IJCRR - 7(20), October, 2015
Pages: 41-44
Date of Publication: 20-Oct-2015
Print Article
Download XML Download PDF
POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME (PRES) IN PREGNANCY
Author: Pratik J. Mavani, Hina V. Oza, Hafsa M. Vohra
Category: Healthcare
Abstract:Aims and Objective: Explain association and outcome of Posterior Reversible Encephalopathy Syndrome in Pregnancy. Method: This is a Retrospective Study based on obstetric patients visited at Civil Hospital, Ahmedabad, Gujarat, India withconvulsion and/or alteration of sensations in the period of 2 YEARS from July 2013 to July 2015. These patients diagnosed as Posterior Reversible Encephalopathy Syndrome with help of MRI Brain. Details of these patients like history, examination and investigation findings recorded and final data analysis done. Results: All patients with Posterior Reversible Encephalopathy Syndrome had convulsions and alteration of sensations. Development of Posterior Reversible Encephalopathy Syndrome is more common in primigravida, antenatal patients with average age of 21 year. There is increased rate of preterm delivery and Neonatal ICU admissions in neonates which increases morbidity and mortality of babies. Conclusion: Posterior Reversible Encephalopathy Syndrome develops more commonly in Primigravida Antenatal patients during Third decade of their life. In Posterior Reversible Encephalopathy Syndrome there are increased incidences of unconsciousness, Caesarean delivery, Intensive Care Unit admissions (peripartum morbidity), preterm babies (Neonatal ICU admission) and perinatal mortality. Though Posterior Reversible Encephalopathy Syndrome increases maternal morbidity, no maternal mortality seen.
Keywords: Posterior reversible encephalopathy syndrome, MRI brain
Full Text:
INTRODUCTION
Posterior Reversible Encephalopathy Syndrome (PRES)1,2 is a clinicoradiological entity that was explained by Hinchey3 . This condition has been designated by a variety of names like Reversible Posterior Leuko encephalopathy Syndrome, Reversible Posterior Cerebral Oedema Syndrome and Reversible Occipital Parietal Encephalopathy
ASSOCIATIONS
• Posterior Reversible Encephalopathy Syndrome can develop in association with a vast array of conditions. However, regardless of the underlying cause, the main abnormality is cerebral vasogenic oedema3 . • Hypertensive encephalopathy, eclampsia-preeclampsia, renal failure, vasculitis, immunosuppressive treatment, electrolyte imbalance and hyper calcaemia have been reported to be major causes of this syndrome.
PATHOPHYSIOLOGY
• ONE THEORY posits a hypertension-induced auto regulatory failure. In Posterior Reversible Encephalopathy Syndrome auto regulatory response maintaining blood pressure is abnormal resulting in a breakdown of the normal blood brain barrier and culminating in vasogenic brain oedema.1,2
• SECOND THEORY posits that excessive arteriolar vasoconstriction results in decreased blood flow, ischemia. Sepsis that leads to endothelial injury also seem to have a role in the pathogenesis.1,2 This Oedema presents without infarction. Therefore accurate treatment is imperative to halt progression and if we remove the cause we can prevent permanent damage. The preferential involvement of the parietal and occipital lobes is thought to be related to the relatively poor sympathetic innervation of the posterior circulation.
DIAGNOSIS
Clinical Manifestations of Posterior Reversible Encephalopathy Syndrome:
• It is clinically characterized by variable associations of seizure activity, alteration of sensations, headache, visual abnormalities, nausea/vomiting, and focal neurological signs.3,6,7,8,11
• Consciousness impairment may range in severity from confusion, somnolence, and lethargy to encephalopathy or coma
Radiological Characteristics of Posterior Reversible Encephalopathy Syndrome:
• It was believed to consistently produce bilateral and symmetric regions of oedema typically located in the white matter and predominating in the posterior parietal and occipital lobes.3,4,6,11
• Cerebral MRI is the key investigation for the diagnosis of Posterior Reversible Encephalopathy Syndrome.
• Fluid-attenuated inversion recovery (FLAIR) sequences also visualize the lesions.
The four radiological patterns of Posterior Reversible Encephalopathy Syndrome11:-
1. Holohemispheric watershed pattern (23 %)
2. Superior frontal sulcus pattern (27 %)
3. Dominant parietal-occipital pattern (22 %)
4. Partial or asymmetric expression of the primary patterns (28 %)
TREATMENT
It is important to treat patients with Posterior Reversible Encephalopathy Syndrome as soon as recognized to avoid the risk of irreversible injury. However, permanent neurological impairment occurs in a minority of patients. 5,7
Correction of the underlying cause of Posterior Reversible Encephalopathy Syndrome:
• In Preeclampsia-eclampsia related Posterior Reversible Encephalopathy Syndrome definitive treatment consists of immediate delivery (i.e. induction or caesarean section), general measures (e.g. Intravenous fluids, thrombo prophylaxis), Blood pressure control, prevention and/or treatment of seizures must be provided.
General measures
• Patients with Posterior Reversible Encephalopathy Syndrome require the symptomatic measures usually taken in the Intensive Care Unit. The need for upper airway protection should be evaluated continuously in patients with marked consciousness impairment or seizure activity. 9,10
Antiepileptic treatment
• Intravenous benzodiazepines (clonazepam 1 mg or diazepam 10 mg) given. The dose can be repeated up to three times if necessary.
• Patients with refractory status epilepticus need midazolam, propofol or thiopental in titrated doses until remission of the clinical seizure activity.
• Inj. mannitol 100 ml intravenous 8 hourly.
MATERIAL AND METHOD
Study type: Retrospective study
No. of patients (n): 9
Place: B. J. Medical College and Civil Hospital, Ahmedabad, Gujarat, India.
Exclusion criteria: Obstetric Patients having Convulsion and not having alteration of sensations in whom MRI not done.
The obstetrical outcomes studied.
• Peripartum maternal morbidity and mortality
• ICU admission
• Preterm delivery The neonatal outcomes studied
• Admission to the neonatal intensive care unit
• Perinatal mortality
• Prematurity
RESULTS
• Majority cases of Posterior Reversible Encephalopathy Syndrome seen during period of early 3rd decade of life with an average of 21yr.
• Majority of patients (approximately 66.6%) develop Posterior Reversible Encephalopathy Syndrome during their 1st pregnancy.
• Antenatal patients are more likely (approximately 55.5% among all patients) to develop Posterior Reversible Encephalopathy Syndrome.
• Posterior Reversible Encephalopathy Syndrome has inverse relationship with socioeconomic status.
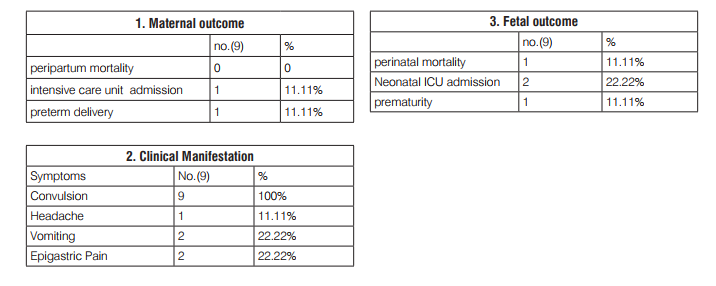
• All patients had convulsions with average of 3-4 times and alteration of sensations.
• Approximately 11% patients had c/o headache and 22% patients had c/o vomiting and epigastric Pain.
• Approximately 66% patients were conscious. Whereas 34% patients were Unconscious.
• Average Systolic Blood pressure was 160 mm hg and Average Diastolic Blood Pressure was 98 mm hg among all cases of Posterior Reversible Encephalopathy Syndrome.
• Approximately 22% chances of preterm delivery and Neonatal ICU admission of new born. Rate of perinatal mortality of new born is 11%.
Alteration of Renal Functions and Liver Functions was seen in 22% cases which was not so significant.
• Approximately 11% cases needs intensive care unit support to maintain O2 saturation and treatment of pulmonary Oedema. Although no mortality recorded because of early diagnosis and treatment.
DISCUSSION
• Risk of development of Posterior Reversible Encephalopathy Syndrome decreases as parity, socioeconomic status and age increases. Among various clinical features all patients develop convulsion and alteration of sensations. Minority develops nausea, vomiting and unconsciousness.
• Pregnancy Induced Hypertension has direct relationship with Posterior Reversible Encephalopathy Syndrome.
• Posterior Reversible Encephalopathy Syndrome itself not causes alterations of liver and renal functions and it’s not necessary to have altered liver and renal functions to develop Posterior Reversible Encephalopathy Syndrome.
• Posterior Reversible Encephalopathy Syndrome increases morbidity of obstetric patients and itself not so fatal if diagnosed and treated earlier. So not causes maternal mortality. As a part of its treatment, Termination of pregnancy is needed which increases preterm delivery and also morbidity and mortality of newborns.
CONCLUSION
Posterior Reversible Encephalopathy Syndrome seen more commonly in primigravida antenatal patients during third decade of their life. Though Posterior Reversible Encephalopathy Syndrome increases maternal morbidity, no maternal mortality reported. In Posterior Reversible Encephalopathy Syndrome patients there are increased incidences of unconciousness, caesarean section, intensive care unit admissions (peripartum morbidity), preterm delivery (Neonatal ICU admission) and perinatal mortality.
LIMITATIONS
It is not possible to do MRI of all patients with eclampsia. So as we cannot judge how many percent of Eclampsia patients will develop Posterior Reversible Encephalopathy Syndrome.
ACKNOWLEDGMENT
This Research paper is made possible through the immense help and support from my Professors, Senior, Hospital staffs and Friends. First and foremost, I would like to thank GOD for his unconditional guidance as I make my Research. Second, I would like to thank my Professors for their most support and encouragement for giving me this research. Finally, I sincerely thank to my Senior and Friends who advised and helped me to complete this research paper.
References:
1. Bartynski WS (2008) Posterior reversible encephalopathy syndrome, part 1: fundamental imaging and clinical features. AJNR Am J Neuroradiol 29: 1036–1042.
2. Bartynski WS (2008) Posterior reversible encephalopathy syndrome, part 2: controversies surrounding pathophysiology of vasogenic oedema. AJNR Am J Neuroradiol 29: 1043–1049.
3. Hinchey J, Chaves C, Appignani B, et al (1996) A reversible posterior leukoencephalopathy syndrome. N Engl J Med 334: 494–500.
4. McKinney AM, Short J, Truwit CL, et al (2007) Posterior reversible encephalopathy syn- drome: incidence of atypical regions of involvement and imaging findings. AJR Am J Roentgenol 189: 904–912.
5. Schwartz RB, Bravo SM, Klufas RA, et al (1995) Cyclosporine neurotoxicity and its rela- tionship to hypertensive encephalopathy: CT and MR findings in 16 cases. AJR Am J Roentgenol 165: 627–631.
6. Casey SO, Sampaio RC, Michel E, Truwit CL (2000) Posterior reversible encephalopathy syndrome: utility of fluid-attenuated inversion recovery MR imaging in the detection of cortical and subcortical lesions. AJNR Am J Neuroradiol 21: 1199–1206.
7. Lee VH, Wijdicks EF, Manno EM, Rabinstein AA (2008) Clinical spectrum of reversible posterior leukoencephalopathy syndrome. Arch Neurol 65: 205–210.
8. Burnett MM, Hess CP, Roberts JP, Bass NM, Douglas VC, Josephson SA (2010) Presenta- tion of reversible posterior leukoencephalopathy syndrome in patients on calcineurin inhibitors. Clin Neurol Neurosurg 112: 886–889.
9. Servillo G, Striano P, Striano S, et al (2003) Posterior reversible encephalopathy syndrome (PRES) in critically ill obstetric patients. Intensive Care Med 29: 2323–2326.
10. Kozak OS, Wijdicks EF, Manno EM, Miley JT, Rabinstein AA (2007) Status epilepticus as initial manifestation of posterior reversible encephalopathy syndrome. Neurology 69: 894–897.
11. Bartynski WS, Boardman JF (2007) Distinct imaging patterns and lesion distribution in posterior reversible encephalopathy syndrome. AJNR Am J Neuroradiol 28: 1320–1327.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





