IJCRR - 7(20), October, 2015
Pages: 45-54
Date of Publication: 20-Oct-2015
Print Article
Download XML Download PDF
A COMPARATIVE STUDY OF EFFECTS OF A STATIONARY CYCLE AND MOTORIZED TREADMILL AS AN ADJUNCT TO CONVENTIONAL EXERCISES IN IMPROVING THE FUNCTIONAL STATUS OF PATIENTS
WITH KNEE OSTEOARTHRITIS
Author: Shivani Vaid (P.T.)
Category: Healthcare
Abstract:Objective: To determine the effectiveness of different interventions: conventional exercises, and a stationary cycle and motorized treadmill as an adjunct to it in improving the functional status of patients with knee osteoarthritis. Method: Experimental study (RCT type of study). 95 patients with knee osteoarthritis fulfilling the inclusion and exclusion criteria of the study were studied. Patients were randomly allotted by envelope method to any of the three groups. All patients were subjected to a standardized assessment including the detailed demographic details, Visual Analogue Scale (VAS) for assessing pain, 36, 61 The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) for pain, stiffness and physical function, 33, 62 Timed Up and Go test (TUG) for assessing physical function and balance, 63, 64, 65 and Single Leg Standing test (SLST) for assessing balance, 65 were taken post 1 week and post 2 weeks of the intervention. The intervention was given on thrice a week schedule for total two weeks follow up. Difference between the three groups was compared by statistical methods.
Result: The study shows that irrespective of the demographic characteristics and the other parameters (OA grade, leg dominance, U/L or B/L, etc.), all the three intervention groups A, B and C are homogenous and comparable and effective intervention types showing statistically significant difference. Conclusion: The study shows a statistically highly significant result of Group C, i.e. motorized treadmill within sub maximal limits should be used as an adjunct to conventional exercises for treating Grade I and Grade II knee osteoarthritis patients in improving their functional status.
Keywords: Knee osteoarthritis, Conventional exercises, Stationary cycle, Motorized treadmill
Full Text:
INTRODUCTION
There are more than hundred types of arthritis. The most common type of arthritis is osteoarthritis (OA) or degenerative joint disease. It is a leading cause of disability and commonly affects the middle aged and elderly, although younger people may be affected as a result of injury or overuse. It is often more painful in weight bearing joints such as knee, hip and spine than the wrist, elbow and shoulder joints. Knee OA is a degenerative disease of knee joint, more common in people older than 40 years, predominantly considered a wear and tear process, where there is gradual degradation of the hyaline cartilage that covers the articulating surfaces of the bones of the knee joint. Symptoms may include joint pain, tenderness, stiffness, effusion, decreased movement secondary to pain, muscle weakness, ligament laxity, and radiological changes such as loss of joint space and osteophytes.17 Activities like walking, squatting and stair climbing are affected the most. The incidence of knee OA in India is as high as 12%. According to the International Journal of Rheumatic Disease 2011, the Community Program for Control of Rheumatic Disease (COPCORD) studies conducted in India revealed a significantly higher prevalence of knee pain in the rural (13.7%) compared to urban (6%) community.18, 20 According to The European League against Rheumatism (EULAR) committee report 2012, knee OA is likely to become the 4th most important global cause of disability in women and the 8th most important in men. Moreover, studies over the years have suggested that postural stability and balance control are also altered in people with OA, increasing their risk to falls.12, 14 These findings suggest that modification of traditional rehabilitation programs may improve the overall effectiveness of exercise therapy for people with knee OA. The management of OA is broadly divided into non pharmacological, pharmacological and surgical. Surgical management is generally reserved for failed medical management where functional disability affects the patient’s quality of life. Exercises are considered one of the major interventions in the conservative or non pharmacological treatment of patients with knee osteoarthritis.1, 35 Stationary cycle, a low impact aerobic exercise, proves to be beneficial to improve general fitness, pain and function in patients with knee OA by unloading compressive forces on the knee joints.1, 26 Motorized treadmill, though considered a high impact aerobic exercise, if the speed and inclination is kept within the submaximal limits, 15 may prove to be a better low impact exercise for patients with knee osteoarthritis, as the person is required to walk in the functional position, which is required for the activities in daily living. The present study compares the effects of a stationary cycle and motorized treadmill as an adjunct to conventional exercises in improving the functional status of patients with knee osteoarthritis.
MATERIALS
• Plinth
• Chair with arm rest
• Measuring tape - small - Large (30 m)
• Weighing scale – manual with 1 kg increment
• Stadiometer instrument
• Stop watch application available in mobile
• Pillows
• Sandbag or cloth pad
• Motorized treadmill (Kamachi company)
• Stationary cycle (Body Gym company) • Climbing stool • Parallel bars • Pen, pencil, eraser and sharpener • Ruler and stapler • Notebook • Written informed consent • Patient information sheet • Data collection sheet • Exercise handouts
METHOD STUDY DESIGN: Experimental study (RCT type of study)
SETTING OF THE STUDY: This study was conducted in Physiotherapy department, SSG Hospital, Vadodara.
DURATION OF THE STUDY: Study was completed over a period of four months i.e. December 2013 to March 2014.
SAMPLE SIZE: The difference between means of TUG of group A and group B is 0.76 and S.D (standard deviation) of group A is 0.48 and group B is 0.91 (from pilot study done on 30 knee OA patients referred to OPD 16, S.S.G Hospital, Vadodara, Gujarat, India fulfilling the inclusion and exclusion criteria of the study). With α risk 5% and power 90, the minimum expected sample size in each group came to 20, considering non responsive rate 20%, the minimum total sample size came to 72. [Ref: Med Cal C Version 12.50] 95 patients with knee osteoarthritis fulfilling the inclusion and exclusion criteria of the study were studied.
STUDY POPULATION: Patients coming to Outpatient department and being referred to OPD-16, College of Physiotherapy, S.S.G Hospital, Vadodara, Gujarat, India, at morning time, as new patients with knee OA, fulfilling the inclusion and exclusion criteria of the study.
SAMPLING METHOD: Patients were randomly allotted by envelope method to either of the Three groups: Group A: Conventional Exercises
Group B: Conventional Exercises + Stationary Cycle (voluntary speed) Group
C: Conventional Exercises + Motorized Treadmill (sub maximal speed, 0 inclinations)
SELECTION CRITERIA:
Inclusion criteria: 1
. Age: 40-75 years;
2. Grade I or II on Lawrence and Kellegren Radiological Classification;
3. Osteoarthritis knee (OA Knee) diagnosed according to the American College
Exclusion criteria:
1. Pace maker use or used;
2. Unstable heart conditions;
3. Going to participate in another physical activity program;
4. Inability to pedal a stationary cycle;
5. Inability to walk;
6. Previous knee or hip arthroplasty;
7. Epilepsy;
8. Presence of tumor or cutaneous lesion that could interfere with the procedure;
9. Previous traumatic history;
10. Other significant neurological and musculoskeletal disorders.
DATA COLLECTION AND METHODOLOGY
A written and informed consent about enrolment in the interventional study and maintaining adequate privacy and confidentiality was taken from all the patients included in the study. All patients were subjected to a standardized assessment including the detailed demographic details, Visual Analogue Scale (VAS) for assessing pain, 36,61 The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) for assessing pain, stiffness and physical function,33,62 Timed Up and Go test (TUG) for assessing physical function and balance,63,64,65 and Single Leg Standing test (SLST) for assessing balance in patients.65 A detailed clinical, past, personal and family history was taken to rule out any other cause other than idiopathic or primary knee osteoarthritis. Subcommittee on Osteoarthritis of the American College of Rheumatology has defined OA as “A heterogeneous group of conditions that lead to joint symptoms and signs which are associated with defective integrity of articular cartilage, in addition to related changes in the underlying bone at the joint margins.”19 Patients of knee OA were taken from the new cases referred to OPD-16, College of Physiotherapy, S.S.G Hospital, Vadodara. They were randomly allotted by envelope method to any of the three groups: Group A: Conventional Exercises Group B: Conventional Exercises + Stationary Cycle (voluntary speed) Group C: Conventional Exercises + Motorized Treadmill (sub maximal speed, 0 inclinations)
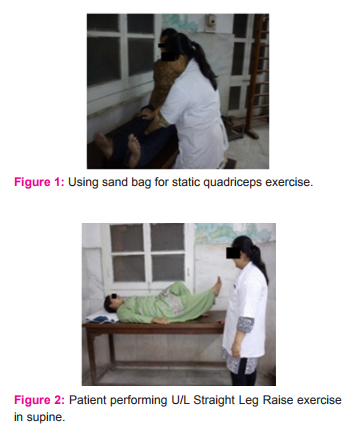
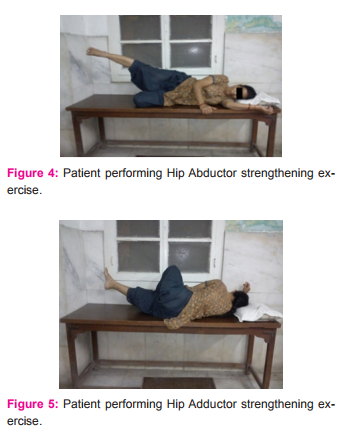
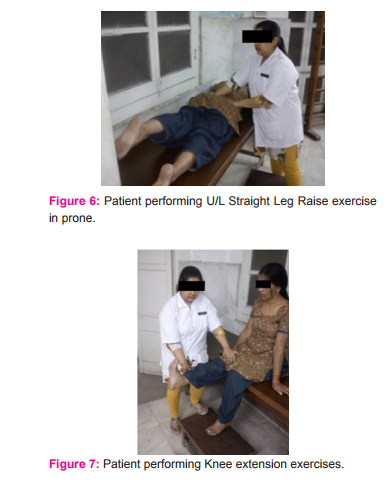
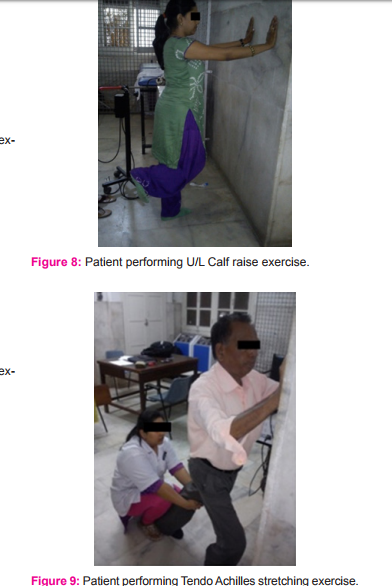
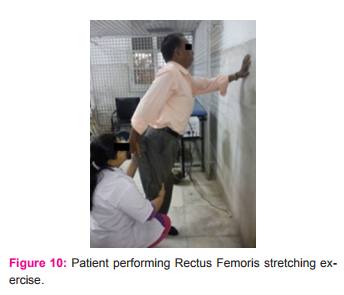
Group A patients were given Conventional exercises according to the American Academy of Orthopedic Surgeons (AAOS) guidelines and protocol for knee conditioning, which includes:

Group B patients were given stationary cycle as a form of exercise adjunct to the conventional exercises. It was given for 10 minutes after the conventional exercises at patient’s voluntary speed.1 (Figure 11.1 and 11.2)

Group C patients were given motorized treadmill as a form of exercise adjunct to the conventional exercises. It was given for 10 minutes after the conventional exercises at sub maximal speed according to Modified Bruce Protocol, 37 starting with the default lowest speed of treadmill being 0.8 miles per hour and gradually increasing, but not exceeding the speed of 1.7 miles per hour, and at 0 degree inclination level. (Figure 12.1 and 12.2)


Each group and each patient was given the same attention by the physiotherapist and the exercises were given with same care and precaution. Patients were allowed to follow the orthopedic advices and the prescribed medication. The assessment was done using the outcome measures VAS, WOMAC, TUG and SLST taken on the date of admission to OPD-16. These outcome measures were again taken post 1 week and post 2 weeks of the intervention. The intervention was given on thrice a week schedule for total two weeks follow up. Difference between the three groups was compared by statistical methods.
RESULT
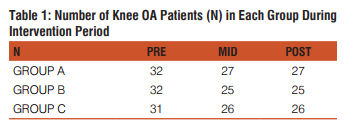
The result states that irrespective of the demographic characteristics (age, sex, BMI, etc.) and the other parameters (OA grade, leg dominance, U/L or B/L, etc.), all the three intervention groups A, B and C are homogenous, comparable and effective intervention types showing statistically significant difference.
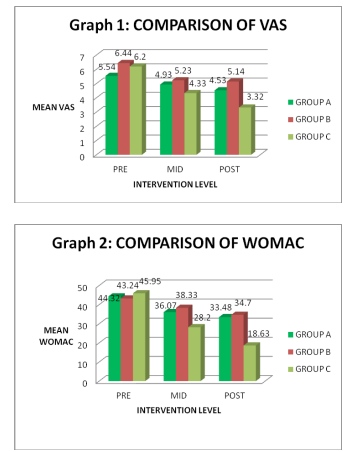
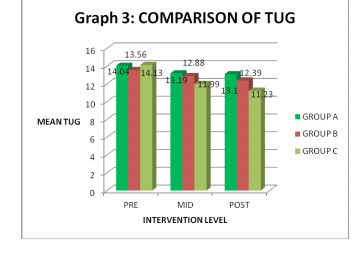
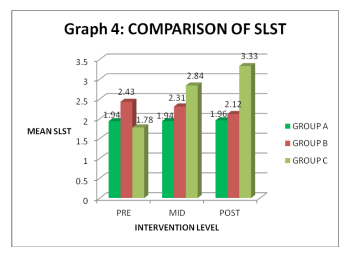
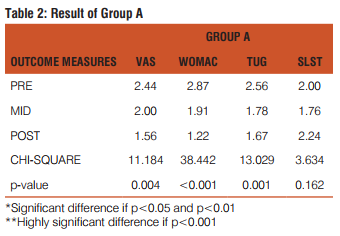
The study shows a statistically significant result of Group A, i.e. conventional exercises as an intervention type, in improving VAS and TUG scores, and a highly significant result in improving WOMAC scores, but there was statistically no significant result in improving SLST scores, in patients with knee osteoarthritis. (Table 2)
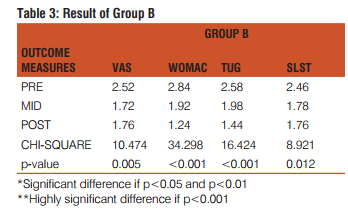
The study shows a statistically significant result of Group B, i.e. stationary cycle adjunct to conventional exercises as an intervention type, in improving VAS and SLST scores, and a highly significant result in improving WOMAC and TUG scores, in patients with knee osteoarthritis. (Table 3)
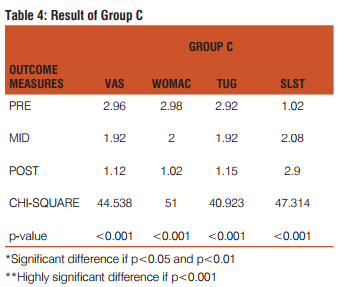
The study shows a statistically highly significant result of Group C i.e. motorized treadmill adjunct to conventional exercises, as an intervention type, in improving all the four outcome measures scores VAS, WOMAC, TUG and SLST scores, in patients with knee osteoarthritis.(Table 4)
DISCUSSION
Osteoarthritis (OA) also called as degenerative joint disease (DJD) is the most common of all joint diseases to affect mankind. Although joint inflammation is implied by the suffix ‘itis’, in osteoarthritis, inflammation is typically found only after there has been substantial articular degeneration.38 Approximately 40% of adults older than the age of 70 suffer from OA of the knee, 80% of people with OA knee have limitation of movement, and 25% cannot perform their major daily activities of living.39 Predisposition to knee OA increases in Asians, especially Indians as there is a common thread that binds millions of inhabitants in near similar lifestyles ranging from squatting and kneeling to sitting cross legged on ground for prayers.40 Knee OA is associated with considerable disability and functional limitation is an inevitable consequence. Studies over the years have suggested that postural stability and balance control are also altered in people with OA, increasing their risk to falls, 12, 14 the need for a specific intervention type hence becomes important. Oliveria AM, Peccin MS, Silva KN, Teixeira LE, Trevisani VF. (2012) studied the impact of exercise on the functional capacity and pain of patients with knee osteoarthritis on a thrice a week intervention for 8 weeks comparing the exercise group which included stationary cycle along with exercises and an instruction group and concluded Quadriceps strengthening exercises for eight weeks are effective to improve pain, physical function, and stiffness of patients with knee OA. Strengthening exercises combined with stretching and stationary bike should be implemented in rehabilitation programs of patients with knee OA.1 The present study compared the conventional exercises and stationary cycle as an adjunct to conventional exercises as two different intervention groups A and B, and found that group B gives more significant results than group A (table 2 and 3), which supports the conclusion of the above study, that strengthening exercises combined with stretching and stationary bike should be implemented in rehabilitation programs of patients with knee OA. Moreover the present study also compared motorized treadmill as an adjunct to conventional exercises i.e. group C with the other two groups A and B, and found that group C gives the most significant results out of the three groups, with pvalue <0.001 for VAS, WOMAC, TUG and SLST suggesting the highly significant results (table 4), which states that conventional exercises along with motorized treadmill as an adjunct should be implemented in rehabilitation programs of patients with knee OA for improving their functional status. Damiano DL, Norman TL, Stanley CJ, Park HS. (2011) studied the kinetics and kinematics analysis of elliptical training, stationary cycling, treadmill walking and over ground walking and found that treadmill walking excursion, position, gait deviation index (GDI) and variability were very similar to those of over ground walking showing kinematic and coordinative similarity, whereas elliptical training and stationary cycling showed unique patterns of differences from over ground walking. In stationary cycling the three joints hip, knee and ankle were highly coupled and constrained to move in unison. The study concluded that if kinematic similarity was the sole determinant of skill transfer, then a treadmill would be the universally preferred device. However, other devices may promote different aspects of the target task that may be even more important for transfer, particularly in varied rehabilitation applications.2
In the present study, motorized treadmill shows more significant results as an adjunct to conventional exercises than stationary cycle in improving the functional status of knee OA patients (table of 3 and 4), but supporting the above study conclusion stationary cycle may give better results in improving the range of movement of the knee joint wherein the range is limited following specific disorders. Hunt MA, McManus FJ, Hinman RS, Bennell KL. (2010) studied the predictors of Single Leg Standing balance in individuals with medial knee osteoarthritis and concluded that given the reduced balancing ability in this patient population, interventions targeting these factors are necessary.11 Another study by Kim HS, Yun DH, Yoo SD, Kim DH, Jeong YS, Yun JS, Hwang DG, Jung PK, Choi SH. (2011) on balance control and knee osteoarthritis severity and concluded that evaluation of balance control and education aimed at preventing falls would be useful to patients with knee OA.8 Supporting the above studies conclusion, the present study showed group C i.e. motorized treadmill as an adjunct to conventional exercises, as more significant intervention for knee OA patients in improving their functional status (table 4), As walking on a motorized treadmill is in a functional position for the patient where he bears equal weight on both legs because of the moving belt. And when within the sub maximal limits, the stance phase is same for both legs increasing the balance and reducing the risk to fall, as well as reduces the lurching or leaning to one side, a common finding in knee OA patients. The results from the statistical analysis of the present study support the alternative hypothesis which suggests that there is a significant difference between the effects of a stationary cycle and motorized treadmill as an adjunct to conventional exercises in improving the functional status of patients with knee osteoarthritis.
CONCLUSION
The study shows a statistically highly significant result of Group C i.e. motorized treadmill adjunct to conventional exercises, as an intervention type, in improving all the four outcome measures scores VAS, WOMAC, TUG and SLST scores, in patients with knee osteoarthritis. Thus, Group C i.e. motorized treadmill adjunct to conventional exercises, is more effective intervention type for improving the functional status of patients with knee osteoarthritis. Hence, motorized treadmill within sub maximal limits should be used as an adjunct to conventional exercises for treating Grade I and Grade II knee osteoarthritis patients in improving their functional status.
ACKNOWLEDGEMENT
Any accomplishment cannot be performed single handed but requires the efforts of many individuals. Firstly, I am thankful to GOD who always kept my faith inbuilt in me as a constant force of encouragement, support and trust. I have been privileged to have the direction and guidance from my P.G. Guide Beena Kodnani, Senior Lecturer, College of Physiotherapy, Vadodara, who has remained generous with her time and guided me with her resourceful knowledge. I acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. I am also grateful to the authors, editors and publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. I thank Dr. A.T.Leuva, Dean, Faculty of Medicine, M.S.University of Baroda and Dr. R.N. Daveshwar, Medical Superintendent, S.S.G.Hospital, Vadodara for permitting me to carry out the study in the hospital. I would like to thank Dr Vikas Doshi, Assistant Professor in PSM department, Baroda Medical College, for helping me in statistical analysis of the results of this study. My heartfelt appreciation goes to all the patients who generously volunteered to participate in the study; they deserve my utmost respect for keeping faith in me. I am thankful to my colleagues in Master of Physiotherapy, for being with me always and helping me continuously in all manners. Finally, I owe to my parents Dr. Sanjiv Vaid and Jyoti Vaid and my brother Ankit Vaid for always believing in me and encouraging me to achieve my goals.
References:
1. Oliveria AM, Peccin MS, Silva KN, Teixeira LE, Trevisani VF. Impact of exercise on the functional capacity and pain of patients with knee osteoarthritis: a randomized clinical trial. Rev Bras Rheumatol 2012; 52(6):870-882.
2. Damiano DL, Norman TL, Stanley CJ, Park HS. Comparison of elliptical training, stationary cycling, treadmill walking and over ground walking. Damiano et al. Gait Posture 2011; 34(2):260- 264.
3. Prosser LA, Stanley CJ, Norman TL, Park HS, Damiano DL. Comparison of elliptical training, stationary cycling, treadmill walking and over ground walking. Prosser et al. Gait Posture 2011; 33(2):244-250.
4. Hurley MV, Scott DL, Rees J et al. Sensorimotor changes and functional performance in patients with knee osteoarthritis. Ann Rheum Dis 1997; 56:641-648.
5. Takacs J, Anderson JE, Leister J RS, MacDonald PB, Peeler JD. Lower body positive pressure: an emerging technology in the battle against knee osteoarthritis. Takacs J et al. Clinical Interventions in Aging 2013; 8:983-991.
6. Brosseau L, Wells GA, Kenny GP, Reid R, Maetzel A, Tugwell p, Huijbregts M, McCullough C, De Angelis G, Chen L. The Implementation of a community- based aerobic walking program for mild to moderate knee osteoarthritis: a knowledge translation randomized controlled trial: Part II: Clinical outcomes. Brosseau L et al. BMC Public Health 2012; 12:1073.
7. Brosseau L, Wells GA, Kenny GP, Reid R, Maetzel A, Tugwell p, Huijbregts M, McCullough C, De Angelis G, Chen L. The Implementation of a community- based aerobic walking program for mild to moderate knee osteoarthritis: a knowledge translation randomized controlled trial: Part I: The uptake of the Ottawa panel clinical practice guidelines. BMC Public Health 2012; 12:871.
8. Kim HS, Yun DH, Yoo SD, Kim DH, Jeong YS, Yun JS, Hwang DG, Jung PK, Choi SH. Balance control and knee osteoarthritis severity. Ann Rehabil Med 2011; 35:701-709.
9. Olestad BE, Osteras N, Frobell R, Grottle M, Brogger H, Risberg MA. Efficacy of strength and aerobic exercise on patientreported outcomes and structural changes in patients with knee osteoarthritis: study protocol for a randomized controlled trial. Olestad et al. BMC Musculoskeletal Disorders 2013; 14:266.
10. Mangione KK, Axen K, Haas F. Mechanical unweighting effects on treadmill exercise and pain in elderly people with osteoarthritis of the knee. PHYS THER 1996; 76:387-394.
11. Hunt MA, McManus FJ, Hinman RS, Bennell KL. Predictors of Single Leg Standing balance in individuals with medial knee osteoarthritis. Hunt et al. Arthritis Care and Research 2010; pp: 496-500.
12. Park JH, Ko S, Hong HM, Ok E, Lee JI. Factors related to standing balance in patients with knee osteoarthritis. Ann Rehabil Med 2013; 37(3):373-378.
13. Peat G, Thomas E, Dunean R, Wood L, Hay E, Croff P. Clinical classification criteria for knee osteoarthritis: performance in the general population and primary care. Ann Rheum Dis 2006; 65:1363-1367.
14. Hinman RS, Bennel KL, Metcalf BR, Crossley KM. Balance impairments in individuals with symptomatic knee osteoarthritis: a comparison with matched controls using clinical tests. Rheumatology 2002; 41:1388-1394.
15. Spyropoulos P, Armstrong C, Chtomopoulos E, Kwiatkowski B, Babatsikou F. Impact loading in osteoarthritic women during varied walking conditions. Health Science Journal 2008; pp: 51- 58; ISSN: 1108-7366.
16. Purser JL, Golightly YM, Feng Q, Helmick CG, Renner JB, Jordan JM. Slower walking speed is associated with incident knee osteoarthritis- related outcomes. Arthritis Care Res (Hoboken) 2012; 64(7):1028-1035.
17. Thorstensson CA, Petersson IF, Jacobsson L TH, Boegard TL, Roos EM. Reduced functional performance in the lower extremity predicted radiographic knee osteoarthritis five years later. Ann Rheum Dis 2004; 63:402-407.
18. Fransen M, Bridgett L, March L, Hoy D, Penserga E, Brooks P. The epidemiology of osteoarthritis in Asia. International Journal of Rheumatic Diseases 2011; 14:113-121.
19. Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the knee. Arthritis Rheum 1986; 29:1039-1049.
20. Haq SA, Rasker JJ, Daremawan J, Chopra A. WHO-ILARCOPCORD in the Asia-Pacific: the past, present and future. International Journal of Rheumatic Diseases 2011; 14:113-121.
21. Messier SP, Mihalko SL, Beavers DP, Nicklas BJ, DeVita P, Carr JJ, Hunter DJ, Williamson JD, Bennel KL, Geurmasi A, Lyles M, Loesser RF. Strength Training for Arthritis Trial (START): design and rationale. Messier et al. BMC Musculoskeletal Disorders 2013; 14:208.
22. Helmark IC, Mikkelsen HR, Berglum J, Rothe A, Petersen M CH, Andersen O, Langberg H, Kjaer M. Exercise increases interleukin-10 levels both intra-articularly and peri-synovially in patients with knee osteoarthritis: a randomized controlled trial. Helmark et al. Arthritis Research and Therapy 2010; 12:R126.
23. Lin C WC. March L, Crosbie J, Crawford R, Graves S, Naylor J, Harmer A, Jan s, Bennel K, Harris I, Parker D, Moffet H, Fransen M. Maximum recovery after knee replacement- the MARKER study rationale and protocol. BMC Musculoskeletal Disorders 2009; 10:69.
24. Kassavou A, Turner A, French DP. Do interventions to promote walking in groups increase physical activity- a meta analysis. International Journal of Behavioral Nutrition and Physical Activity 2013; 10:18.
25. Ni GX, Lei L, Zhou YZ. Intensity dependent effect of treadmill running on lubricin metabolism of rat articular cartilage. Arthritis Research and Therapy 2012; 14:R256.
26. Salacinski AJ, Krohn K, Lewis SF, Holland ML, Ireland K, Marchetti G. The effects of group cycling on gait and pain related disability in individuals with mild to moderate knee osteoarthritis: a randomized controlled trial. J Ortho Sports Phys Ther 2012; 42(12):985-95.
27. Takacs J, Kirkham AA, Perry F, Brown J, Marriot E, Monkman D, Havey J, Hung S, Campbell KL, Hunt MA. Lateral trunk lean gait modification increases the energy cost of treadmill walking in those with knee osteoarthritis. Osteoarthritis Cartilage 2013; pii: S1063-4584(13)01035-2.
28. Roper JA, Bressel E, Tillman MD. Acute aquatic treadmill exercise improves gait and pain in people with knee osteoarthritis. Arch Phys Med Rehabil 2013; 94(3):419-25.
29. Haq SA, Davatchi F. Osteoarthritis of the knees in the COPCORD world. International Journal of Rheumatic Diseases 2011; 14:122-129.
30. Ebnezar J, Nagarathna R, Bali Y, Nagendra HS. Effect of integrated yoga therapy on pain, morning stiffness and anxiety in osteoarthritis of the knee joint: a randomized control study. Int J Yoga 2012; 5(1):28-36.
31. Lutyen FP, Denti M, Filardo G, Kon E, Engebresten L. Definition and classification of early osteoarthritis of the knee. Knee Surg Sports Traumatol Arthrosc 2012; 20(3): 401-406.
32. Kellegren JH, Lawrence JS. Radiological assessment of osteoarthrosis. Ann Rheumatol Dis 1957; 16(4): 494-502.
33. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument measuring clinically important patient relevant outcomes to anti rheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 1988; 15(12): 1833-40.
34. Hochberg MC, Altman RD, April KT, Benkhalti M, Guyatt G, McGowan J, Tuwheed T, Welch V, Wells G, Tugwell P. American College of Rheumatology 2012 recommendations for the use of non pharmacological therapies in osteoarthritis of the hand, hip and knee. Arthritis Care and Research 2012; pp: 465- 474.
35. Jevsevar DS, Brown GA, Jones DL, Matzkin EG, Manner P, Mooar P, Schouseboe JT, Stovitz S, Sanders JO, Bozic K, MartinIII WR, Cummins DS, Woznica A. Treatment of osteoarthritis of the knee: Evidence based guidelines, 2nd edition. J Am Acad Ortho Surg 2013; 21:571-576.
36. Averbuch M, Katzper M. Assessment of Visual Analog versus categorical scale for measurement of osteoarthritis pain. J Cin Pharmacol 2004; 44(4):368:72.
37. McInnis KJ, Balady GJ. Comparison of sub maximal exercises responses using the Bruce versus Modified Bruce protocols. Med Sci Sports Exerc 1994; 26(4):103-7.
38. Physical rehabilitation. Susan B O’Sullivan, Thomas J. Schmitz.
39. World Health Organization and the Bone and Joint Decade, 2001. Available at: http://www.boneandjointdecade.org. Accessed May 2002.
40. Bindya Sharma efficacy of knee osteoarthritis outcome score (KOOS) in measuring functional status of knee osteoarthritis patients in Indian population. Indian Journal of Physiotherapy and Occupational Therapy July-Sept., 2012, Vol. 6, No. 3.
41. Felson DT, Naimark A, Anderson J, Kazis L, Castelli W, Meenan RF. The prevalence of knee osteoarthritis in the elderly. The Framingham Osteoarthritis Study. Arthritis and Rheumatism 1987; 30:914-918.
42. Australia A. Painful Realities. The economic impact of arthritis in Australia in 2007, 2007.
43. Hamerman D. clinical implications of osteoarthritis and aging. Annals of Rheumatic Diseases 1995; 54:82-85.
44. Badley E, Wang P. Arthritis and the aging population: projection of arthritis prevalence in Canada 1991 to 2031. Journal of Rheumatology 1998, 25(1):138-144.
45. Ledingham J, Regan M, Jones A, Doherty M. Radiographic patterns and associations of osteoarthritis of knee in patients referred to hospital. Ann Rheum Dis 1993; 52(7):520-526.
46. Ioro R, Healy WL. Unicompartmental arthritis of the knee. J Bone Joint Surg Am 2003; 85-A (7):1351-1364.
47. Guccione AA, Felson DT, Anderson JJ, Anthony JM, Zhang Y, Wilson PWF, Kelly-Hayes M, Wolf PA, Kreger BE, Kannel WB. The effects of specific medical conditions on the functional limitations of elders in the Framingham study. American journal of Public Health 1994; 84:351-358.
48. Dieppe PA, Ebrahim S, Martin RM, Juni P. Lessons from the withdrawal of rofecoxib. Bio Med Journal 2004; 329(7471):867- 868.
49. Jordan K, Arden N, Doherty M, Bannwarth B, Bijlsma J, Dieppe P, Gunther K, Hauselmann H, Herrero-Beaumont G, Kaklamanias P, et al. EULAR recommendations 2003: an evidence based approach to the management of knee osteoarthritis. Report of a task force of the Standing Committee for International Clinical Studies Including Therapeutic Trails (ESCISIT). Annals of Rheumatic Diseases 2003; 62:1145-1155.
50. OA ASo: Recommendations for the medical management of osteoarthritis of the hip and knee. 2000 update. Arthritis and Rheumatism 2000; 43(9):1905-1915.
51. Guccione AA, Felson DT, Anderson JJ, et al. The effects of specific medical conditions on the functional limitations of elders in the Framingham Study. Ann J Public Health 1994; 84:351-358.
52. Creamer P, Lethbridge-Cejku M, Hochberg MC. Where does it hurt? Pain localization in osteoarthritis of the knee. Osteoarthritis Cartilage 1998; 6:318-323.
53. Messier SP, Loeser RF, Hoover JL, et al. Osteoarthritis of the knee: effects on gait, strength and flexibility. Arch Phys Med Rehabil 1992; 73:29-36.
54. Fisher NM, White SC, Yack HJ, et al. Muscle function and gait in patients with knee osteoarthritis before and after muscle rehabilitation. Disabil Rehabil 1997; 19:47-55.
55. Rogind H, Bibow-Nielson B, Jenson B, et al. The effects of a physical training program on patients with osteoarthritis of the knees. Arch Phys Med Rehabil 1998; 79:1421-1427.
56. Van Baar ME, Assendlft WJ, Dekker J, et al. Effectiveness of exercise therapy in patients with osteoarthritis of the hip or knee: a systematic review of randomized clinical trials. Arthritis Rheum 1999; 42:1361-1369.
57. Fischer NM, Pendergast DR, Gresham GE, Calkins E. Muscle rehabilitation: its effect on muscular and functional performance of patients with knee osteoarthritis. Arch Phys Med Rehabil 1991; 72:367-374.
58. Hochberg MC, Altman RD, Brandt KD, et al. Guidelines for the medical management of osteoarthritis, part II: osteoarthritis of the knee. American College of Rheumatology. Arthritis Rheum 1995; 38:1541-1546.
59. Deyle GD, Henderson NE, Matekel RL, et al. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee: a randomized controlled trial. Ann Intern Med 2000; 132:173-181.
60. Beard DJ, Dodd CA, Trundle HR, Simpson AH. Proprioception enhancement for anterior cruciate deficiency: a prospective randomized trial of two physiotherapy regimes. J Bone Joint Surg Br 1994; 76:654-659.
61. Hawker GA, Mian S, Kendzerska T, French M. Measures of Adult Pain. Arthritis Care and Research 2011; pp: S240-S252.
62. Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). American College of Rheumatology. Available at http://www.rhematology.org.
63. Timed Up and Go (TUG) Test. American College of Rheumatology. Available at http://www.rhematology.org.
64. Hayes KW, Johnson ME. Measures of Adult General Performance Tests. Arthritis Care and Research 2003; pp: S28-S42.
65. Mancini M, Horak FB. The relevance of clinical balance assessment tools to differentiate balance deficits. Eur J Phys Rehabil Med 2010; 46(2):239-248.
66. Messier SP, Royer TD, Craven TE, O’toole ML, Burns R, Ettinger WH. Journal of the American Geriatrics Society 2000; ISSN:0002-8614; pp:131-138.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





