IJCRR - 14(1), January, 2022
Pages: 87-93
Date of Publication: 03-Jan-2022
Print Article
Download XML Download PDF
A Study to Find the Effect of Short-Wave Diathermy, Cervical Traction and Mobilization on Pain and Range of Motion in Acute Locking of the Cervical Spine - An Interventional Study
Author: Parmar J, Chhatlani R, Kakkad A
Category: Healthcare
Abstract:Introduction: Acute locking of the cervical spine is a very clearly defined syndrome, occurring most commonly in adolescents. The short-wave diathermy used widely utilise the frequency of 27.12 MHz and wavelength greater than 11m. Cervical traction is a modality of choice for many cervical dysfunctions. It is applicable in a wide range of problems from sprain to fractures and dislocations of the cervical vertebrae. Mobilization is defined as a low-velocity and small- or large-amplitude movement applied anywhere within a joint Range of Motion. Aim: To find the effectiveness of Short-Wave Diathermy (SWD), Cervical Traction (CT) and Mobilization on Pain and range of Motion in Acute Locking of Cervical Spine. Method: 15 male patients with age between 23 to 45 years with the chief complaint of locked neck and difficulty in moving the neck were included in the study. SWD, CT and Mobilization was given to them. VAS and Cervical ROM was assessed before and after the treatment. Result: All Statistical analysis were done by software SPSS 20.0 version. Means and Standard Deviation (SD) were calculated as a measure of central tendency and measure of dispersion respectively. Comparison within group for Visual Analogue Scale (t=30.984), Cervical Flexion (t=-6.671), Cervical Side-Flexion (t=-21.569) and Cervical Rotation (t=-20.601) Range of motion were done by Paired 't' test (p< 0.05). Conclusion: Combination of Short-Wave Diathermy, Cervical Traction and Mobilization is effective in reducing pain and increas�ing range of motion in acute locking of the cervical spine..
Keywords: Short-Wave Diathermy, Cervical Traction, Locking Cervical Spine, Mobilization, Pain, Range of motion, Acute Locking, Visual Analogue Scale
Full Text:
INTRODUCTION:
Acute locking of the cervical spine is a very clearly defined syndrome, occurring most commonly in adolescents.1 It can be described as a condition of sudden onset of ipsilateral neck pain and contra-lateral side flexion of the cervical spine which is primarily caused by abnormal facet joint articulation.2 This syndrome is not to be confused with the locking of joints which can occur as a result of "loose bodies" or torn menisci. The disease has a classic history, preventive deformity and consistent pain. The onset is always sudden and is associated with movement, usually a very quick and often unexpected movement. The result is a sudden, sharp pain accompanied by an inability to return the head to the straight position.1
There are various treatment options available for pain relief including manual and electrical modalities in Physical Therapy. Patients also take various steroid medications for pain relief. 4-10
Short wave Diathermy is a Deep healing modality. Radio waves in the short-wave band have frequencies in the range of 10 MHz-100 MHz. The short-wave diathermy used widely utilize the frequency of 27.12 MHz and wavelength greater than 11m.
There are further 3 methods of applying SWD to the patients:
1. Co-planar: It is also called as the parallel method. The electrodes are placed side by side.
2. Contra-planar. It is also called as through and through the method. Pads are placed on either side of the joints. In this method, deeper tissues are heated.11
3. Crossfire Method: In this technique, half of the treatment is given with the placement of electrodes in one direction, i.e., medial or lateral aspect and another half is used with the placement of electrodes in other direction, i.e., anterior or posterior aspect. This method is commonly used for the treatment of the knee joint, sinuses (frontal, maxillary and ethmoidal) and for pelvic organs.12
Cervical traction is a modality of choice for many cervical dysfunctions. It is applicable in a wide range of problems from a sprain to fractures and dislocations of the cervical vertebrae.
Mainly there are 2 ways in which CT can be given
-
Static traction: Traction for 20-25 minutes is applied with weight ranging from 10 to 30 lbs with a constant pull. It is indicated when pain does not subside with other conservative treatments, especially in radiating neurological pain.
-
Intermittent traction: Traction with alternate phases of stretching (pull) and relaxation is the popular mode of traction. It produces the effects of massage on the muscular, ligamentous and capsular structures. It promotes circulation and reduces swelling, thereby reducing inflammation, spasm and pain.13
Mobilization is defined as a low-velocity and small- or large-amplitude movement applied anywhere within a joint ROM. For an immediate effect, mobilization of the cervical spine had shown a superior effect to reduce pain and increase ROM than mobilization with muscle energy technique or positional release therapy.14,15 The MET was done by asking the patients to repeatedly contract their affected muscles isometrically against the manual resistance by the therapist.14
Outcome Measures:
Neck pain was measured via the VAS. It was a 10-cm line with pain descriptors marked “no pain” at 1 end and “the worst pain imaginable” at the other. The patients were asked to point their perceived pain level with a perpendicular mark on the line, both on most painful activity and at rest. VAS is a reliable and valid measure of pain.16,17
Neck mobility was assessed with a Goniometer. The neck ROM of the patients were measured while high-sitting with feet on the ground, their hips and knees positioned at a 90-degree angle, and their back supported on a chair. Theintratester reliability was reported to be high (ICCs range, .76 –.98).17,18
AIMS AND OBJECTIVES:
AIM:
To find the effectiveness of Short-Wave Diathermy, Cervical Traction and Mobilization on Pain and range of Motion in Acute Locking of Cervical Spine.
OBJECTIVES:
To find the effect of Short-Wave Diathermy on Pain and Range of Motion in Acute Locking of Cervical Spine.
To find the effect of Cervical Traction on Pain and Range of Motion in Acute Locking of Cervical Spine.
To find the effect of Mobilization on Pain and Range of Motion in Acute Locking of Cervical Spine.
HYPOTHESIS:
Experimental Hypothesis:
There is a significant difference in Pain and Range of Motion with the application of Short-wave Diathermy, Cervical Traction and Mobilization in patients with Acute Locking of Cervical Spine.
Null Hypothesis:
There is no significant difference in Pain and Range of Motion with the application of Short-wave Diathermy, Cervical Traction and Mobilization in patients with Acute Locking of Cervical Spine.
MATERIALS AND METHODS:
Study Design: Interventional Study
Study Duration: July 2019 to March 2020
Study Setting: Department of Physiotherapy, Marwadi University, Rajkot, Gujarat, India.
Study Population: Patients with Acute Cervical Lock syndrome
Sampling Design: Purposive Sampling
Sample Size: 15 Male Patients
Inclusion criteria:
-
Age between 23 to 45 years,
-
Chief complaint of locked neck,
-
difficulty in moving the neck at desired direction without pain, and
-
Patients with sudden onset of cervical pain.
Exclusion criteria:
1) Disorders and diseases of the cervical spine such as PIVD, cervical spine stenosis, postoperative diseases of neck and shoulder areas,
2) Torticollis,
3) Any other Cervical Pathology.
The primary physiotherapy screening was done in the OPD. All patients had very similar complaints and signs/symptoms when the assessment was done which is as mentioned here. The diagnosis is made solely on the findings of physical examination and none of the patients were referred for the radiological investigation.
Pain
The patients have pain at the nape of the neck and trapezius muscle of the same side of the neck. All patients were very anxious about the sudden locking of the cervical spine as it would be very difficult to do the Activities of Daily Living (ADL).
Range of Motion
The most commonly seen protective limitation was one of rotation and lateral flexion restriction and sometimes a degree of extension is also limited. Out of all movements at cervical spine rotation was more limited than the lateral flexion and lateral flexion was more limited than the extension. All patients were more concerned about the rotation than the extension of the cervical spine.
METHOD:
Total of 15 patients were taken as per inclusion and exclusion criteria. The procedure and aim of the study were explained to the patients and written consent was taken. Demographic data like Age, onset of the condition, contact details, etc were taken.
SWD for 20 minutes to the trapezius area in supine position. SWD was given in a contra planner manner means one pad was kept on trapezius muscle and the other pad was kept in front of the shoulder. All the necessary precautions were taken before applying short wave diathermy to the patients.
Every patient was given manual cervical traction and checked for the symptoms, if symptoms were increased or gave any discomfort then mechanical cervical traction was not given. If a patient had relief in symptoms then mechanical cervical traction was given to the patients.
If the patient did not have pain and gives comfort to the patient and reduction in pain then the patients were given cervical traction in supine position with 1/7th of the body weight in intermittent mode. At every cycle feedback was taken for any discomfort or pain in the neck. Next day onwards, feedback was not taken while traction was given.
Heat therapy with the hot bag was advised at home for 10 to 15 minutes 2 times in a day.
Next part of the treatment was facilitation of the vertebral rotation while the patient attempts to do the rotation. The patient was in a comfortable sitting position and hands were relaxed on the arms of chair.
The therapist was at backside of the patient. Patients were asked to do the active rotation and when the movement is halted the therapist will help to do the rotation of the cervical vertebra from C4 to C7 and every time patient has to do active rotation maximally. The tip of the right thumb was kept at every level of the cervical spine and pushed to the opposite side of rotation i.e., if the patient was attempting right cervical rotation then the therapist pushed the vertebra towards left side to facilitate the rotation towards right side and vice versa. The gentle oscillatory movement was also performed at each level of cervical spine from C4 to C6 when the active rotation was halted by the patient. The patient was instructed not to do excessive rotation which increased the pain intensively. But at the same time minimal or bearable pain while attempting the movement was allowed.

Thumb kneading was given only for 5 to 7 minutes to the affected trapezius to reduce the spasm. Gentle myofascial release was given from the occiput to the trapezius area with the radial side of the thumb for 5 to 7 minutes to relax the muscle of the same side.
After this, to improve the extension of the cervical spine the position was the same as for rotation. The patient was asked to do the active extension till he can do it without much pain when the active extension was halted due to pain the therapist will be palpating the spinous process of cervical vertebra from C4 to C7 and it was pushed towards the anterior-superiorly with the help of ulnar border of right thumb. Gentle oscillations were also given at each level at the end of active movement which was done by the patient. Oscillations were given for 2 to 3 minutes to the patients.
Patient was advised to do the active movement of the cervical spine at home but in pain free range of motion along with the heat therapy. No other exercises were given at home.
Patient was informed that soreness may occur after some time due to this mobilization and advised not to do anything for that except heat therapy.
RESULT:
All Statistical analysis were done by software SPSS 20.0 version. Means and Standard Deviation (SD) were calculated as a measure of central tendency and measure of dispersion respectively. Comparison within-group for, Cervical Flexion, Cervical Side-Flexion and Cervical Rotation Range of motion were done by Paired ‘t’ test.
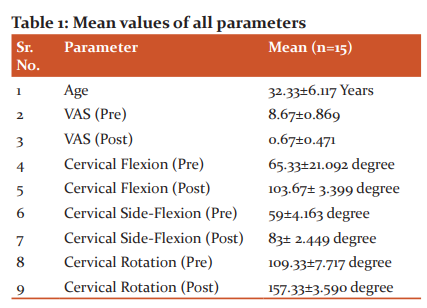

Interpretation: The above table shows the mean difference of pre and post cervical Flexion score i.e., 38.333±22.253 (SD). Result shows significant difference for pre & post Cervical Flexion Range of Motion (t= -6.671).
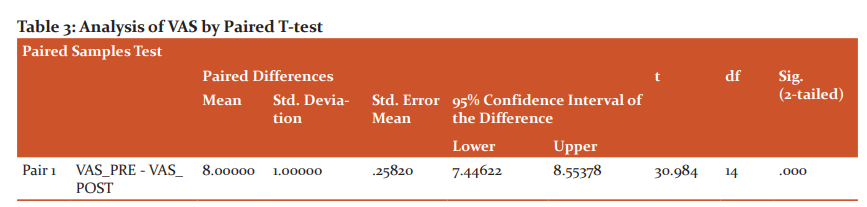
Interpretation: The above table shows the mean difference of pre and post-VAS scores i.e., 8±1 (SD). Result shows significant difference for pre & post VAS score (t= 30.984).
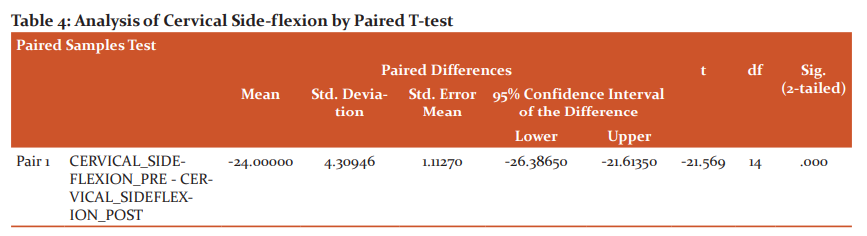
Interpretation: The above table shows the mean difference of pre and post cervical Side-Flexion score i.e., 24±4.309 (SD). Result shows significant difference for pre & post-Cervical Side-Flexion Range of Motion (t= -21.569).
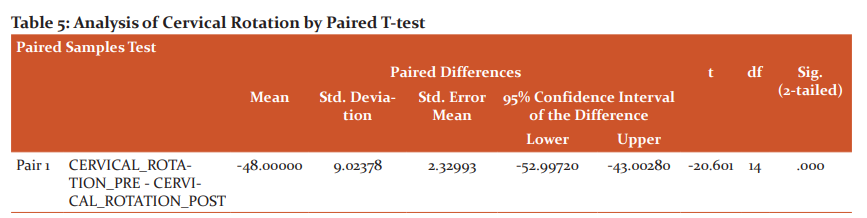
Interpretation: The above table shows the mean difference of pre and post cervical Rotation score i.e., 48±9.023 (SD). Result shows significant difference for pre & post Cervical Rotation Range of Motion (t= -20.601).
DISCUSSION:
From the results it can be commented that significant improvements in terms of pain and increased range of motion at the cervical spine is obtained with the designed protocol.
SWD is considered as a deep heating modality.18 Short-wave diathermy uses an oscillating electromagnetic field of high frequency to heat body surface areas. It heats to a tissue depth of 2 to 3 cm.19 SWD increases temperature of the tissue. SWD effects can be divided mainly into thermal and not thermal. Thermal effects cause vasodilatation, reduction in muscle spasm, elevation of pain threshold, increased soft tissue extensibility, and acceleration of cellular metabolism.21 They include decreased joint pain and stiffness, increased blood flow, faster resolution of oedema, accelerated wound healing, and reduced inflammation.22 Another possible mechanism is activation of A-alpha and A-beta fibres or the cutaneousthermoreceptors which blocks the transmission of pain (A-delta and C fibres) as it enters the spinal cord.23 Diathermy improves cellular healing processes, which produces expression of heat shock proteins (HSP), which causes faster intracellular protein repair and in turn healing process.24,25,26
Cervical traction is commonly used to reduce the spasm at the neck. Cervical traction in a supine lying position gives stretching effects on the neck muscle and gives muscle relaxation which ultimately reduces pain and improved range of motion. Traction was given to only those patients who had improved in symptoms during manual traction. None of the patient had increased pain during or after the cervical traction in supine lying position.27,28
Manual mobilization was given in terms of gentle oscillation, forward glide, rotatory glide which have facilitated the movements in the restricted direction. This had improved the rotation to the affected side along with the forward flexion and extension. Research has shown that mobilization helps initiate local physiological mechanism and also involves central mechanism like facilitation of pain-gait mechanism.29
Limitations:
Small Population size was taken.
Only male patients were taken.
Long term effect of treatment could not be observed due to time constraint.
Further Recommendations:
Study can be conducted with larger sample size.
Male as well as Female patients can be included.
The intervention can be compared to other manual and electrical modalities.
Long term follow-up of patients should be taken.
CONCLUSION:
A combination of Short-Wave Diathermy, Cervical Traction and Mobilization is effective in reducing pain and increasing range of motion in acute locking of the cervical spine.
ACKNOWLEDGEMENT:
Authors acknowledge the immense help received from the scholars whose articles are cited and included in the references of this manuscript. The authors are also grateful to the authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
SOURCE OF FUNDING:
No fund was needed for the study.
CONFLICT OF INTEREST:
There was no personal or institutional conflict of interest for this
AUTHORS’ CONTRIBUTION:
PARMAR J:
Data Collection, Methodology, Research Design, and Framework for the research.
CHHATLANI R:
Referencing, Discussion, and Statistical Analysis
KAKKAD A:
Data Collection, and Cross-referencing
References:
-
Maitland G. ACUTE LOCKING OF THE CERVICAL SPINE1 1Presented at “Conference on Headache, Neck and Arm Pain”, Western Australian Institute of Technology, Australian Physiotherapy Association, 26th November, 1977. Aus J of Physio. 1978;24(3):103-109.
-
Langenfeld A, Humphreys B, de Bie R, Swanenburg J. Effect of manual versus mechanically assisted manipulations of the thoracic spine in neck pain patients: study protocol of a randomized controlled trial. Trials. 2015;16(1).
-
Shanmugam S. Immediate Effects of Paraspinal Dry Needling in Patients with Acute Facet Joint Lock Induced Wry Neck. JOURNAL OF CLINICAL AND DIAGNOSTIC RESEARCH. 2017.
-
McCray R, Patton N. Pain Relief at Trigger Points: A Comparison of Moist Heat and Shortwave Diathermy. Journal of Orthopaedic & Sports Physical Therapy. 1984;5(4):175-178.
-
Binder A. Cervical spondylosis and neck pain. BMJ. 2007;334(7592):527-531.
-
Rawe I. The case for over-the-counter shortwave therapy: safe and effective devices for pain management. Pain Management. 2014;4(1):37-43.
-
Graham N. An ICON Overview on Physical Modalities for Neck Pain and Associated Disorders. The Open Ortho J. 2013;7(1):440-460.
-
Masiero S, Pignataro A, Piran G, Duso M, Mimche P, Ermani M et al. Short-wave diathermy in the clinical management of musculoskeletal disorders: a pilot observational study. Int J of Biometeoro. 2019;64(6):981-988.
-
Braddom’s Rehabilitation Care: A Clinical Handbook. 1st ed. Elsevier; 2017.
-
Graham N, Gross A, Goldsmith C, Group t. MECHANICAL TRACTION FOR MECHANICAL NECK DISORDERS: A SYSTEMATIC REVIEW. J of Rehab Med. 2006;38(3):145-152.
-
Helpline Electrotherapy for Physiotherapists Vivendra Kr. Khokhar, Bharat BharatiPrakashan, 3rd Edition, pg.49-62
-
Textbook of Electrotherapy, Jagmohan Singh, Jaypee Brothers Publication, 2nd Edition, pg.151-162.
-
Essentials of Orthopaedics and Applied Physiotherapy, Jayant Joshi, Elsevier Publication, 3rd Edition, pg.439-442
-
Cassidy JD, Lopes AA, Yong-Hing K. The immediate effect of manipulation versus mobilization on pain and range of motion in the cervical spine: a randomized controlled trial. J Manipulative Physiol Ther 1992;15:570-5. 18. Martinez-Segura R, Fernandez-de-las-Penas C, Ruiz-Sáez M,
-
López-Jiménez C, Rodriguez-Blanco C. Immediate effects on neck pain and active range of motion after a single cervical high-velocity low-amplitude manipulation in subjects presenting with mechanical neck pain: a randomized controlled trial. J Manipulative Physiol Ther 2006;29:511-7.
-
Vernon H, Humphreys BK. Manual therapy for neck pain: an overview of randomized clinical trials and systematic reviews. EurMedicophys 2007;43:91-118. 15. Sarigiovannis P, Hollins B.
-
Effectiveness of manual therapy in the treatment of non-specific neck pain: a review. Phys Ther Rev 2005;10:35-50.
-
Youdas JW, Carey JR, Garrett TR. Reliability of measurements of cervical spine range of motion— comparison of three methods. Phys Ther 1991;71:98-106. 28. Capuano-
-
Pucci D, Rheault W, Aukai J, Bracke M, Day R, Pastrick M. Intratester and intertester reliability of the cervical range of motion device. Arch Phys Med Rehab 1991;72:338-40
-
Masiero S, Pignataro A, Piran G, Duso M, Mimche P, Ermani M et al. Short-wave diathermy in the clinical management of musculoskeletal disorders: a pilot observational study. International Journal of Biometeorology. 2019;64(6):981-988.
-
Laufer Y, Dar G. Effectiveness of thermal and athermal short-wave diathermy for the management of knee osteoarthritis: a systematic review and meta-analysis. Osteoarthritis and Cartilage. 2012;20(9):957-966.
-
Al-Mandeel M, Watson T. The thermal and non-thermal effects of high and low doses of pulsed short wave therapy (PSWT). Physiotherapy Research International. 2010;15(4):199-211.
-
Goats G. Continuous short-wave (radio-frequency) diathermy. British Journal of Sports Medicine. 1989;23(2):123-127.
-
Costantino C, Pogliacomi F, Vaienti E (2005) Cryoultrasound therapy and tendonitis in athletes: a comparative evaluation versus laser CO2 and t.e.ca.r. therapy. Acta Biomed 76:37–41
-
Terauchi R, Takahashi KA, Arai Y et al.(2003) Hsp-70 prevents nitric oxide-induced apoptosis in articular chondrocytes. Arthritis Rheum 48:1562–1568
-
McCarthy CJ, Callaghan MJ, Oldham JA (2006) Pulsed electromagnetic energy treatment offers no clinical benefit in reducing the pain of knee osteoarthritis: a systematic review. BMC Musculoskelet Disord 7:51.
-
Physical Agent Modalities Chueh-Hung Wu, in Braddom's Rehabilitation Care: A Clinical Handbook
-
Physical Medicine Approaches to Pain Management Steven Stanos, Allison Baum, in Current Therapy in Pain, 2009
-
Moss P, Sluka K, Wright A. The initial effects of knee joint mobilization on osteoarthritis hyperalgesia. Man Ther. 2007;12(2):109–18.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





