IJCRR - 13(21), November, 2021
Pages: 14-18
Date of Publication: 09-Nov-2021
Print Article
Download XML Download PDF
Management of Diabetic Peripheral Neuropathy Using Ayurvedic Protocol: A Case Report
Author: Naduvathu Vasudevan Anjaly, Mund Jaya Sankar, Mishra Rattna Prava
Category: Healthcare
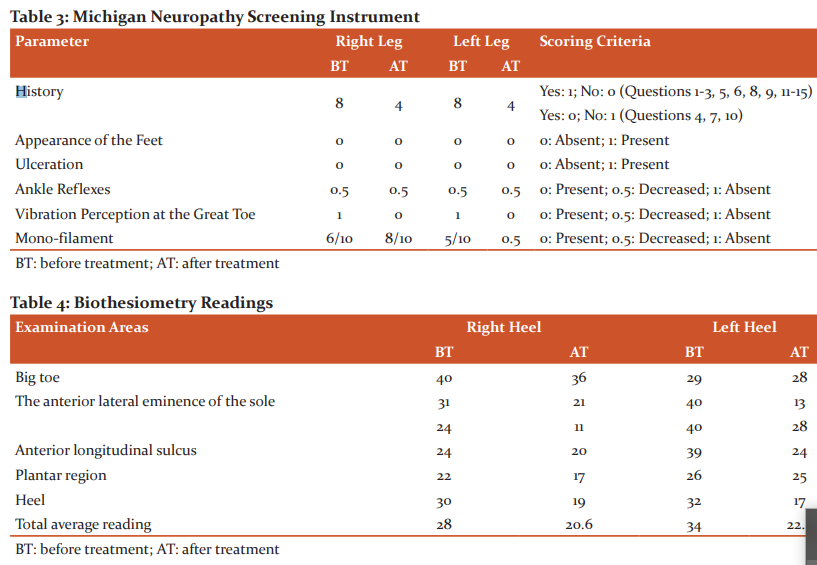
Abstract:Introduction: Diabetic peripheral neuropathy is the most common complication of diabetes, and can occur in all diabetics regardless of the type. Its diagnosis is clinical, with suggestive history and neurologic examination. Altering the natural history and administering symptomatic treatments are the hallmark of management, but many systems of medicine tried to target multiple pathways have not shown promising results. Hence, options in Ayurveda may be sought. Case Report: A 49-year-old female patient who presented with numbness over her lower limbs associated with tingling sensation since the past year and who was diagnosed case of diabetic peripheral neuropathy is presented here. She underwent an inpatient treatment protocol, which included oral medicines and external therapies. Results: Michigan Neuropathy Screening Assessment showed a 50% improvement in the history questionnaire and 80 % improvement in physical examination. In the biothesiometry readings, there was an improvement in vibratory perception by 25 % and 50% in right and left leg respectively. Conclusion: This case illustrates the potential of an Ayurvedic treatment protocol to manage peripheral diabetic neuropathy.
Keywords: Ayurveda, Case Report, Diabetic neuropathy, Holistic approach, Prameha, Raktavrita vatam
Full Text:
Introduction
Neuropathies are common in diabetics1 and may result in serious consequences including foot ulcers, amputations, silent myocardial infarctions, and premature death.2 Diabetic peripheral neuropathy primarily involves the distal portion of the longer myelinated and un-myelinated sensory axons, with sparing of motor axons.3 Symptoms encompass numbness, tingling, burning sensation, a sensation of shooting and cutting pain, walking on cotton wool or glass shards, and feeling of either heat or cold. Conservative management in peripheral diabetic neuropathy aims at symptom relief. The efficacy of an Ayurvedic treatment protocol to manage peripheral diabetic neuropathy in a 49-year-old female with gestational diabetes is presented here. The report adheres to the Case Report (CARE) Guidelines to ensure efficacy and transparency in reporting.4 Institutional ethics committee clearance was not required; however, written informed consent was obtained from the patient before writing her case.
Case Report
In 2015, the patient started experiencing occasional pricking pain in the plantar aspect of both feet. She initially ignored it, but the condition gradually worsened to the point where she started having severe burning sensations, numbness, and tingling sensations. She consulted her allopathic diabetologist for the above and he diagnosed it as Diabetic peripheral neuropathy and prescribed Remylin D tablets. She developed altered sensations in both feet four months ago. She approached Sreedhareeyam Eye Hospital for management of glaucoma, which was diagnosed three months previously, and was offered treatment for both glaucoma and peripheral diabetic neuropathy. She had developed gestational diabetes during her second pregnancy 20 years before. She has been using insulin for ten years (30 units in the morning and 10 in the evening). Her father is a known case of diabetes mellitus. Bowel, appetite, micturition, and sleep were normal. Cardiovascular, gastrointestinal, and central nervous systems; and all vital signs were normal.
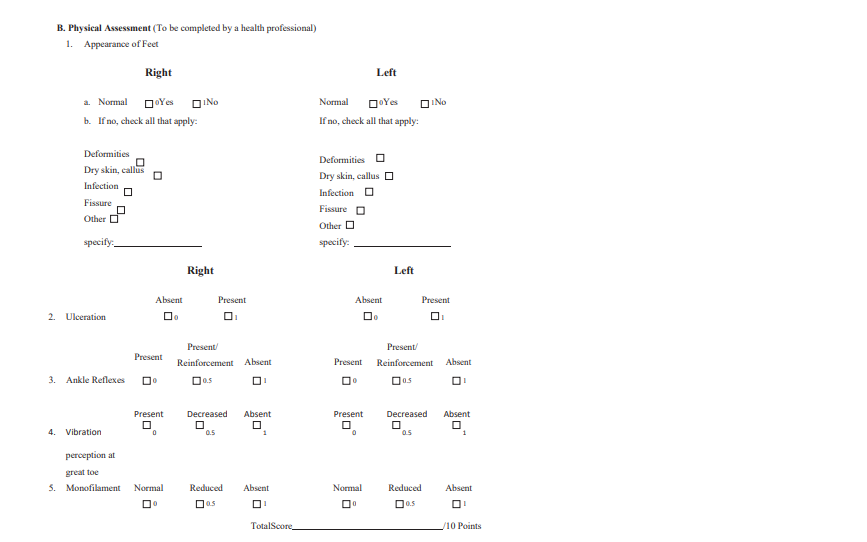
The examination demonstrated feet devoid of deformities, dry skin, callus, infections, and fissures; absence of ulceration, decreased ankle reflexes, absent vibration perceptions at the great toes. Monofilament examination is a noninvasive examination to test the sensitivity to touch. It is measured by using a thin strand of nylon, which is applied perpendicular to skin in 10 areas of each foot. Biothesiometry, done on six specific areas of both heels, viz., big toe, anterior lateral eminences of the sole on both sides, anterior longitudinal sulcus, plantar region, and heel, demonstrated severe loss of vibratory perception, the mean being 28 volts and 34 volts in right and left foot respectively. Laboratory investigations showed an HbA1c of 6.4%, fasting blood glucose level of 174mg/dL, and post-prandial blood glucose level of 291mg/dL.
The Ayurvedic assessment demonstrated that the patient was MadhyamaVaya (middle age), Kapha-Vata Prakriti (somatic constitution of Kapha and Vata), and Madhyama (moderate) Samhanana (compactness of body parts), Pramana (measurement), Sattva (psyche), Satmya (habituation), Ahara Sakti (digestion), and Vyayama Sakti (exercise capacity). The disease was explored along the lines of Prameha Upadrava (complications of diabetes mellitus) based on her symptoms.
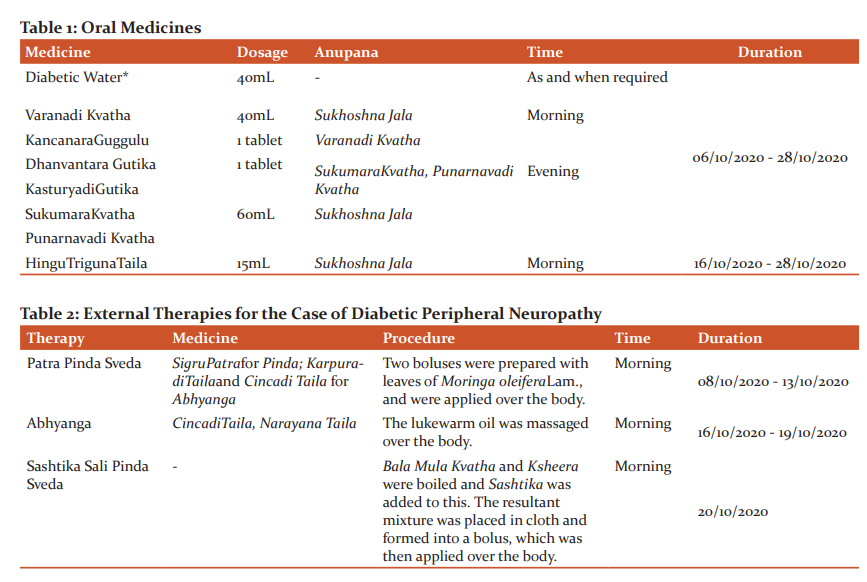
A COVID-19 reverse-transcription polymerase chain reaction (RTPCR) test done before IP admission turned out to be negative. Her course of inpatient Ayurvedic treatment comprised of oral medicines (Table 1) and external therapies (Table 2). Pancakarma (bio-purification) was not attempted due to the severity of the case. She was also placed on a strict dietary regime amounting to a total calorie intake of 1600 Kcal/day, which included regular mild-to-moderate exercise and intake of leafy vegetables, pulses, skimmed milk, and other healthy items; and abstinence from sweet, deep-fried, and starchy foods and products prepared from refined grains. Insulin administration as per dose and time was also adhered to.
Assessment before and after treatments was done with the Michigan Neuropathy Screening Instrument (MNIS), 5 biothesiometry readings, and laboratory investigations. Improvements in MNSI scores were noted. (Table 3) Biothesiometry readings improved to a stage where a moderate loss of vibratory perception was observed (20.6 and 22.5 volts in right and left foot respectively). (Table 4) FBS taken on October 13th, 2020 showed improvement to 144mg/dL. FBS and PPBS taken on 25th October, 2020 improved to 140mg/dL and 207mg/dL respectively.
Diabetic Powder* (2 tablespoons boiled in 1L of water and taken intermittently after filtering), PrabhanjanaVimardanaTailaand Sahacaradi Taila (application 1/2 hour before bath), Varanadi Kvatha and Indukanta Kvatha (10mL of each decoction boiled in 45mL boiled and cooled water and taken twice a day before food), Dhanvantara Gutika (1 tablet powdered and added to the decoctions), and VaraChurna (1 teaspoon of powder with hot water 1/2 hour after dinner) were prescribed at discharge, along with instructions to adhere to a strict diabetic diet and perform regular mild-to-moderate exercise daily.
All medicines were manufactured at Sreedhareeyam Farmherbs India, Pvt. Ltd., the hospital’s GMP-certified manufacturing unit.
Discussion
Diabetes mellitus is considered as Prameha as per Ayurveda, and is placed among the eight dreadful conditions (Ashta Mahagada), viz., Vatavyadhi (neurological diseases), Asmari (renal calculus), Kushta(obstinate skin disorders), Meha (obstinate urinary disorders including diabetes mellitus), Udara(abdominal enlargement), Bhagandara (fistula-in-ano), Arsas (haemorrhoids), and Grahani (irritable bowel).6 All varieties of Meha, if untreated, progress to Madhumeha, which is Asadhya (incurable).
The probable Nidanas observed in this patient were overindulgence in foods that were Guru (heavy), Snigdha (unctuous), Sita (cold), and Picchila (slimy) by nature. These resulted in Dhatvagnimandya (impaired digestion at the level of the tissues), which in turn lead to the production of Ama (undigested, toxic waste). The weakened Agni was not able to produce proper Anna Rasa (the essence of food). Dhatvagnimandya of Medas (adipose tissue) failed nourishment of the other Dhatus, viz., Asthi (bone), Majja (marrow), and Sukra (seminal fluid), resulting in their Kshaya (decrease). This Kshaya was manifested in the form of neuropathy and other consequences of diabetes mellitus.
The Rukshata (dryness) in the patient’s body as a result of increased Vata caused a failed vasodilator mechanism that altered the functions of endoneural and epineural blood vessels. Sensory disturbances in this patient were caused by affected Rakta Dhatu (blood tissue), It also resulted in Dhamani Praticaya (hardening of vessels), a Nanatmaja Vikara of Kapha, as evidenced by microangiopathy.
Pricking pain in this patient was significant of Sucibhiriva Tudyate (feeling of pins and needles), which is a Lakshana of Sonitavrta Vata described by Acarya Susruta7 and Majjavrta Vata described by Acarya Caraka.8 Tingling sensation is indicative of Cumcumayana, a feature of Sonitavrta Vata told by Acarya Susruta; Harsha Lomaharsha, a feature of Tvaggata Vata as per Susruta and Pittavrta Samana Vata told by Caraka. The burning sensation is indicative of Daha, a Purvarupaand Upadrava of Prameha told in Caraka SamhitaNidanaSthana; Vidaha, a NanatmajaVikara told by Caraka; Plosha, a NanatmajaVikaraof Pitta explained by AshtangaSangraha; and Pariplosha, a Lakshanaof KaphaKshaya and RaktaMedogata Pitta as per AshtangaSangraha, and a Upadrava of Pittaja Prameha as per Susruta. The numbness was indicative of Supti, a Purvarupaof Prameha as per Caraka Samhita Nidana Sthana. Abnormal perceptions of pain were indicative of Toda, a Lakshana ofVyanavrtaPrana told by Caraka; Sula, a Lakshanaof Prameha Upadrava told by Susruta Samhita Nidana Sthana; and Bheda, a NanatmajaVikaraof Vata.
Based on the above, the treatment protocol was adopted to reduce Prameha and to nourish the nerves. The common properties of the oral medications are Kapha-Vata Samana (pacifying Kapha and Vata), Dipana (appetizing). Pacana (digestive), SrotoSodhana(channel-cleansing), and Lekhana (scarifying). Excess Snigdha(unctuous), Manda (slow), and Picchila(slimy) qualities were avoided as the Kapha Dosha was pathologically active. The medicines possess antioxidant, antibacterial, and anti-diabetic properties, which helped to re-establish homeostasis and metabolism, and supply nutrition to the nerves.
The external therapies were aimed at normalizing Vata. Patra Pinda Sveda enhanced vasodilation and promote the activity of the parasympathetic nervous system by its Ushna (hot) property. The Sukshma (minute) and Sara (fluid) properties enabled dislodging of the adherent Doshas and expelling through the pores of the skin as sweat. The use of Saindhavaand JambiraSvarasa enhanced its absorption into the skin and propelled it to dislodge adherent Doshas. Abhyanga further enhanced vasodilation and transport of nutrients by its application of pressure and motion. The medicines used for Abhyangawere Vataharaby nature. Sashtika Sali Pinda Sveda not only stimulated Vata but also nourished the nervous system. The combined effects of the external therapies enhanced nervous activity, stimulated the peripheral nervous system, and enhanced sensitivity, as documented in the biothesiometry readings.
The strict dietary regime was to lower serum glucose, minimize carbohydrates, and restore metabolism. Equal and spaced portions from each of the main food groups were essential to balance the amounts of carbohydrates, vitamins, minerals, and nutrients.
Conclusion
A concerted effort by the oral medicines, external therapies, and dietary regime yielded positive results in the patient. At the time of discharge, biothesiometry readings improved and the MNIS showed more positive results. Management of Meha may always be a challenge, but concerted efforts by the physician, medicine, attendants, and physicians, the four limbs of treatment, result in positive outcomes. The results obtained in this report may be analyzed and validated by large-scale sample trials.
Acknowledgement:
The authors thank Sreedhareeyam Ayurvedic Eye Hospital and Research Center, and Sreedhareeyam Farmherbs India Pvt. Ltd., for their help in preparing this case report. The authors acknowledge the immense help received from the scholars whose articles are cited and included in references to this manuscript. The authors are also grateful to the authors/editors/publishers of all those articles, journals, and books from where the literature for this article has been reviewed and discussed.
Source of Funding:
No financial interests (stocks, patents, employment, honoraria, or royalties) or nonfinancial relationships (political, personal, or professional) that may be interpreted as influential toward the content of this manuscript are declared as well.
Conflict of Interest: None declared.
Authors’ Contribution:
-
Anjaly Naduvathu Vasudevan collected and analyzed the data and prepared the report.
-
Jaya Sankar Mundanalyzed the data and reviewed the article.
-
RatnaPravaMisraanalyzed the data and reviewed the article.
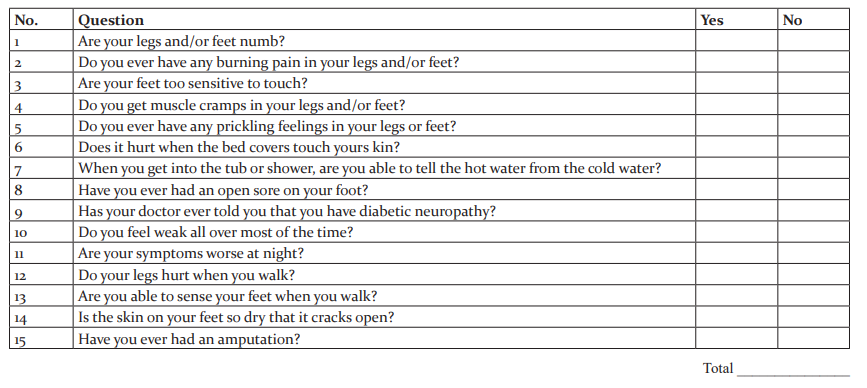
Annexure: The Michigan Neuropathy Screening Instrument
Part A: History (to be completed by the patient of diabetes)
Please take a few minutes to answer the following questions about the feeling in your legs and feet. Check ‘yes’ or ‘no’ based on how you feel. Thank you.
References:
-
Dyck PJ, Kratz KM, Karnes JL(1993) The prevalence by staged severity of various types of diabetic neuropathy, retinopathy and nephropathy in a population-based cohort: the Rochester Diabetic Neuropathy Study. Neurol. 43: 817-824
-
Boulton AJ, Vinik AI, Arezzo JC (2005) Diabetic neuropathies: a statement by the American Diabetes Association. Diabetes Care 28: 956-962
-
Malik RA, Tesfaye S, Newrick PG (2005) Sural nerve pathology in diabetic patients with minimal but progressive neuropathy. Diabetol. 48: 578-585
-
Gagnier J, Kienle G, Altman DG, Moher D, Sox H, Riley DS, CARE group, The CARE guidelines: Consensus-based clinical case-reporting guideline development. Global Advances in Health Med. 2013; 2(5):38-43
-
Feldman EL, Stevens MJ, Thomas PK, Brown MB, Canal N, Greene DA. A practical two-step quantitative clinical and electrophysiological assessment for the diagnosis and staging of diabetic neuropathy. Diabetes Care. 1994;17:1281-89
-
Murthy KRS, editor, (2nded.). Ashtanga Samgraha of Vagbhata, NidanaSthana;Atisara-GrahanidoshaNidana: Chapter 8, Verse 33. Varanasi: Chaukhambha Sanskrit Series Office, 1999; 197.
-
Sharma PV, editor, (1sted.).Susruta Samhita: With English Translation of Text and Dalhana’s Commentary along with Critical Notes, Vol. II, Nidana Sthana: VatavyadhiNadana, Chapter 1, Verse 33. Varanasi: ChaukhambhaVishwabharati, Reprint 2005; 9.
-
Sharma RK, Dash B, (1sted.). Caraka Samhita: Text with English Translation and Critical Exposition based on Cakrapanidatta’s Ayurveda Dipika: Vol. 5, Cikitsa Sthana, Vatavyadhi Cikitsa, Chapter 28, Verse 67, Varanasi: Chaukhambha Vishwabharati, Reprint 2013; 39 .
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





