despite having the majority of migrants' access to healthcare provided by the employer, still a larger number of them suffer health issues continuingly. It is noted that a substantial portion of health problems were attributed to prolonged working conditions among migrants. It is recommended to provide adequate information for the migrants making them aware of their health risks in the hosted countries. This study emphasizes implementing various strategies or policies to protect health and improve their access to essential health services to all types of migrant workers. Recommends different government agencies must engage with the Ministry of Health to create a migration platform of tracking and adopt different health policies including easy working environments.
Acknowledgment
The authors acknowledge the immense help received from all the gulf migrants who participated in this study. The authors also thank Mr. Elamin kheir for his statistical analysis in the current study.
Conflict of Interest: None
Financial Support: None
Author Contribution: First Author: Developing questionnaire survey, data collection and analysis including manuscript writing. Second Author: Reviewed literature and editing the manuscript.
References:
-
India-Gulf Migration. Available from:https://www.mei.edu/publications/india-gulf-migration-testing-time.[Last accessed on 2021 June 15]
-
Benach J, Muntaner C, Chung H, Benavides FG. Immigration, employment relations, and health: developing a research agenda. Am J Ind Med.2010;53:338–43
-
Khadria B. Skilled labour migration from developing countries: study of India. Geneva: International Labour Office; 2002 (International Migration Papers, No. 49)
-
Irudaya RS, Kumar P. 2010. Historical overview of international migration. In Governance and Labour Migration. India Migration Report 2010, Irudaya RS (ed.). Routledge: London, New York and New Delhi;1–29
-
Czaika, M. Internal versus international migration and the role of multiple deprivations: some evidence from India. Asian Population Studies, Asian Population Studies.2012; 8(2),125-149
-
Eevit Z, Zachariah KC. (1978). International labour migration. Finance and Development. 1978;15(4)
-
Shah, Nasra, “Recent Immigration Policies in the Oil-Rich Gulf: How Effective are they likely to be?” ILO Asian Regional Programme on Governance of Labor Migration, WP No. 3, 2008
-
Czaika M, Varela M. V. Labour market activity, occupational change and length of stay in the gulf. Migration Studies.2014;3,315-342
-
Castelli F. Drivers of migration: why do people move? J Travel Med 2018;25(1)
-
Bhugra D, Becker MA. Migration, cultural bereavement and cultural identity. World Psychiatry.2005;4(1):18-24
-
Spencer (ed) S, Johnson MRD, Phillips D, Rudiger A, Somerville W, Wintour P, Refugees and other new migrants: a review of the evidence on successful approaches to integration,(2004)iii-39
-
Raphaely N: Understanding the health needs of migrants in the South East Region. London: Health Protection Agency and Department of Health,2010
-
Zimmerman C, Hossain M, Yun K., The health of trafficked women: a survey of women entering post trafficking services in Europe. Am J Public Health. 2008;98(1):55–59
-
Bhugra D, Jones P. Migration and mental health. Advances in Psychiatric Treatment.2001;7:216–222
-
Mou J, Cheng J, Zhang D, Jiang H, Lin L, Griffiths SM: Health care Utilisation amongst Shenzhen migrant workers: Does being insured make a difference? BMC Health Service Research 2009,9:241
-
Mucci N, Traversini V, Giorgi G, Tommasi E, De Sio S, Arcangeli G. Migrant workers and psychological health: a systematic review. Sustainability. 2019;12(1):120
-
Mehlum IS, Kjuus H, Veiersted KB, Wergeland E. Self-reported work-related health problems from the Oslo Health Study. Occup Med (Lond) 2006;56:371–379
-
de Castro AB, Gee GC, Takeuchi DT. Job-related stress and chronic health conditions among Filipino immigrants. J Immigr Minor Health.2008;10(6):551–558
-
Joshi S, Simkhada P, Prescott GJ: Health problems of Nepalese migrants working in three Gulf countries. Bmc Int Health Hum R. 2011,11:3-10.1186/1472-698X-11-3
-
World Bank, “Migration and Remittances Recent Developments and Outlook; 2019. Available from:https://www.knomad.org/sites/default/files/2019-04/Migration and Development Brief_31_0.pdf.[Last accessed on 2021 June 19]
-
Arabian Business. Indian workers migrating to Gulf region dropped 21% in 2018. Available from:https://www.arabianbusiness.com/politics-economics/411281-indian-workers-migrating-to-gulf-region-dropped-21-in-2018.[Last accessed on 2021 June 20]
-
ILO 2012 Global estimate of forced labour Executive summary. Available from:https://www.ilo.org/wcmsp5/groups/public/---ed_norm/---declaration/documents/publication/wcms_181953.pdf.[Last accessed on 2021 June 22].
-
The plight of Indian migrant workers in Gulf countries; 2020. Available from:https://blog.ipleaders.in/plight-indian-migrant-workers-gulf-countries/.[Last accessed on 2021 June 22]
-
Kusuma YS, Babu BV. Migration and health: a systematic review on health and health care of internal migrants in India. Int J Health Plann Manag.2018;33(4):775–93
-
Rafiuddin M, Kalpana K. Psychosocial Workplace Factors and Health Problems among Indian Migrants in Gulf Cooperation Council Countries.Indian J Public Health Res Dev. 2022;13(1)290-300
-
Kamat A, “The Men in the Middle,” Dissent 62,2(2015):65-72
-
Diop A, Johnston T, Le KT. Migration policies across the GCC: Challenges in reforming the Kafala. In P. Fargues and N. Shah (Eds.), Migration to the Gulf: Policies in Sending and Receiving Countries.2018;(pp. 33–60.
-
Unpaid and abandoned: the abuse of Mercury MENA workers. Available from:https://www.amnesty.org/en/latest/research/2018/09/mercury-mena-abuses-qatar/.[Last accessed on 2021 June 23]
-
Plant, Roger,“Temporary Contract Labour in the Gulf States: Perspectives from Two Countries of Origin”, paper presented at the Gulf Forum on Temporary Contractual Labor, 23–24 January 2008.
-
Beshwari M, Bener A, Ameen A, Al-Mehdi A, Ouda H, Pasha M: Pesticide-related health problems and diseases among farmers in the United Arab Emirates. Int. J. Environ. Health Res..1999,9:213-221
-
Bener A. Health status and working condition of migrant workers: major public health problems. Int J Prev Med.2017;8:68
-
Fargues, Philippe, Shah, Nasra M., Brouwer, Imco. “Working and Living Conditions of Low-Income Migrant Workers in the Hospitality and Construction Sectors in the United Arab Emirates”, Gulf Labour Markets, Migration and Population Programme (2019):1-79
-
Petrie JR, Guzik TJ, Touyz RM.Diabetes, hypertension, and cardiovascular disease: clinical insights and vascular mechanisms. Can J Cardiol 2018;34:575–584
-
Mishra SR, Ghimire S, Joshi C, Gyawali B, Shrestha A, Neupane D, et al. Cardio-metabolic disease risk factors among South Asian labour migrants to the Middle East:a scoping review and policy analysis. Global Health. 2019;15(1):33
-
Asgary R, Segar N. Barriers to health care access among refugee asylum seekers. J Health Care Poor Underserved. 2011;22(2):506–22
-
Chuah FLH, Tan ST, Yeo J, Legido-Quigley H. The health needs and access barriers among refugees and asylum-seekers in Malaysia: a qualitative study. Int J Equity Health. 2018;17:120
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





