IJCRR - 13(22), November, 2021
Pages: 68-72
Date of Publication: 20-Nov-2021
Print Article
Download XML Download PDF
Effect of Combining Vacuum Massage and Shock Wave Therapy on the Post Burn Scar
Author: Mahmoud Elshazly, Abdelrazak A. Ahmed, Mohammed Ali Sarhan
Category: Healthcare
Abstract:Introduction: Post burns hypertrophic scar is the most serious problem with the burned patient. There are different physical therapy modalities used in the rehabilitation of post-burn scars as pressure therapy, splinting stretching exercises, mechanical massage, and shock wave therapy. Aim: our study was applied to detect the efficacy of combining treatment vacuum massage and shockwave on the post-burn scar. Methods: Forty patients with post-burn scars, age 20-40 years old randomly divided into 2 groups. study group (group A) received manual physical therapy program in addition to combining therapy of shockwave and vacuum massage 3 times per week for 4 weeks, control group (group B) received manual physical therapy program) plus shockwave therapy, 3 times per week for 4 weeks. Results: Skin thickness and VSS decreased significantly in both groups after treatment compared with before treatment but the percent of decreasing of skin thickness and VSS in group A (44.25 and 46.45% respectively) was more than in group B (23.98 and 29.41% respectively). Conclusion: Shock wave treatment has a positive effect on the post-burn scar treatment but the positivity increase if combined with vacuum therapy.
Keywords: Vacuum therapy, Massage, Shock wave, Post-burn scar, Combining therapy, Hypertrophic scar
Full Text:
Introduction
A hypertrophic scar is the most serious functional problem that occurs after burn wounds. 1 Serious of the post-burn scar because it developed within few weeks after burning injury, its serious increase when it develops across a joint axis that is leading to limitation of joint range of motion. 2 The prevalence rate of post scars can be up to 60 % and the scar contracture up to 54 %. 3 Keloid is most serious than scar because it develops and grows beyond the burn wound boundaries. 4 High elastic skin areas (neck, anterior chest, and lower face) are common areas for post-burn scar development. 5 surgical removal of the scar and repair with flap or graft is one from scar treatments but there is a higher per cent for recurrence and tendency of scar formation in donor site of the graft or flap increase (in case of auto-graft). 2
Shockwave therapy is defined as a mechanical sound wave used originally in 1980 in the breakdown of kidney stones. Shockwave therapy causes micro-trauma during the breakdown of extra-collagen fibres in scar tissue and enhances the growth factor release for tissue remoulding and repair. 6 The breakdown effect of shockwave therapy is used in the treatment of calcaneal spurring, muscle fibrosis is also used in the improvement of wound healing and is nowadays used in the treatment of hypertrophic scar. 7
Vacuum massage (depression-massage or vacuum-therapy) is a non-invasive modality characterized by lifting layers of the skin by negative pressure (suction) effect and used to mobilize the skin folds.8 Vacuum massage as manual massage has a significant effect on scar properties but this effect lasts for short time (1-2 hours). 9
So our study was applied to clarify the efficacy of combining treatment vacuum massage and shockwave on the post-burn scar.
Methods & Materials:-
Forty patients with post-burn scars with age 20-40 years old were selected from outpatients clinics of physical therapy faculty, south valley university, Egypt, during the period from June 2020 to February 2021. Patients were randomly distributed into two equal groups, study group (group A) received a manual physiotherapy program (deep friction massage, stretching exercises) in addition to combining therapy of shockwave and vacuum massage 3 times/week for 4 weeks, control group (group B) received manual physiotherapy program (scar tissue mobilization, deep friction massage, pressure therapy, stretching exercises) in addition to shockwave therapy, 3 times/week for 4 weeks. Patients with skin abnormalities, immunodeficiency disorders, mature hypertrophic scars, diabetic patients, spinal cord injuries, peripheral paralysis, and pregnant female were excluded from this study.
Procedures:
Assessment procedures:
-
Ultrasonography:-
By using Toshiba Xario prime ultrasound machine.
-
U.S assessment applies to the higher point of the scar.
-
Then the ultrasonography assessment procedure was applied by the radiology specialist before treatment and after 4 weeks. (probe perpendicular to the skin).
-
The radiological specialist was the same person who applies the assessment each time
-
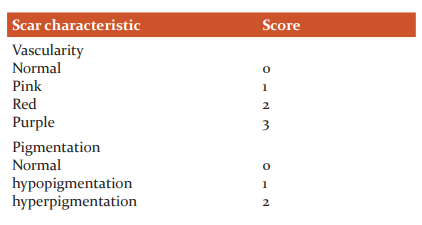
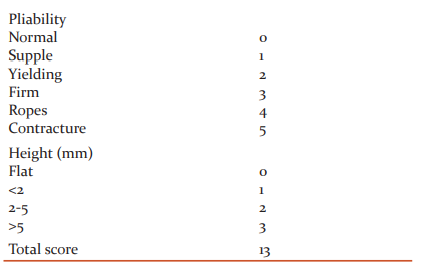
Vancouver scale:-
It was used to assess the scar tissue with parts (vascularity, pigmentation, pliability, and height) before and after 4 weeks of treatment and scored as follow:- 10,11
Treatment procedures:-
Deep friction massage, stretching exercise, and shock wave therapy was applied in both groups as follow:-
-
Deep friction massage:-
-
Put your fingertip pad perpendicularly on the scar tissue.
-
Then move across the scar band in the direction of surrounding normal fibres.
-
Then back and forth motion applied along the length of scar tissue. 12
-
Stretching exercises:-
-
Shockwave therapy:
-
In group A we applied vacuum massage therapy before application of shockwave therapy as follow:-
Vacuum massage therapy:-
-
Use PRUS device (Belgium)
-
The patient position should be comfortable and allow good vision for the area of application.
-
Set device parameters in intensity: 250-900 millibar, frequency: 0.25- 0.50 HZ for 10 min.
-
Then apply shockwave therapy directly after vacuum massage application.
Statistical analysis
Descriptive statistics and an unpaired t-test were applied to compare the age between both groups. Data Normal distribution was tested using the Shapiro-Wilk test for all variables. Variances homogeneity Levene’s test was applied to test the homogeneity between groups. Unpaired t-test was applied to compare the mean values of thickness and visual analogue scale (VSS) between group A and B. Paired t-test was applied to compare between before and after treatment in each group. The significance level for all statistical tests was set at p < 0.05. All statistical analysis was applied through the statistical package for social studies (SPSS) version 25 for windows (IBM SPSS, Chicago, IL, USA).
- Results
- Subject characteristics:
Forty subjects participated in this study. The mean ± SD age of study group (A) was 34.7 ± 6.86 years and that of group B was 35.55 ± 5.78 years. There was no significant difference between both groups in patients age (p = 0.67).
Effect of treatment thickness and VSS:
- Within-group comparison:
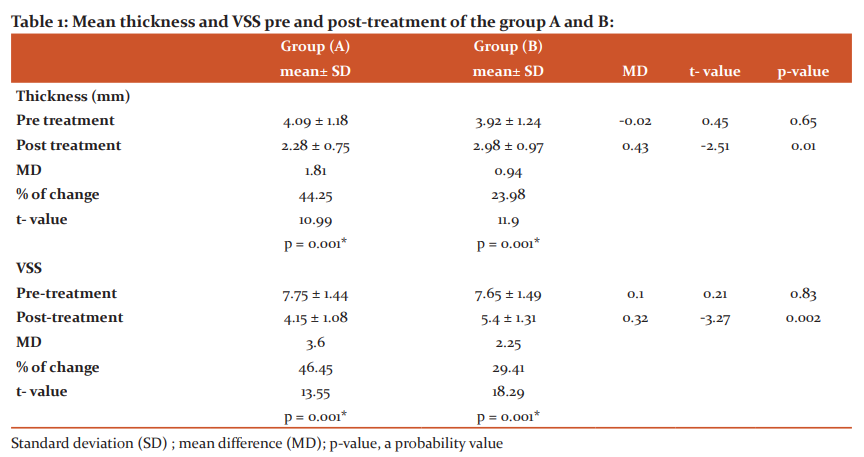
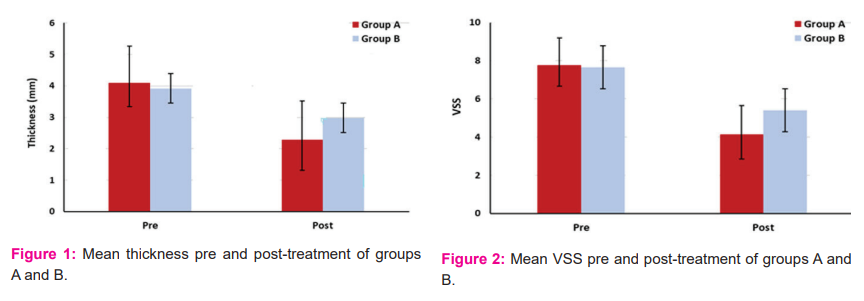
Thickness and VSS post-treatment compared with that pre-treatment in groups A and B significantly decreased (p > 0.001). The decreasing per cent in thickness and VSS in group A was 44.25 and 46.45% respectively, while that in group B was 23.98 and 29.41% respectively. (table 1, figure 1-2).
- Comparison Between groups:
Pre-treatment: there was no significant difference between groups (p > 0.05). Post-treatment: comparison between groups showed a significant decrease in thickness and VSS of group A compared with that of the group (p > 0.01). (table 1, figure 1-2).
Discussion:-
Our trial reported that patients with a hypertrophic scar treated with shockwave therapy and vacuum massage therapy in group A and patients treated with shockwave therapy in group B had a significant decrease in thickness & VSS after treatment compared with those before treatment (p > 0.001). But the decrease per cent in the thickness and VSS in group A (44.25 and 46.45% respectively) was more than in group B (23.98 and 29.41% respectively). So, the post-treatment groups Comparison revealed a significant decrease in thickness and VSS of group A compared with that of the group (p > 0.01).
Zaghloul et al. reported that post-burn hypertrophic scar thickness and appearance significantly decreased according to ultrasonographic measurement (42.55%) and VSS (48.57%) respectively post-application of shockwave therapy in addition to the physiotherapy program.1
Cho et al. revealed that scar pain decreased significantly after the application of shockwave therapy. Also, it was reported that hematological, molecular, microscopic and immunological responses in different cells and plasma decrease pain and induce tissue regeneration.13
Laura et al. reported that the destructive and stimulatory effects of shock waves are dose-dependent. They compared the effects of different doses of shock wave therapy on normal fibroblast proliferation in vitro. After 1 hour from the shock-wave application, the cell viability decreased related both to the energy and the shocks numbers applied: a constant decrease was observed to impulses number (300, 1,000, 2,000) with maximum viability decreasing at 2,000 impulses (18%) while there was no statistically significant association between energy levels and fibroblast viability. 14
Merete et al. reported that vacuum massage had a short-term effect on scar physical properties and there were significant changes in the density of the epidermal layer immediately after the treatment. The thickness of the dermal layer increased significantly immediately after the treatment; after 1 h, and decreased significantly after 2 h compared to baseline. The density of the dermal layer decreased significantly after treatment by vacuum massage, and even at 2 h after treatment, this decrease was still significant compared to baseline. 9
Serup et al. Myofibroblasts (cells responsible for pathological scar formation) were present in the pre-treated scars abundantly, but after application of mechanical pressure therapy myofibroblast activity was suppressed significantly and at the end, myofibroblasts disappeared by apoptosis and collagen fibre alignment improved. 15
Moortgat et al.8 in their review reported that vacuum massage therapy had a positive effect on physical as improvement of tissue hardness, skin elasticity16,17, skinfold thickness18, skin laxity19, skin roughness20, and decrease skin redness21. It also had a positive physiological effect as increasing numbers of fibroblast and collagen fibres.
Conclusion:-
From the gained results it could be concluded that shock wave therapy and vacuum massage therapy are effective in the treatment of the post-burn scar, but the combination treatment between vacuum massage and shock wave is more effective. This increase in effectiveness comes from the ability of vacuum massage to help the reorientation f collagen fibres and decrease the hardness of scar tissue, so it prepared the scar tissue before application of shockwave therapy.
Acknowledgement:-
The authors thank the members and staff of the faculty of physical therapy, south valley university and our colleagues in the department of burns in south valley university hospitals. Also great thanks to all patients who participated in our study.
Conflict of interest:
We have NO affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Individual author’s contribution:
-
Conceived the ideas and experimental design of the study. 1,3
-
Performed data collection.1,2
-
Data analysis and interpretation. 1,2,3
-
Primary author (wrote most paper) 1
-
Revision of scientific content of manuscript.2,3
-
Provide stylistic and grammatical revisions to the manuscript.1,3
References:
-
Mahmoud SZ. et al. ‘Effect of Extracorporeal Shock Wave Therapy on Post Burn Scars’ /Int.J. PharmTech Res. 2016,9(3),p 78-85.
-
Chan SYJ.: “The effectiveness of extracorporeal shockwave therapy on hypertrophic scar appearance and hand mobility in a severe burn patient” Burns O.J. 4 (2020) 72–77.
-
Bombardo KM, Engrave LH, Carrougher GJ, Weichman SA, Faucher I, Costa BA, et al. 'extracorporeal shock wave therapy for the management of burn scars, Dermatol Surg 2012; 38: 778-82.
-
Roseborough, Mark A, Grevious and Raphael C Lee “Prevention and treatment of excessive dermal scarring”. J Natl Med Assoc. January 2004 96(1): 108– 116.
-
Cui HS., “Extracorporeal Shock Wave Therapy alters the expression of fibrosis-related molecules in fibroblast-derived from human hypertrophic scar” Int. J. Mol. Sci. 2018;19,124.
-
Fioramonti P; Cigna E; Onesti MG; Fino P; Fallico Ne; Scuderi N “Extracorporeal Shock Wave Therapy for the Management of Burn Scars” Dermatol surg., 2012; 38:778-82.
-
Z. Rezasoltani, S. Najafi, S. Azizi, B. Forough, N. Maleki and H. Fateh: “The comparison of Shock Wave therapy and Corticosteroid injection on the treatment of Plantar Fasciitis” Ann Mil Health Sci Res., 11 (2013), pp. 53-60.
-
Moortgat P. The physical and physiological effects of vacuum massage on the different skin layers": current status of the literature” Burns Trauma, (2016) 4:34.
-
Merete., "Short-term effects of vacuum massage on the epidermal and dermal thickness and density in burn scars: J Burn Care Res (2016) 4:27.
-
Sullivan T, Smith J, Kermode J, Mclver E, Courtemanche DJ. Rating the Burn Scar. J Burn Care Rehabil. 1990;11:256-260.
-
Truong PT, Lee JC, Soer B, Gaul CA, Olivotto IA. Reliability and validity testing of the Patient and Observer Scar Assessment Scale in evaluating linear scars after breast cancer surgery. Plast Reconstr Surg. 2007;119:487–494.
-
Zhang YT, Li-Tsang CWP, Au RKC. A Systematic Review on the Effect of Mechanical Stretch on Hypertrophic Scars after Burn Injuries" Hong Kong J Occup Ther., 2017; 29(1):1-9.
-
Cho D. Effect of extracorporeal shock wave therapy on scar pain in burn patients” A prospective, randomized, single-blind, placebo-controlled study. Medicine (2016) 95:32.
-
Laura B, Annamaria F, Anna MF, Patrizia ME, Maria GC and Roberto F. Acta Orthopaedica 2009, 80 (5): 612–617.
-
Serup J, Keiding J, Fullerton A, Gniadecka M, Gniadecki R. High-frequency ultrasound examination of the skin: introduction and guide. In: Serup J, Jemec GBE, Grove GL. Handbook of Non-Invasive Methods and the Skin. 2nd ed. 1995, p. 473–92.
-
Márquez-Rebollo C, Vergara-Carrasco L, Díaz-Navarro R, Rubio-Fernández D, Francoli-Martínez P, Sánchez-De la Rosa R. Benefit of endermology on indurations and panniculitis/lipoatrophy during relapsing-remitting multiple sclerosis long-term treatment with glatiramer acetate. Adv Ther. 2014;31: 904–14.
-
Majani UGO, Majani A. Tissue mechano-stimulation in the treatment of scars. Acta Medica Mediterr. 2013; 29:133–4.
-
Monteux C, Lafontan M. Use of the microdialysis technique to assess lipolytic responsiveness of femoral adipose tissue after 12 sessions of mechanical massage technique. J Eur Acad Dermatol Venereol. 2008;22: 1465–70.
-
Revuz J, Adhoute H, Cesarini J, Poli F, Lacarrière C, Emiliozzi C. Clinical and histological effects of the Lift 6 device used on facial skin aging. Les Nouv Dermatologiques. 2002; 21:335–42..
-
Bourgeois JF, Gourgou S, Kramar A, Lagarde JM, Guillot B. A randomized, prospective study using the LPG technique in treating radiation-induced skin fibrosis: clinical and profilometric analysis. Skin Res Technol. 2008;14:71–6.
-
Worret WI, Jessberger B. Effectiveness of LPG treatment in morphea. J Eur Acad Dermatol Venereol. 2004; 18:527–30.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





