IJCRR - 7(19), October, 2015
Pages: 16-19
Date of Publication: 10-Oct-2015
Print Article
Download XML Download PDF
SALBUTAMOL NEBULISATION: IS IT A PREDISPOSING FACTOR FOR POSTOPERATIVE ATRIAL FIBRILLATION IN CORONARY ARTERY BYPASS GRAFTING PATIENTS?
Author: Megha Shah, Hetal D. Shah
Category: Healthcare
Abstract:Background: Atrial fibrillation (AF) is one of the known complications of cardiac surgery and represents a major cause of morbidity. However, improvements in surgical and anaesthesia technique and controlling various predisposing factors have not helped to curb the incidence. Therefore, search is going on for various modalities to decrease the incidence. Aim: This retrospective study was conducted to evaluate the risk of AF with nebulised ß2 agonists in postoperative cardiac bypass surgery patients. Methods: In this observational study, data of 100 eligible patients operated for coronary artery bypass grafting (CABG) was collected. Patients were divided in two groups: Group A: Patients who had received postoperative nebulised salbutamol Group B: Patients who had not received postoperative nebulised salbutamol The data was analyzed for onset, duration, severity, treatment, outcome of post operative AF (POAF) and also regarding dose, duration of salbutamol. Results: POAF occurred frequently in patients who had received nebulised salbutamol (p< 0.05). ICU and hospital stay was also prolonged in Group A. However, none of the patients had fatal postoperative complication. Conclusion: Salbutamol nebulisation in post CABG patients could be an additional risk factor for POAF.
Keywords: Atrial fibrillation, ß2 agonists, Post cardiac surgery patients, Salbutamol nebulisation
Full Text:
INTRODUCTION
Atrial fibrillation (AF) is most common type of arrhythmia in post cardiac surgery patients; more common with valvular surgeries. It may cause hemodynamic disturbances and so increase in ICU stay and thus treatment cost. It can also increase stroke and other thromboembolic complications.(1) Post operative atrial fibrillation (POAF) has been associated with higher risk of postoperative congestive heart failure (CHF) and renal insufficiency. (2) Various preoperative factors like past history of AF, concomitant valvular disease and intraoperative factors like duration of surgery, intraoperative arrhythmia may increase risk of AF post surgery.(3,4) Increased catecholamine and ionic imbalance during the postoperative period may be associated with AF.(5) Other factors like pericardial inflammation, hypokalemia, systemic arterial hypertension could also increase risk.(6) However, the exact cause for AF post cardiac surgery is not well established. Hence, the search is on to find out other predisposing factors and preventing measures. A study (7) published in American journal of respiratory critical care medicine has showed an association between major cardiovascular events and ß2 agonists in asthma and chronic obstructive pulmonary disease (COPD) patients. They observed modest increase in risk of myocardial infarction (MI) in those taking ß2 agonists (OR=1.67). (7) Over many years, various cardiovascular adverse events, including MI, heart failure, ventricular ectopy, AF and sudden cardiac death resulting from ß2 agonists use in patients with COPD have accumulated.(8,9,10) However, the risk of AF with ß2 agonist is not confirmed in post coronary artery bypass grafting (CABG) patients. As ß2 agonists are used for excess respiratory secretions after cardiac bypass surgery, our study aimed to examine the risk of AF with nebulised ß2 agonists in post cardiac surgery patients.
MATERIALS AND METHODS
This observational, retrospective study was conducted at a tertiary cardiac care hospital, Gujarat. The study was in accordance with the Helsinki Declaration. Information about patients operated for CABG was obtained from case records and also verified with computer records during one year period. A well-designed case record form was used to collect the data of the recruited patients. Patients with risk for AF like concomitant valvular surgery, left main coronary artery disease , age>70 yrs, preoperative/ intraoperative arrhythmias (including AF) and hypo or hyperkalemia, COPD, Asthma, poor left ventricle (LV) function, recent MI, renal impairment, CHF, hypothyroidism, patients requiring IABP and longer duration of CPB(> 120 mins ) and aortic-cross clamp time were excluded . Also, patients on ß blockers and drugs with arrhythmogenic potential, diuretics, angiotensin converting enzyme (ACE) inhibitors or corticosteroids were excluded. Data of eligible patients were collected. Patients did receive their routine medications till the day prior to surgery except anticoagulants which were stopped three days prior as per institute protocol. All other variables like myocardial protection, closure of pericardium, elective maintenance of potassium and analgesia remained same in both the groups. The patients were given salbutamol or normal saline nebulisation therapy for lung recruitment, to remove excess respiratory secretions every 8 hrly for three days after surgery as per hospital protocol. Based on post CABG nebulisation exposure, data of total 100 patients was collected (equal number of patients taken in both groups):
Group A: Patients had received nebulised salbutamol post CABG (n= 50)
Group B: Patients had received saline nebulisation post CABG (n= 50)
Information about baseline characteristics of patients, CABG (on pump or of pump), occurrence of POAF and use of nebulisation in post-operative period was obtained from case record forms. In POAF patients details regarding onset, duration, treatment, outcome and other complications were also analysed.
Statistics Data analysis was performed using chi square test and student’s t test (Sigma stat 3.5software, trial version).The p <0.05 was considered to be statistically significant.
RESULTS
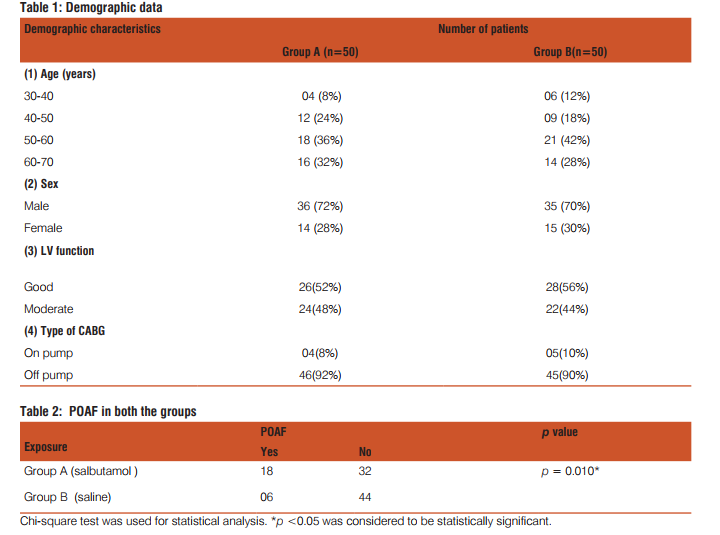
The demographic characteristics of patients are presented in Table-1. All participants were between the 30-70 years. Majority of them were between 50-60 years of age. No difference in gender regarding development of AF was noted. Majority of patients underwent off pump CABG. As shown in table-2, 18 patients in group A while 6 in group B had POAF. AF was common on 2nd and 3rd post operative day. We did not observe any POAF case after discharge from ICU. Average duration for conversion of AF into sinus rhythm was 1 to 1.5 hrs after onset of first episode. Table-3 depicts the incidence of POAF between on pump and off pump CABG cases . Mean length of ICU stay was 5 days in group A while 3 days for group B(5 ± 1.9 vs. 3± 1.3 days; p = 0.163, C.I.-1.080 to 5.080).Hospital stay is also prolonged in group A than group B(10 ± 6.1 vs. 7 ± 3.5 days; p = 0.262 , C.I.-2.481 to 8.481). All POAF patients were treated with inj. amiodarone 5mg/kg i.v. bolus followed by 1 gm/day as i.v. infusion. Oral amiodarone was started to overlap the infusion. Patients were given beta blockers too in postoperative period. The choice was made by cardiologist. Potassium correction was done to maintain range of 4-4.5 mmol/L. However, none of the patients had developed fatal or non fatal complication either due to AF or due to omission of salbutamol. There was no incidence of acute renal failure (ARF), cardiovascular stroke or embolization in any patients.
DISCUSSION
Incidence of POAF varies from 25 - 40 % for cardiac surgery and 50-60% after valvular surgery. (11) The present study revealed that salbutamol nebulisation could be a risk factor for AF in post CABG patients (p<0.02). It usually occurs within 3 days postoperatively but can occur at any point in recovery phase. No difference in incidence was reported between on pump and off pump cases (1), which is in accordance with our study. Use of antiarrythmic drugs, ICU and hospital stay were also increased in salbutamol group as compared to group-B. The competing risks and benefits of ß2 agonist use has been a topic of much discussion. A meta-analysis of 33 randomized placebo-controlled trials of patients with obstructive lung disease revealed that a single dose of ß agonist increased heart rate by 9 beat/min and reduced potassium concentration by 0.4 mmol/L compared with placebo. ß2 agonist treatment for 3 days to 1 year has increased the risk of cardiovascular events more than twofold compared with placebo in trials. (10) Though exact aetiology is not known, multiple factors can predispose to POAF. Hypoxia due to airflow obstruction or due to drug, may precipitate POAF.(12, 13) A study found that despite treatment with ß agonists, airflow obstruction caused hypoxemia and precipitated MI.(7) Observations from various studies evaluating risk of AF proposed various theories. Breeden and colleagues (14) observed risk of arrhythmias with not only systemically administered but also with inhaled selective ß agonists. Myocardial contraction mediated by ß2 receptors present in heart, could be a reason for association of ß2 agonists with tachycardia, an abnormal ECG and atrial fibrillation. (15) A meta-analysis of 3,840 patients undergoing heart surgery found 14% reduction in incidence of POAF between the control group (placebo) and ß receptor blocker group (P<0.00001). (15) Increased plasma levels of ß2 agonists also reported though given by inhalation with low systemic absorption. (16) There are several possible explanations for our finding of risk of POAF in CABG patients. A study by Au DH and colleagues suggested increased rate and force of contraction, decreased peripheral vascular resistance with increased pulse pressure and changes in serum potassium and magnesium levels with ß2 agonists, which may affect conduction pathways in the heart. (7) Stimulation of ß2 receptors can cause intracellular shifts of potassium into skeletal muscle and lead to hypokalemia. Hypokalemia is associated with increased risk of AF, more in pts with COPD or taking diuretics or corticosteroids. (6) Other probable causes include inter individual susceptibility and physical alterations of cardiac structure from incisions on atria. Amiodarone, beta blockers, calcium channel blockers and others like procainamide, methylprednisolone and magnesium have been used for prevention of POAF. Atrial pacing has also gained popularity as non pharmacological preventive measure for POAF. As most of the anti arrhythmic drugs used for prevention have their own side effects, substitution of inhaled salbutamol in high risk CABG patients could be beneficial with other measures. Our study also has certain limitations. The results of study cannot apply to all ß2 agonists as salbutamol was the only ß2 agonist studied based on hospital protocol. Being a retrospective study with small sample size, there are chances of bias due to unrecognized confounding factors. Further randomized controlled trials are required to clarify association of ß2 agonist in POAF. Nevertheless, according to our literature search, this is first type of study evaluating risk of AF with ß2 agonists in post CABG patients. Despite these limitations, we believe that this study should heighten concern over use of salbutamol in patients undergoing cardiac surgery. To help clarify the issue, our study could serve as a landmark for future clinical trials to find out risk of POAF with ß2 agonists.
CONCLUSION
The current study revealed that when other predisposing factors are taken care of, elective omission of salbutamol nebulisation may decrease AF and associated morbidity in post CABG patients. Until proved, the available evidence needs to be examined closely in an attempt to assess whether ß2- agonists should be administered to post cardiac surgery patients.

References:
1. Hashimoto, Hsturp. Influence of clinical and hemodynamic variables on risk of supraventricular tachycardia after CABG. J Thorac Cardiovascular Surg. 1993; 56: 405.
2. Ma JP, Fontes ML, Tudor IC, et al. A multicenter risk index for atrial fibrillation after cardiac surgery. JAMA. 2004; 291:1720- 9.
3. Chidambaram M, Akhtar MJ, Al-Nozha M, Saddique A. A relationship of atrial fibrillation to significant pericardial effusion in valve replacement patients. Thorac Cardiovascular Surg. 1992; 10 :70 -3.
4. Dimpi Patel, Marc A Gillinov, Andrea Natale. Atrial Fibrillation after Cardiac Surgery: Where are we now? Indian Pacing and Electrophysiology Journal. 2008; 8 (4): 281-91.
5. Steve ommen, John A. Odel, Marshall S. Stanton. Atrial arrhythmias after cardiothoracic surgery. NEJM. 1997; 336(20): 1429-34.
6. Salpeter SR, Ormiston TM, Salpeter EE. Cardiovascular effects of beta-agonists in patients with asthma and COPD: a meta-analysis. Chest. 2004; 125: 2309–21.
7. Au DH, Lemaitre RN, Curtis JR, Smith NL, Psaty BM. The risk of myocardial infarction associated with inhaled beta-adrenoceptor agonists. American journal of respire criti care med. 2000;161: 827-30.
8. Cazzola M, Matera MG, Donner CF. Inhaled beta 2-adrenoceptor agonists: cardiovascular safety in patients with obstructive lung disease. Drugs. 2005; 65(12):1595-610.
9. Appleton S, Poole P, Smith B, Veale A, Lasserson T, Chan M.
structive pulmonary disease. Cochrane Database Syst Rev. 2006;3:CD001104.
10. Salpeter SR, Buckley NS, Salpeter EE. Meta-analysis: anticholinergics, but not beta-agonists, reduce severe exacerbations and respiratory mortality in COPD. J Gen Intern Med. 2006; 21:1011-9.
11. Maisel WH, Rawn JD, Stevenson W. Atrial fibrillation after cardiac surgery. Ann Intern Med. 2001;135;1061-73.
12. B J Lipworth .Revisiting interactions between hypoxaemia and ß2 agonists in asthma. Thorax. 2001; 56 :567-9.
13. Carlos A. Viegas, Antoni Ferrer, Josep M. Montserrat, Joan A. Barbera, Josep Roca, Robert Rodriguez-Roisin. Ventilationperfusion response after fenoterol in hypoxemic patients with stable COPD. Lancet. 1990; 336 :1396-99.
14. Breeden C, Safirstein B. Albuterol and spacer induced atrial fibrillation. Chest. 1990; 98:762-3.
15. Crystal E, Connolly S, Sleik K et al. Interventions on prevention of postoperative atrial fibrillation in patients undergoing heart surgery: A meta- analysis. Circulation. 2002; 106:75-80.
16. Anderson PJ, Zhou X, Breen P, Gann L, Logsdon TW, Compadre CM, et al. Pharmacokinetics of (R,S)-Albuterol after aerosol inhalation in healthy adult volunteers. J Pharm Sci. 1998; 87: 841–4.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





