IJCRR - 14(1), January, 2022
Pages: 94-97
Date of Publication: 03-Jan-2022
Print Article
Download XML Download PDF
Cadaveric Study of Branches of Facial Artery in the Face
Author: Ramya Pavithran
Category: Healthcare
Abstract:Introduction: The facial artery is the anterior branch of the external carotid artery and forms the major source of nourishment to the face and terminates as the angular artery. The variations in the facial artery is highly useful to surgeons and clinicians in facial reconstructions and evaluating various clinical conditions. Aim: To identify and trace the branches of the facial artery in the face. Settings and Design: It is an observational study. Methods and Material: The present study is a descriptive observational study done by dissection method in 50 cadavers. The facial artery branches were identified and traced from their origin to the termination. Care was taken not to damage the vessels. Variations were documented and analyzed. Statistical Analysis Used: The data obtained were entered in a master chart. All qualitative data obtained were quantified according to the frequencies. Frequencies were calculated as percentages. Results: In 73% of cases all the facial branches were present. The facial artery terminated as the angular artery in 82% of cases, as lateral nasal in 12%, superior labial and alar artery in 3% of cases each. 10% of cases showed the presence of the alar branch and pre masseteric was seen in 18%. Conclusions: Variations in the facial artery are useful to anatomists and surgeons alike. These studies provide information that is welcome in this world of cosmetic surgeries of face.
Keywords: Facial artery; Premasseteric branch; Angular artery; Lateral nasal artery; Alar artery; Labial arteries; Facial reconstruction
Full Text:
Introduction:
The facial artery forms the main arterial supply of the face along with the superficial temporal artery and branches from the ophthalmic arteries. Facial artery arises from the external carotid artery at the level of greater cornu of the hyoid bone within the carotid triangle. It has a tortuous course throughout and passes onto the face at the anteroinferior border of the masseter muscle. The facial artery supplies branches to the skin and muscles of the face. The branches on the face are the pre masseteric branch, the superior and inferior labial arteries and the lateral nasal artery. Beyond the lateral nasal the facial artery terminates as the angular artery.1 The facial artery may be rudimentary or hypoplastic. It can terminate as the submental artery (not reaching the face), as labial arteries or as nasal arteries. In its absence, it can be replaced by either the nasal branch of the ophthalmic artery at the medial side of the orbit, the transverse facial, or the maxillary artery. The buccal, posterior alveolar, or infraorbital artery can also be larger than usual, compensating for a deficiency of the facial artery.2
The facial artery pulsations can be felt on the base of the mandible at the anteroinferior angle of the masseter. The anaesthetists feel the facial artery pulsations for monitoring the patients during surgeries(facial artery is also known as the Anaesthetist’s artery). The branches of the facial artery anastomose with each other and with other arteries of the face. The deep wounds and incisions involving the face will bleed profusely. The facial wounds will usually heal quickly and rarely necrose. The anatomical knowledge of the facial artery and its branches become important in cosmetic and reconstructive surgeries. FAMM flap (Facial artery myomucosal flap) is an effective means for reconstructing defects in and around the oral cavity. The FAMM flap was first used by Pribaz.3 Francis Henry et al.4, Hui Ling Chia et al.5, Dupoireux et al.6, Tereck Ayad et al.7 have studied the use of the FAMM flap. The Abbe flap used for the reconstruction of the lips, cleft lip, philtrum and palate also depend on the anatomy of the facial artery. Koshy John C et al.8 and Theodore T Nyame et al.9 have conducted recent studies on the same. The masseter muscle is often exploited to correct facial palsies, benign masseteric hypertrophy, neurectomy induced atrophy of muscle traumatic or non-traumatic upper and lower lip defect repairs and also in other maxillofacial surgeries. If the pre masseteric branch is not taken care of, it can lead to profuse bleeding during the procedure.10
Proper anatomical knowledge of the facial artery and its variations would help the clinicians and surgeons alike.
Materials and Methods:
The present study was done on 100 hemi-facies from 50 properly embalmed and formalin fixed cadavers in the Department of Anatomy, Government Medical College, Kozhikode used for the undergraduate teaching of MBBS and BDS students as a part of the thesis work on the variations of the facial artery. The study protocol was approved by the Institutional Ethics Committee. The facial artery was identified and traced from its origin to the termination. Care was taken not to damage the vessels. Mutilated bodies were excluded from the study.
Results:
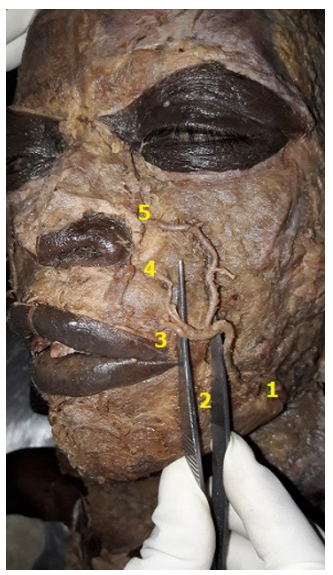
In 73% of the specimen the facial artery showed the presence of all branches in the face, in 27% the artery lacked one or the other branch. Angular artery was absent in 7 specimen (14%), of which 6 specimen showed bilateral absence of the angular artery. Out of the 50 cadavers dissected, lateral nasal artery was not seen in 13 cadavers (26%). In 4 cases, there was bilateral absence of the lateral nasal artery, in 6 cases it was absent on the right and in 3 on the left. The absence of the inferior labial artery was seen in 1 case on the right side. Unilateral absence of the superior labial was seen in 4%, one on right and left side each. Pre masseteric branch was noted in 18% (figure 1), 2 cases showed bilateral pre masseteric branch, unilateral right and left pre masseteric were noted in 5 and 2 cases respectively. The presence of the alar artery directly from the facial artery was seen in 10%. Bilateral alar artery was seen in 2 cases, unilateral right side was seen in 3 cases. Left-sided alar branch from facial artery was noted found in the present study. Sometimes one or the other branch of the facial artery may arise as a common trunk and then divide to form separate arteries. In one of the specimen (1%), the left facial artery gave a common trunk for the labial arteries near the angle of the mouth (figure 2). This common trunk then bifurcated into the superior and the inferior labial arteries, which coursed upper and lower lip areas respectively. In another case, the superior labial and the lateral nasal originated as a common trunk from the facial artery on the left side(figure 3). The facial artery then continued as the angular artery.
Discussion:
In the study by Midy et al.11, facial artery gave angular artery in 27.5%, superior labial in 40% and nasal type in 30%. In 2.5% abortive type was seen. In the study by Niranjan NS12, facial artery terminated as angular artery in 68%, lateral nasal artery in 26%, superior labial artery in 4%. In 2% cases artery terminated at the alar base. Koh KS et al.13 noted 44% lateral nasal and 36.3% angular artery. YA Pinar et al.14 noted that facial artery terminated as angular artery in 22%, as nasal facial in 60%, alar in 12%, superior labial in 4%. Hypoplastic type was seen in 2%. Orhan Magden et al.15 noted that the pre masseteric artery originated as a separate trunk in 14 cadavers studied. Bayram et al.16 classified facial artery into 3 types based on termination. They noted Type I (Facial artery terminated as angular artery) in 76%, type II(facial artery terminated as superior labial) in 12% and type III(Facial artery terminated as inferior labial) in 12%. Ashish S Kulkarni and Geetha KN17 noted that the facial artery terminated as the angular artery in 36%, lateral nasal in 44% and superior labial artery in 20%. In 95% they noted the presence of the pre masseteric artery.
According to George Dickson et al.18, the facial artery had been grouped into 6 types based on termination, as
Type I: facial artery terminating as the superior labial artery
Type II: facial artery terminating as the inferior labial artery
Type III: facial artery terminating as the lateral nasal artery
Type IV: facial artery terminating as the superior alar artery
Type V: facial artery terminating as the inferior alar artery
Type VI: facial artery terminating as the angular artery
Angular artery was seen in 27.5%, lateral nasal in 15%, superior labial in 27.5%, inferior labial in 15% and alar type 15%.
Facial artery terminated as the angular artery in 56%, lateral nasal in 12%, superior labial in 12% and was abortive in 2% in the study by Vasudha et al.19. The premasseteric branch was found in 6% of cases. The percentage of occurrence of various branches of the Facial artery with that of previous studies have been compared in table 1.
Conclusion:
The facial artery forms the major arterial supply of the face. Proper anatomical knowledge of the facial artery and its variations would help the clinicians to diagnose various pathological conditions and also avoid various complications during the procedures. The knowledge of the branching pattern of the facial artery becomes important in various flap surgeries and other procedures of the face, parotid region etc. It also has importance in face lift procedures, dermal filler injections etc. which are cosmetically challenging.
Acknowledgement:
“Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.”
Source of funding: Nil
Conflict of Interest: Nil
Authors’ Contribution:
Dr Ramya Pavithran- Collection of data, compilation and presentation.
IEC Letter No: GMCKKD/ RP 2016/EC/215
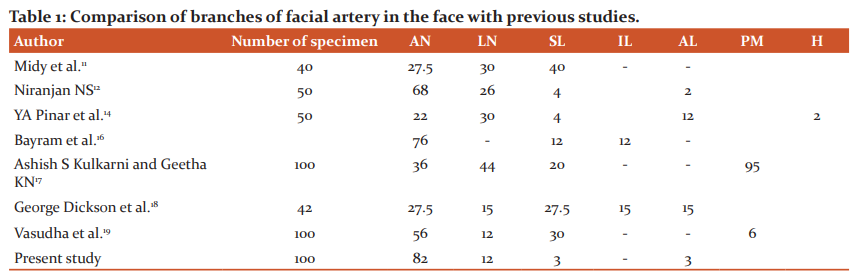

Figure 1: Right side of the face showing the pre masseteric branch of the facial artery
FA- facial artery, PM- pre masseteric branch, TFV- transverse facial vessels

FA- facial artery, PM- pre masseteric branch, TFV- transverse facial vessels
Figure2: Left facial artery with a common trunk for the labial branches.
FV- facial vein, FA- facial artery, IL- inferior labial artery, SL- superior labial artery
Figure 3: Left facial artery with a common trunk for the superior labial and the lateral nasal
List of abbreviations:
FAMM- Facial artery myomucosal flap
AN- Angular artery
LN- Lateral nasal
SL- Superior labial
IL- Inferior labial
AL- Alar artery
PM- Premasseteric branch
H- Hypoplastic
References:
1. Standring S. Gray’s anatomy: the anatomical basis of clinical practice. 2016.
2. Bergman RA, Thompson SA, Afifi AK, Saadeh FA. Compendium of Human Anatomic Variation: Catalog. Atlas World Lit. 1988;86.
3. Pribaz J, Stephens W, Crespo L, Gifford G. A new intraoral flap: facial artery musculomucosal (FAMM) flap. Plast Reconstr Surg. 1992 Sep;90(3):421–9.
4. Henry FP, Leckenby JI, Butler DP, Grobbelaar AO. An algorithm to guide recipient vessel selection in cases of free functional muscle transfer for facial reanimation. Arch Plast Surg. 2014 Nov;41(6):716–21.
5. Chia H-L, Wong C-H, Tan B-K, Tan K-C, Ong Y-S. An algorithm for recipient vessel selection in microsurgical head and neck reconstruction. J Reconstr Microsurg. 2011 Jan;27(1):47–56.
6. Dupoirieux L, Plane L, Gard C, Penneau M. Anatomical basis and results of the facial artery musculomucosal flap for oral reconstruction. Br J Oral Maxillofac Surg. 1999 Feb;37(1):25–8.
7. Ayad T, Kolb F, De Monés E, Mamelle G, Temam S. Reconstruction of floor of mouth defects by the facial artery musculomucosal flap following cancer ablation. Head Neck. 2008 Apr;30(4):437–45.
8. Koshy JC, Ellsworth WA, Sharabi SE, Hatef DA, Hollier LH, Stal S. Bilateral cleft lip revisions: the Abbe flap. Plast Reconstr Surg. 2010 Jul;126(1):221–7.
9. Nyame TT, Pathak A, Talbot SG. The abbe flap for upper lip reconstruction. Eplasty. 2014;14:ic30.
10. Kumar N, Nayak SB, Shetty S, Guru A. Unusual posterior (premasseteric) branch of facial artery–a case report. IJAV. 2011;4:161–3.
11. Midy D. A contribution to the study of the facial artery, its branches and anastomoses. Application to the anatomic vascular bases of facial flaps. Surg Radiol Anat. 1986;8(2):99–107.
12. Niranjan NS. An anatomical study of the facial artery. Ann Plast Surg. 1988 Jul;21(1):14–22.
13. Koh KS, Kim HJ, Oh CS, Chung IH. Branching patterns and symmetry of the course of the facial artery in Koreans. Int J Oral Maxillofac Surg. 2003 Aug; 32(4):414–8.
14. Pinar YA, Bilge O, Govsa F. Anatomic study of the blood supply of perioral region. Clin Anat N Y N. 2005 Jul;18(5):330–9.
15. Ma?den O, Göçmen-Mas N, Senan S, Edizer M, Karaçayli U, Karabekir HS. The pre masseteric branch of facial artery: its importance for craniofacial surgery. Turk Neurosurg. 2009 Jan;19(1):45–50.
16. Bayram SB, Kalaycioglu A. Branching patterns of facial artery in fetuses. NJ Med. 2010;27:227–30.
17. K.N G, Kulkarni A. Variations in Branching Pattern of Facial Artery: An Anatomical Study in 50 Indian Adult Cadavers. 2011.
18. Dickson G, Clark SK, George D, Mackenzie F, Mann NA, Wright K, et al. The variability of the facial artery in its branching pattern and termination point and its relevance in craniofacial surgery. Eur J Plast Surg. 2014 Jan;37(1):1–8.
19. Vasudha TK, DivyashanthiD’Sa, Gowda S. A STUDY ON COURSE AND VARIATIONS OF FACIAL ARTERY ON THE FACE. Int J Anat Res. 2018 Feb 5;6(1.2):4928
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





